

- •Contents
- •Preface
- •Contributors
- •1 Vessels
- •1.1 Aorta, Vena Cava, and Peripheral Vessels
- •Aorta, Arteries
- •Anomalies and Variant Positions
- •Dilatation
- •Stenosis
- •Wall Thickening
- •Intraluminal Mass
- •Perivascular Mass
- •Vena Cava, Veins
- •Anomalies
- •Dilatation
- •Intraluminal Mass
- •Compression, Infiltration
- •1.2 Portal Vein and Its Tributaries
- •Enlarged Lumen Diameter
- •Portal Hypertension
- •Intraluminal Mass
- •Thrombosis
- •Tumor
- •2 Liver
- •Enlarged Liver
- •Small Liver
- •Homogeneous Hypoechoic Texture
- •Homogeneous Hyperechoic Texture
- •Regionally Inhomogeneous Texture
- •Diffuse Inhomogeneous Texture
- •Anechoic Masses
- •Hypoechoic Masses
- •Isoechoic Masses
- •Hyperechoic Masses
- •Echogenic Masses
- •Irregular Masses
- •Differential Diagnosis of Focal Lesions
- •Diagnostic Methods
- •Suspected Diagnosis
- •3 Biliary Tree and Gallbladder
- •3.1 Biliary Tree
- •Thickening of the Bile Duct Wall
- •Localized and Diffuse
- •Bile Duct Rarefaction
- •Localized and Diffuse
- •Bile Duct Dilatation and Intraductal Pressure
- •Intrahepatic
- •Hilar and Prepancreatic
- •Intrapancreatic
- •Papillary
- •Abnormal Intraluminal Bile Duct Findings
- •Foreign Body
- •The Seven Most Important Questions
- •3.2 Gallbladder
- •Changes in Size
- •Large Gallbladder
- •Small/Missing Gallbladder
- •Wall Changes
- •General Hypoechogenicity
- •General Hyperechogenicity
- •General Tumor
- •Focal Tumor
- •Intraluminal Changes
- •Hyperechoic
- •Hypoechoic
- •Nonvisualized Gallbladder
- •Missing Gallbladder
- •Obscured Gallbladder
- •4 Pancreas
- •Diffuse Pancreatic Change
- •Large Pancreas
- •Small Pancreas
- •Hypoechoic Texture
- •Hyperechoic Texture
- •Focal Changes
- •Anechoic Lesion
- •Hypoechoic Lesion
- •Isoechoic Lesion
- •Hyperechoic Lesion
- •Irregular (Complex Structured) Lesion
- •Dilatation of the Pancreatic Duct
- •Marginal/Mild Dilatation
- •Marked Dilatation
- •5 Spleen
- •Nonfocal Changes of the Spleen
- •Diffuse Parenchymal Changes
- •Large Spleen
- •Small Spleen
- •Focal Changes of the Spleen
- •Anechoic Mass
- •Hypoechoic Mass
- •Hyperechoic Mass
- •Splenic Calcification
- •6 Lymph Nodes
- •Peripheral Lymph Nodes
- •Head/Neck
- •Extremities (Axilla, Groin)
- •Abdominal Lymph Nodes
- •Porta Hepatis
- •Splenic Hilum
- •Mesentery (Celiac, Upper and Lower Mesenteric Station)
- •Stomach
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •Small/Large Intestine
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •8 Peritoneal Cavity
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Wall Structures
- •Smooth Margin
- •Irregular Margin
- •Intragastric Processes
- •Intraintestinal Processes
- •9 Kidneys
- •Anomalies, Malformations
- •Aplasia, Hypoplasia
- •Cystic Malformation
- •Anomalies of Number, Position, or Rotation
- •Fusion Anomaly
- •Anomalies of the Renal Calices
- •Vascular Anomaly
- •Diffuse Changes
- •Large Kidneys
- •Small Kidneys
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Irregular Structure
- •Circumscribed Changes
- •Anechoic Structure
- •Hypoechoic or Isoechoic Structure
- •Complex Structure
- •Hyperechoic Structure
- •10 Adrenal Glands
- •Enlargement
- •Anechoic Structure
- •Hypoechoic Structure
- •Complex Echo Structure
- •Hyperechoic Structure
- •11 Urinary Tract
- •Malformations
- •Duplication Anomalies
- •Dilatations and Stenoses
- •Dilated Renal Pelvis and Ureter
- •Anechoic
- •Hypoechoic
- •Hypoechoic
- •Hyperechoic
- •Large Bladder
- •Small Bladder
- •Altered Bladder Shape
- •Intracavitary Mass
- •Hypoechoic
- •Hyperechoic
- •Echogenic
- •Wall Changes
- •Diffuse Wall Thickening
- •Circumscribed Wall Thickening
- •Concavities and Convexities
- •12.1 The Prostate
- •Enlarged Prostate
- •Regular
- •Irregular
- •Small Prostate
- •Regular
- •Echogenic
- •Circumscribed Lesion
- •Anechoic
- •Hypoechoic
- •Echogenic
- •12.2 Seminal Vesicles
- •Diffuse Change
- •Hypoechoic
- •Circumscribed Change
- •Anechoic
- •Echogenic
- •Irregular
- •12.3 Testis, Epididymis
- •Diffuse Change
- •Enlargement
- •Decreased Size
- •Circumscribed Lesion
- •Anechoic or Hypoechoic
- •Irregular/Echogenic
- •Epididymal Lesion
- •Anechoic
- •Hypoechoic
- •Intrascrotal Mass
- •Anechoic or Hypoechoic
- •Echogenic
- •13 Female Genital Tract
- •Masses
- •Abnormalities of Size or Shape
- •Uterus
- •Abnormalities of Size or Shape
- •Myometrial Changes
- •Intracavitary Changes
- •Endometrial Changes
- •Fallopian Tubes
- •Hypoechoic Mass
- •Anechoic Cystic Mass
- •Solid Echogenic or Nonhomogeneous Mass
- •14 Thyroid Gland
- •Diffuse Changes
- •Enlarged Thyroid Gland
- •Small Thyroid Gland
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Circumscribed Changes
- •Anechoic
- •Hypoechoic
- •Isoechoic
- •Hyperechoic
- •Irregular
- •Differential Diagnosis of Hyperthyroidism
- •Types of Autonomy
- •15 Pleura and Chest Wall
- •Chest Wall
- •Masses
- •Parietal Pleura
- •Nodular Masses
- •Diffuse Pleural Thickening
- •Pleural Effusion
- •Anechoic Effusion
- •Echogenic Effusion
- •Complex Effusion
- •16 Lung
- •Masses
- •Anechoic Masses
- •Hypoechoic Masses
- •Complex Masses
- •Index

