

- •Contents
- •Preface
- •Contributors
- •1 Vessels
- •1.1 Aorta, Vena Cava, and Peripheral Vessels
- •Aorta, Arteries
- •Anomalies and Variant Positions
- •Dilatation
- •Stenosis
- •Wall Thickening
- •Intraluminal Mass
- •Perivascular Mass
- •Vena Cava, Veins
- •Anomalies
- •Dilatation
- •Intraluminal Mass
- •Compression, Infiltration
- •1.2 Portal Vein and Its Tributaries
- •Enlarged Lumen Diameter
- •Portal Hypertension
- •Intraluminal Mass
- •Thrombosis
- •Tumor
- •2 Liver
- •Enlarged Liver
- •Small Liver
- •Homogeneous Hypoechoic Texture
- •Homogeneous Hyperechoic Texture
- •Regionally Inhomogeneous Texture
- •Diffuse Inhomogeneous Texture
- •Anechoic Masses
- •Hypoechoic Masses
- •Isoechoic Masses
- •Hyperechoic Masses
- •Echogenic Masses
- •Irregular Masses
- •Differential Diagnosis of Focal Lesions
- •Diagnostic Methods
- •Suspected Diagnosis
- •3 Biliary Tree and Gallbladder
- •3.1 Biliary Tree
- •Thickening of the Bile Duct Wall
- •Localized and Diffuse
- •Bile Duct Rarefaction
- •Localized and Diffuse
- •Bile Duct Dilatation and Intraductal Pressure
- •Intrahepatic
- •Hilar and Prepancreatic
- •Intrapancreatic
- •Papillary
- •Abnormal Intraluminal Bile Duct Findings
- •Foreign Body
- •The Seven Most Important Questions
- •3.2 Gallbladder
- •Changes in Size
- •Large Gallbladder
- •Small/Missing Gallbladder
- •Wall Changes
- •General Hypoechogenicity
- •General Hyperechogenicity
- •General Tumor
- •Focal Tumor
- •Intraluminal Changes
- •Hyperechoic
- •Hypoechoic
- •Nonvisualized Gallbladder
- •Missing Gallbladder
- •Obscured Gallbladder
- •4 Pancreas
- •Diffuse Pancreatic Change
- •Large Pancreas
- •Small Pancreas
- •Hypoechoic Texture
- •Hyperechoic Texture
- •Focal Changes
- •Anechoic Lesion
- •Hypoechoic Lesion
- •Isoechoic Lesion
- •Hyperechoic Lesion
- •Irregular (Complex Structured) Lesion
- •Dilatation of the Pancreatic Duct
- •Marginal/Mild Dilatation
- •Marked Dilatation
- •5 Spleen
- •Nonfocal Changes of the Spleen
- •Diffuse Parenchymal Changes
- •Large Spleen
- •Small Spleen
- •Focal Changes of the Spleen
- •Anechoic Mass
- •Hypoechoic Mass
- •Hyperechoic Mass
- •Splenic Calcification
- •6 Lymph Nodes
- •Peripheral Lymph Nodes
- •Head/Neck
- •Extremities (Axilla, Groin)
- •Abdominal Lymph Nodes
- •Porta Hepatis
- •Splenic Hilum
- •Mesentery (Celiac, Upper and Lower Mesenteric Station)
- •Stomach
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •Small/Large Intestine
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •8 Peritoneal Cavity
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Wall Structures
- •Smooth Margin
- •Irregular Margin
- •Intragastric Processes
- •Intraintestinal Processes
- •9 Kidneys
- •Anomalies, Malformations
- •Aplasia, Hypoplasia
- •Cystic Malformation
- •Anomalies of Number, Position, or Rotation
- •Fusion Anomaly
- •Anomalies of the Renal Calices
- •Vascular Anomaly
- •Diffuse Changes
- •Large Kidneys
- •Small Kidneys
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Irregular Structure
- •Circumscribed Changes
- •Anechoic Structure
- •Hypoechoic or Isoechoic Structure
- •Complex Structure
- •Hyperechoic Structure
- •10 Adrenal Glands
- •Enlargement
- •Anechoic Structure
- •Hypoechoic Structure
- •Complex Echo Structure
- •Hyperechoic Structure
- •11 Urinary Tract
- •Malformations
- •Duplication Anomalies
- •Dilatations and Stenoses
- •Dilated Renal Pelvis and Ureter
- •Anechoic
- •Hypoechoic
- •Hypoechoic
- •Hyperechoic