■ Enlargement
As already mentioned, only enlarged adrenal glands can be clearly visualized with ultrasound.
Anechoic Structure
Glands |
Enlargement |
|
|
Adrenal Cyst |
|||
|
|
|
|
|
|||
|
|
|
|
Anechoic Structure |
|
|
Intra-adrenal Hemorrhage |
|
|
|
|
|
|||
Adrenal |
|
Hypoechoic Structure |
|
|
Adrenal Abscess |
||
|
Complex Echo Structure |
|
|
||||
|
|
|
Cystic Tumor |
||||
|
|
|
|
|
|
||
|
|
|
|
Hyperechoic Structure |
|
|
|
|
|
|
|
|
|
|
|
Masses adjacent to the adrenal glands. Anechoic adrenal masses require differentiation from anechoic structures that are located near the gland but are not related to it. These include:
●Renal cysts
●Pancreatic pseudocysts
●Splenic vessels
Renal cysts. Parietal cysts located in the upper pole of the kidney are particularly apt to be mistaken for adrenal cysts. They are distinguished by defining the relation of the cyst to the renal parenchyma.
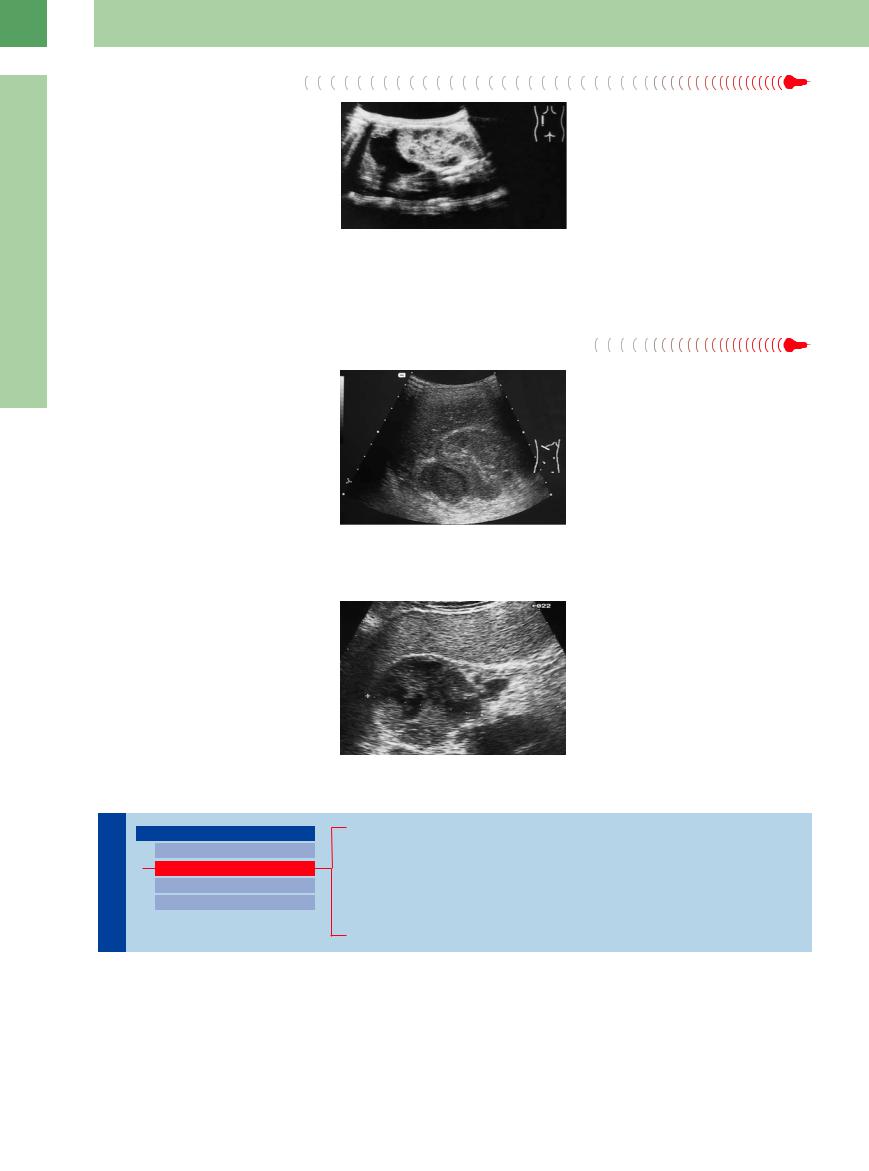
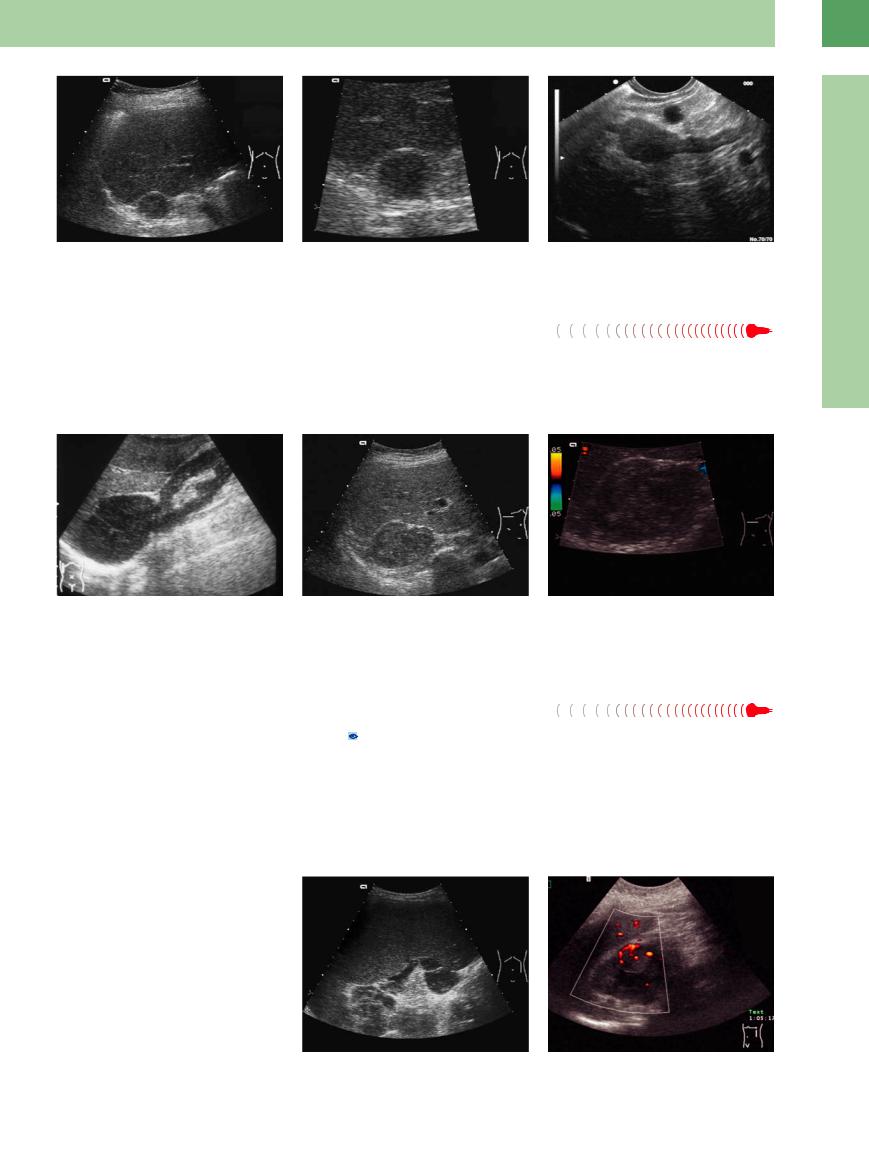
Pancreatic pseudocysts and tumors. Pancreatic pseudocysts often form in the retroperitoneum following acute pancreatitis. The contents of the cysts may be completely anechoic, and the wall is usually irregular (Fig.10.6). Fine-needle aspiration and laboratory analysis demonstrate high levels of pancreatic enzymes. Cystadenocarcinoma of the pancreas can also be a source of confusion (Fig.10.7).
Fig. 10.6 Pancreatic tail pseudocysts are clearly visualized with trans-splenic ultrasound and require differentiation from upper renal cysts and adrenal cysts. Diagnosis is aided by the history and ultrasound-guided fine-needle aspiration.
Splenic vessels. Tortuous and ectatic splenic vessels can mimic a cystic mass in the adrenal region. Shunt vessels in portal hypertension (e. g., secondary to splenic vein thrombosis) can also assume bizarre shapes.
Fig. 10.7 A cystic, septated mass medial to the left kidney is localized to the pancreatic tail, not the left adrenal gland. Imaging and ultrasound-guided fine-needle aspiration identify the lesion as a cystadenocarcinoma of the pancreas.
Adrenal Cyst





















































A cyst of the adrenal region is anechoic, has smooth margins, and shows distal acoustic enhancement. Its extent is variable. True cysts have regular walls and are filled with serous material (Fig.10.8).
Most cystic masses in the adrenal region are |
|
|
secondary cysts that develop following pan- |
|
|
creatitis, hemorrhage, or inflammation. |
|
|
The greater mobility of adrenal cysts serves |
|
|
to differentiate them from hepatic cysts in the |
|
|
right adrenal region. Lack of contact with the |
|
|
renal parenchyma distinguishes them from a |
|
|
cyst of the upper renal pole. |
Fig. 10.8 |
b Behind the right liver lobe is a typical position to detect |
|
a Round, sharply circumscribed, echo-free mass located |
an adrenal gland cyst with typical cystic criteria: echoic |
|
medial to the spleen and cranial to the left kidney: adre- |
wall, echo-free content, and dorsal sound amplification |
|
nal cyst. Ultrasound-guided fine-needle aspiration ex- |
(image courtesy of Dr. Christian Jenssen, Strausberg, |
|
cluded pancreatic cyst, hemorrhage, etc. |
Germany). |
10
Enlargement
369
10
Adrenal Glands
Fig. 10.9 Echo-free intra-adrenal hemorrhage in a newborn.
Adrenal Abscess




