- •Large Bladder
- •Small Bladder
- •Altered Bladder Shape
- •Intracavitary Mass
- •Hypoechoic
- •Hyperechoic
- •Echogenic
- •Wall Changes
- •Diffuse Wall Thickening
- •Circumscribed Wall Thickening
- •Concavities and Convexities
- •12.1 The Prostate
- •Enlarged Prostate
- •Regular
- •Irregular
- •Small Prostate
- •Regular
- •Echogenic
- •Circumscribed Lesion
- •Anechoic
- •Hypoechoic
- •Echogenic
- •12.2 Seminal Vesicles
- •Diffuse Change
- •Hypoechoic
- •Circumscribed Change
- •Anechoic
- •Echogenic
- •Irregular
- •12.3 Testis, Epididymis
- •Diffuse Change
- •Enlargement
- •Decreased Size
- •Circumscribed Lesion
- •Anechoic or Hypoechoic
- •Irregular/Echogenic
- •Epididymal Lesion
- •Anechoic
- •Hypoechoic
- •Intrascrotal Mass
- •Anechoic or Hypoechoic
- •Echogenic
- •13 Female Genital Tract
- •Masses
- •Abnormalities of Size or Shape
- •Uterus
- •Abnormalities of Size or Shape
- •Myometrial Changes
- •Intracavitary Changes
- •Endometrial Changes
- •Fallopian Tubes
- •Hypoechoic Mass
- •Anechoic Cystic Mass
- •Solid Echogenic or Nonhomogeneous Mass
- •14 Thyroid Gland
- •Diffuse Changes
- •Enlarged Thyroid Gland
- •Small Thyroid Gland
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Circumscribed Changes
- •Anechoic
- •Hypoechoic
- •Isoechoic
- •Hyperechoic
- •Irregular
- •Differential Diagnosis of Hyperthyroidism
- •Types of Autonomy
- •15 Pleura and Chest Wall
- •Chest Wall
- •Masses
- •Parietal Pleura
- •Nodular Masses
- •Diffuse Pleural Thickening
- •Pleural Effusion
- •Anechoic Effusion
- •Echogenic Effusion
- •Complex Effusion
- •16 Lung
- •Masses
- •Anechoic Masses
- •Hypoechoic Masses
- •Complex Masses
- •Index
13 Female Genital Tract
Female Genital Tract 441
|
Vagina |
??? |
442 |
|||||
|
||||||||
|
|
|
|
|
Masses |
442 |
||
|
|
|
|
|
||||
|
|
|
|
|
|
|
Imperforate Hymen |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
with Hematocolpos |
|
|
|
|
|
|
|
|
Vaginal Wall Cyst |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Double Vagina, Septate Vagina |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Tampon |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Vaginal Carcinoma |
|
|
|
|
|
|
Abnormalities of Size or Shape |
444 |
||
|
|
|
|
|
||||
|
|
|
|
|
|
|
Postoperative Changes |
|
|
|
|
Uterus |
??? |
444 |
|||
|
|
|
|
Abnormalities of Size or Shape |
446 |
|||
|
|
|
|
|||||
|
|
|
|
|
|
|
Uterine Prolapse |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Malformations |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Uterine Aplasia, Atresia |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Uterine Hypoplasia, |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Small Uterus |
|
|
|
|
|
|
|
|
Hemangioma, Lymphoma, |
|
|
|
|
|
|
|
|
Angiomyoma, Myoma |
|
|
|
|
|
Myometrial Changes |
447 |
|||
|
|
|
|
|||||
|
|
|
|
|
|
|
Uterine Myomas |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Uterine Adenomyomatosis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Uterine Sarcoma |
|
|
|
|
|
Intracavitary Changes |
451 |
|||
|
|
|
|
|||||
|
|
|
|
|
|
|
Foreign Body (IUD) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mucocele, Serometra, |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pyometra, Hematometra |
|
|
|
|
|
|
|
|
Pregnancy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Ectopic Pregnancy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Missed Abortion, |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Incomplete Abortion, |
|
|
|
|
|
|
|
|
Cervical Pregnancy |
|
|
|
|
|
|
|
|
Endometrial Polyps, Cervical |
|
|
|
|
|
|
|
|
Polyps, Placental Polyps |
|
|
|
|
|
|
Endometrial Changes |
454 |
||
|
|
|
|
|
||||
|
|
|
|
|
|
|
Menstrual Cycle: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Proliferative Endometrium |
|
|
|
|
|
|
|
|
Cystic Glandular and |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Atypical Adenomatous |
|
|
|
|
|
|
|
|
Hyperplasia |
|
|
|
|
|
|
|
|
Endometritis, Cervicitis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Corpus Carcinoma |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Chorioepithelioma |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cervical Carcinoma |
|
|
Fallopian Tubes417 |
458 |
||||||
|
||||||||
|
|
|
|
|
Hypoechoic Mass |
458 |
||
|
|
|
|
|
||||
|
|
|
|
|
|
|
Sactosalpinx, Hematosalpinx, |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pyosalpinx |
|
|
|
|
|
|
|
|
Tubal Carcinoma |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Benign Tumors |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Tubal Pregnancy |
|
|
|
|
Ovaries |
xxx |
460 |
|||
|
|
|||||||
|
|
|
|
Anechoic Cystic Mass |
461 |
|||
|
|
|
|
|||||
|
|
|
|
|
|
|
Simple Follicles |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Functional Cysts (Follicular and |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Corpus Luteum Cysts) |
|
|
|
|
|
|
|
|
Theca-Lutein Cyst |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Paraovarian Cyst |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Polycystic Ovaries (PCO Syndrome, |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
Stein–Leventhal Syndrome) |
|
|
|
|
|
|
|
|
Cystic Ovarian Tumors |
|
|
|
|
|
|
Solid Echogenic or |
|
||
|
|
|
|
|
|
|||
|
|
|
|
Nonhomogeneous Mass |
464 |
|||
|
|
|
|
|
|
|
|
|
Endometriotic Cysts
Thecomatosis
Inflammatory Adnexal Mass
Ovarian Carcinoma
Metastases
Pseudomyxoma Peritonei
Ovarian Tumors
(by Histological Criteria)

13Female Genital Tract
B. Beuscher-Willems
Transabdominal ultrasound. Transabdominal scanning of the lower abdomen should be done for screening purposes as part of every abdominal ultrasound examination. The use of ultrasonography in gynecology was first described by Donald in 1958.1 Today, transvaginal sonography has become the procedure of first choice for gynecological investigations. The short penetration depth permits the use of a higher-frequency transducer, which provides higher resolution and more detailed images. Transvaginal sonography has been practiced since about 1985.
Transabdominal ultrasound is still important in gynecology, especially as an adjunct to transvaginal scanning, in defining the boundaries and extent of large masses. With its greater penetration depth, transabdominal ultrasound
Table 13.1 Indications for transabdominal ultrasound scanning in gynecology
●Urinary stasis
●Tumor screening
●Defining the extent of large tumors
●Follow-ups
●Positional anomalies
●Intact hymen
●Vaginal stenosis
●Refusal of transvaginal sonography
●Lower abdominal pain
is also useful for evaluating positional anomalies. Other indications for transabdominal scanning exist in patients with an imperforate hymen or vaginal stenosis, or patients who refuse transvaginal ultrasound (Table 13.1).
Unclear findings in the transabdominal scan cannot always be resolved by the transvaginal scan and require laparoscopy, invasive exploration, and excision.
Appearance of the genital tract. The physiological appearance of the female genital tract varies with hormonal changes relating to the menstrual cycle and to age. The sex hormones (estrogens, progestins, androgens) are produced in the ovaries, and ovarian function is regulated by means of a feedback control loop (hypothalamus [gonadotropin-releasing hor-
Periods of Life in the Female
●Neonatal period, initially still influenced by maternal hormones
●Childhood
●Puberty, including premenarche and postmenarche and marked by increasing ovarian function
●Adolescence, marked by feminization
mone = GnRH] → anterior pituitary [gonadotropins] → ovary [sex hormones]). The gonadotropins (follicle-stimulating hormone, FSH; luteinizing hormone, LH; and prolactin, PRL) are synthesized in the anterior lobe of the pituitary gland.
The likelihood that an abnormal process exists in the female genital tract also depends on the age and hormonal status of the patient. Knowing the patient’s period of life and clinical presentation is essential as part of the overall assessment and in formulating a differential diagnosis. Thus a distinction is drawn between examinations performed before menarche, during the reproductive years, during and after menopause, and in old age.
●Sexual maturity, marked by the onset of fertility and biphasic menstrual cycles
●Menopause, including premenopause with relative estrogenism and luteal insufficiency
●Postmenopause, marked by declining estrogen production
●Old age
Topography 





















































See Figs.13.1, 13.2, 13.3, 13.4, 13.5.
Relations of the genital organs
● Located in the lesser pelvis, predominantly intraperitoneal
● Anterior to the rectum ● Posterior to the bladder
● Medial to the psoas muscle
● Superior and medial to the iliac wings ● Posterior to the pubic bone and
symphysis
Sonographic landmarks
● Bladder
● Rectum
● Internal and external iliac vein
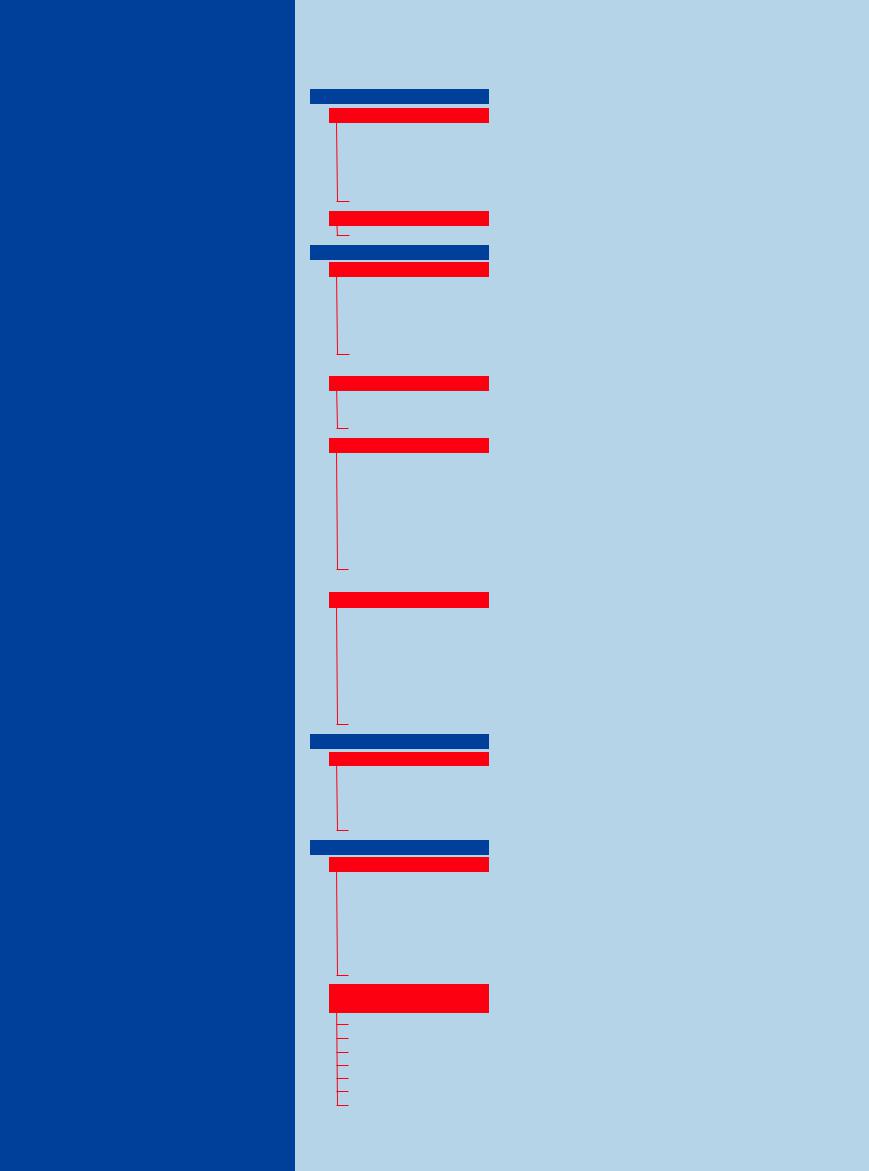
Fig. 13.1 Relations of the female internal genital organs: Fig. 13.2 Longitudinal scan of the uterus (UT) and vagina. vagina, uterus, fallopian tubes, and ovaries.
13
Female Genital Tract
441
13
Female Genital Tract
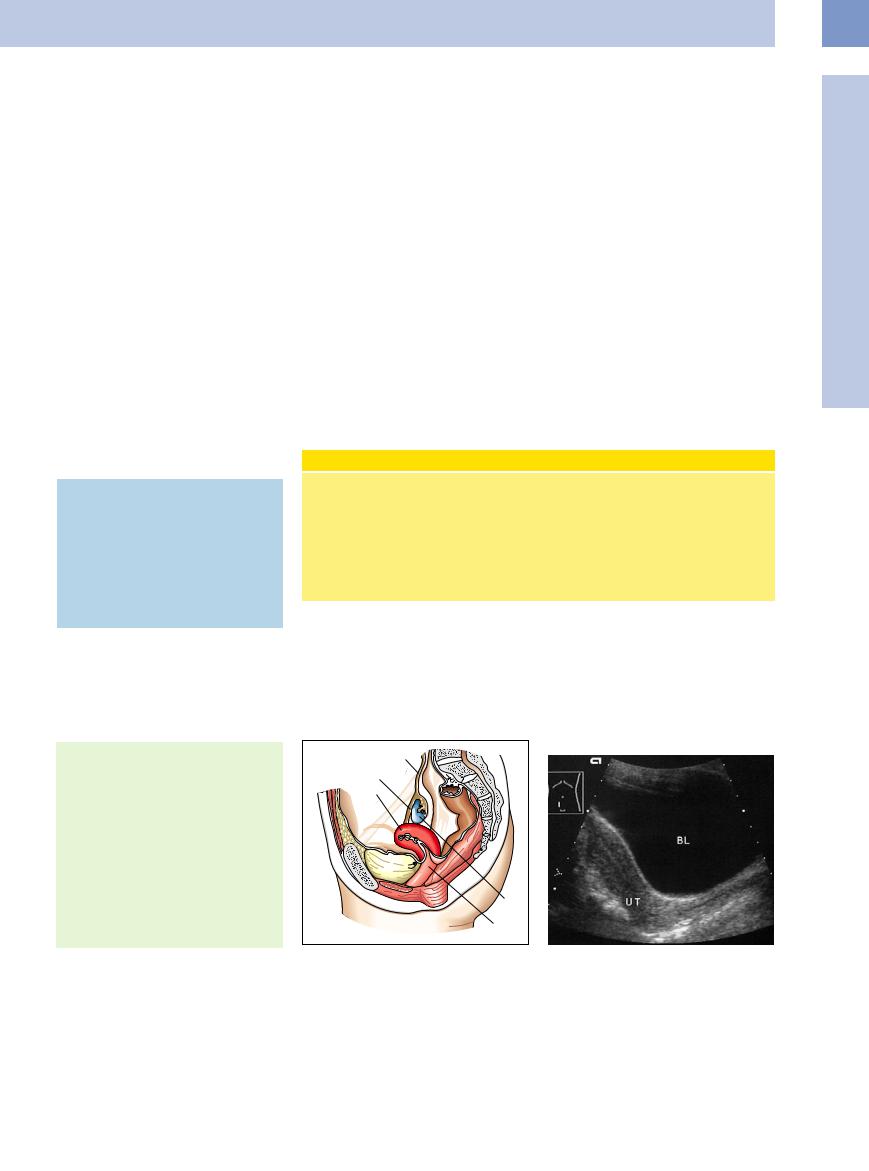
Fig. 13.3 Transverse scan of the uterine fundus: about 4 cm transverse diameter and about 2 cm sagittal diameter. BL = bladder.
Fig. 13.4 Uterine fundus, 29-year-old woman, transverse scan of the lower abdomen: normal echogenicity and size (cursors).
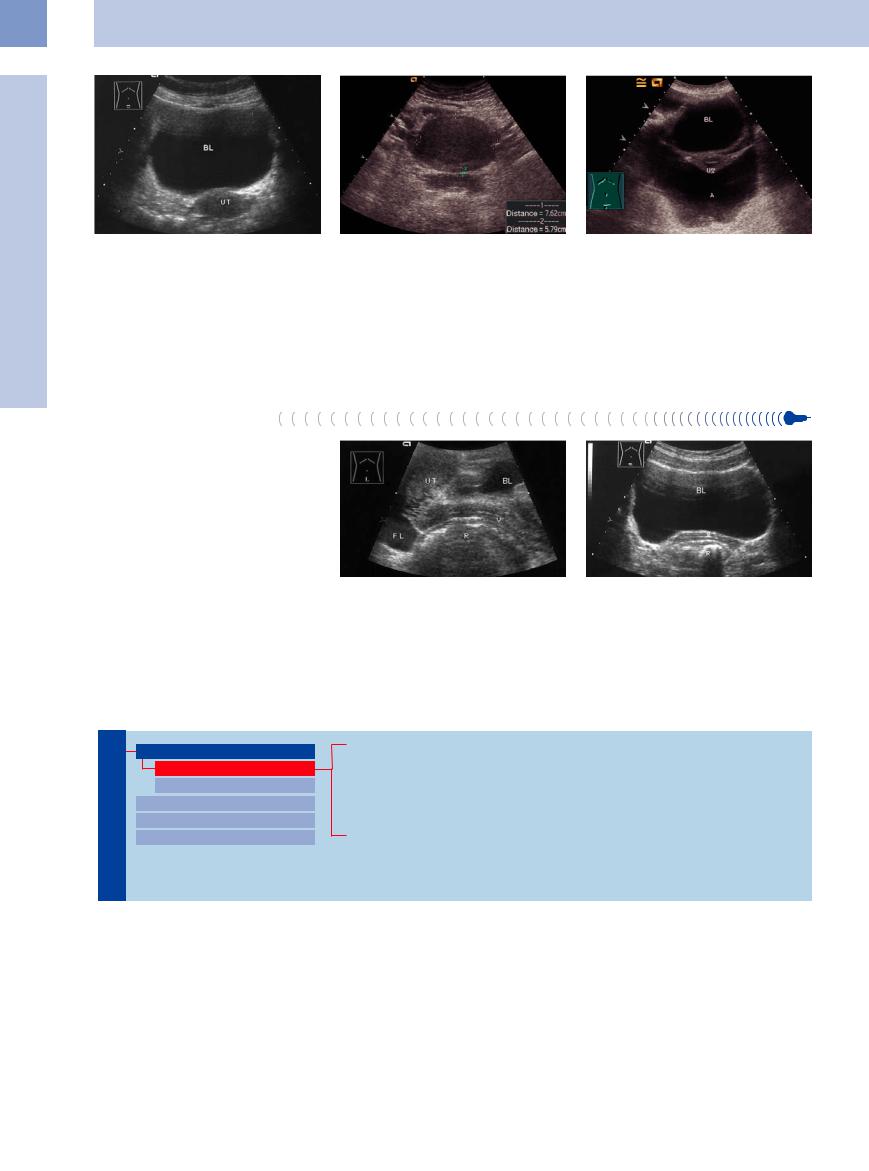
Fig. 13.5 Uterus (UT) in a dorso-inferior position of the bladder (BL), surrounded by ascites (A); also the retinaculi fixing the uterus to the lateral abdominal wall. The central echoic band is formed by the connecting halves of the endometrium.
■ Vagina
Ultrasound Morphology
Morphology
The vagina is a flattened tube leading to the uterus. With its anterior and posterior walls composed of mucosal and muscular layers, the vagina appears as a thin, multilayered band in longitudinal and transverse ultrasound scans through the lower abdomen (Fig.13.6, Fig.13.7). The vagina may appear echogenic to hypoechoic, depending on the angle at which it is scanned. In some cases ultrasound can distinguish a high-level entry echo followed by the hypoechoic anterior wall, a bright luminal echo at the center, the hypoechoic posterior wall, and a bright exit echo. The lumen may also be hypoechoic, depending on the fluid and mucosal content of the vagina.
Masses
Fig. 13.6 Longitudinal scan of the vagina. UT = uterus; BL = bladder; V = vagina; R = rectum; FL = fluid in the cul-de- sac.
Fig. 13.7 Transverse scan of the vagina. BL = bladder; V = vagina; R = rectum.
Female Genital Tract
Vagina Masses
Abnormalities of Size or Shape Uterus
Fallopian Tubes Ovaries
Imperforate Hymen with Hematocolpos Vaginal Wall Cyst
Double Vagina, Septate Vagina Tampon
Vaginal Carcinoma
Imperforate Hymen with
with Hematocolpos
Hematocolpos






































An imperforate hymen is rare (incidence 1/ 60 000) and does not become clinically apparent until puberty. With menarche, the patient experiences monthly lower abdominal pain and increasing malaise with an absence of menstrual bleeding. The blood pools in the vagina (hematocolpos) and may reflux into
the uterus (hematometra) or fallopian tubes (hematosalpinx). The pseudotumor may extend to the level of the umbilicus.
Hematocolpos. Ultrasound demonstrates an almost anechoic mass of variable size and extent in the vagina, located posterior and infe-
rior to the bladder. The uterus, which shows increased echogenicity, is displaced upward and is often barely detectable in its position above the mass (Fig.13.8).
442
13
Hematometra. The blood may back up into the |
Fig. 13.8 Hematocolpos. |
uterus, resulting in an enlarged anechoic mass |
|
posterior to the bladder. |
|
Hematosalpinx. The fallopian tubes may also fill with blood, causing extension of the mass lateral to the bladder (see Fig.13.77).
Vagina
Vaginal Wall Cyst
Cyst 


















































Vaginal wall cysts are remnants of the wolffian duct (mesonephric duct), appearing sonographically as anechoic, smooth-bordered masses located caudal to the bladder. The development of carcinoma in vaginal wall cysts is known to occur.
Double Vagina, Septate Vagina
Vagina











































Malformations are somewhat rare and result from fusion anomalies of the müllerian ducts. In 40% of cases, malformations of the vagina are combined with anomalies of the kidneys and urinary tract.
When a double vagina is scanned with ultrasound, it initially appears thickened with a central, echogenic band. The two hypoechoic lumina can be distinguished when viewed in transverse section. Differentiation from a septate vagina is often difficult.
Only certain vaginal malformations are detectable by transabdominal scanning, and generally it is difficult to evaluate all malformations with ultrasound alone. A gynecological examination and additional tests (hysteroscopy and laparoscopy) are required.
Tampon 























































A tampon appears caudal to the bladder as a very echogenic mass with indistinct margins and a posterior acoustic shadow (Fig.13.9). The nature of the mass is easily determined by questioning the patient.
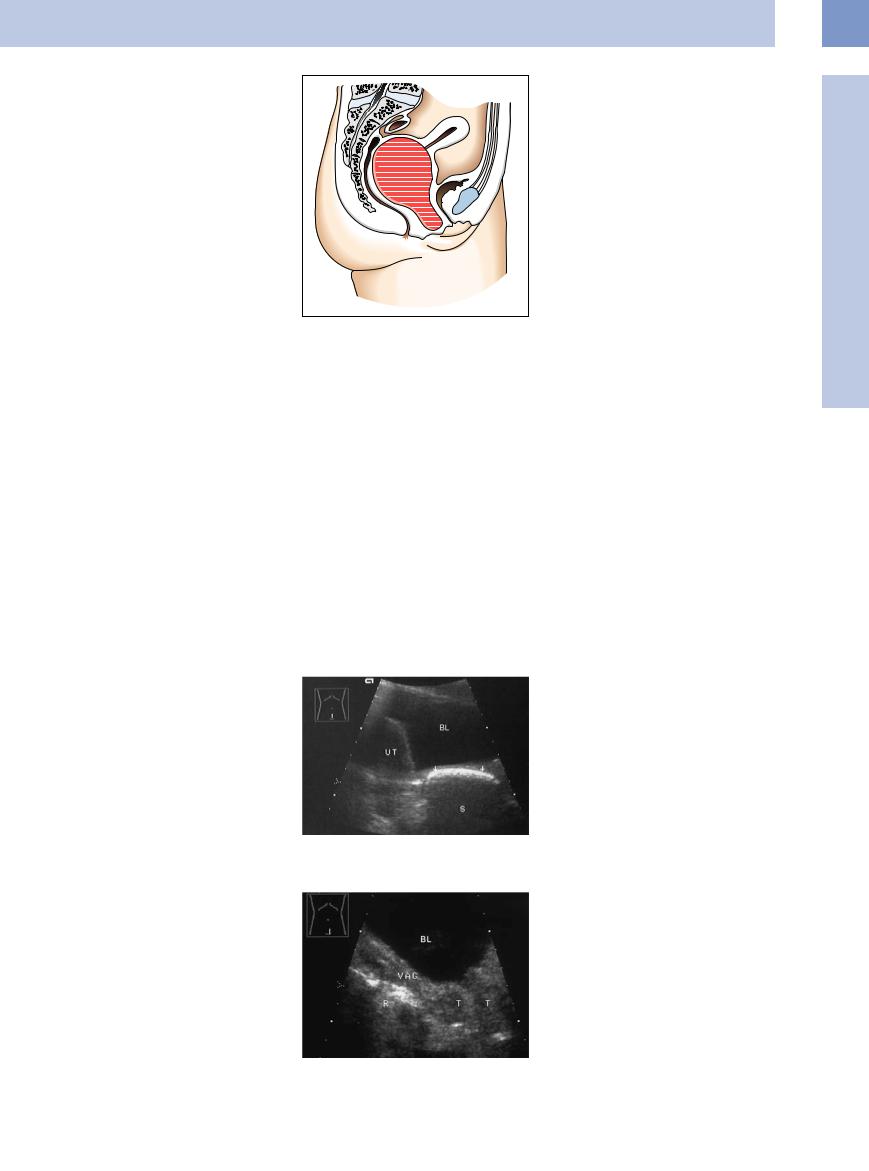
Fig. 13.9 Intravaginal tampon (arrows) appears as an elongated, echogenic mass with an acoustic shadow (S). BL = bladder; UT = uterus.
Vaginal Carcinoma 

















































The most frequent site of occurrence is the posterior fornix. Squamous cell carcinomas are the most common and tend to be locally invasive (rectum, uterus, bladder) and seed locoregional metastases (Fig.13.10).
Fig. 13.10 Vaginal/vulval carcinoma (T): hypoechoic mass infiltrating the rectum (R) and bladder (BL). VAG = vagina.
443