An abscess of the adrenal glands is rarely an- |
Fig. 10.10 Adrenal abscess. Circumscribed hypoechoic |
echoic. It is usually hypoechoic or has a com- |
structure in the right adrenal region. Typical inflamma- |
plex echo structure. When the contents are |
tory laboratory findings. Ultrasound-guided fine-needle |
anechoic, the clinical and laboratory findings |
aspiration yielded pus. |
can differentiate the lesion from an ordinary |
|
cyst. The wall is irregular, and distal acoustic |
|
enhancement may be present (Fig.10.10). |
|
Cystic Tumor





















































A cystic tumor may be anechoic in rare cases, |
Fig. 10.11 Hypoechoic, partly cystic, predominantly solid |
but usually it is hypoechoic. The walls are ir- |
tumor in the right adrenal gland: adrenal metastasis from |
regular in thickness and outline with some |
bronchial carcinoma. |
|
|
solid elements (Fig.10.11). |
|
Hypoechoic Structure
Adrenal Glands

Enlargement
Anechoic Structure
Hypoechoic Structure
Complex Echo Structure
Hyperechoic Structure
Hyperplasia
Adenoma
Metastasis
Lymphoma
Adrenal Carcinoma
Incidentaloma
Hyperplasia 





















































Hyperplastic adrenal glands are usually hypoechoic, especially in the cortical zone. They appear plump and elongated, may show lowlevel nodular echoes, and usually are only moderately enlarged (Fig.10.12). Adrenal hy-
perplasia can occur, for example, as an adaptive response in ACTH-dependent Cushing syndrome. It may have a paraneoplastic cause, or it may occur in hyperaldosteronism. The hyperplasia is bilateral in most cases. The adrenal
glands are poorly demarcated from their surroundings. Again, CT provides a better view of the hyperplastic adrenal glands, which usually cannot be detected with ultrasound.
370
10
Enlargement
Fig. 10.12
a Hypoechoic enlargement of the adrenal glands, identified as bilateral adrenal hyperplasia.
b The hyperplastic adrenal gland is enlarged to approximately 2.5 cm. Affected glands may retain their normal triangular shape or may be rounded.
c Endosonography detects a small hyperplastic nodule of the region of the proximal crura.
Adenoma 































Adenomas are uniformly hypoechoic with |
indicate that they are quite common |
smooth margins and a round to oval shape, |
(10–20%), but most adenomas (90%) produce |
although some lesions have scalloped borders |
no endocrine symptoms and are too small to be |
(Fig.10.13). Adenomas occasionally have a non- |
seen with ultrasound. The average size of 23 |
homogeneous appearance. Autopsy statistics |
operated adenomas in one study was 1.5 cm,7 |
although they may exceed 5 cm in diameter. Adenomas are bilateral in a small percentage of patients. Functioning and nonfunctioning adenomas are indistinguishable by their sonographic features.
Fig. 10.13
a Large, very hypoechoic, sharply circumscribed mass above the right kidney. Typical adrenal adenoma. If the gland is more than 5 cm in diameter, laparoscopic adrenalectomy should be performed.
b Hypoechoic, sharply circumscribed adenoma of the right adrenal gland discovered at routine ultrasound (confirmed by ultrasound-guided fine-needle aspiration).
c Scant vascularity on color Doppler.
Metastasis































With their rich blood supply, the adrenal |
margins ( 10.1). The most common primaries |
glands are the fourth most frequent site for |
are bronchial carcinoma (15–25%) and breast |
hematogenous metastasis. Metastases to the |
carcinoma. Other possible sources are renal |
adrenal glands account for the majority of solid |
carcinoma, gastric carcinoma, pancreatic carci- |
adrenal tumors. These lesions are less homoge- |
noma, and malignant melanoma.8,9 Adrenal |
neous than adenomas and often have irregular |
metastases are bilateral in up to 30% of cases, |
and this can produce the clinical manifestations of Addison disease. Bronchial carcinoma is virtually the only tumor that is associated with isolated adrenal metastases.
Lymphoma






















































The adrenal region is a rare extranodal site of occurrence for lymphoma. Foci of lymphomatous infiltration have smooth borders and are hypoechoic (Fig.10.14). Differentiation is required from lymphomas in the renal hilum ( 9.2i). If invasion by lymphoma is suspected, other nodal stations should be scanned and commonly infiltrated organs should be closely scrutinized.
9.2i). If invasion by lymphoma is suspected, other nodal stations should be scanned and commonly infiltrated organs should be closely scrutinized.
Fig. 10.14
a Perisplenic lymphoma in the left adrenal region of a patient with B-cell lymphoma.
b Isolated highly malignant non-Hodgkin lymphoma of the left adrenal gland (rare extranodular dissemination).
371
10
Adrenal Glands
 10.1 Adrenal Metastases
10.1 Adrenal Metastases
Primary tumors that can metastasize to the adrenal glands
●Bronchial carcinoma
●Breast carcinoma
●Renal carcinoma
●Pancreatic carcinoma
●Malignant lymphoma
a Longitudinal scan of an enlarged, hypoechoic adrenal gland with metastatic bronchial carcinoma. The original shape of the gland (triangular or cowl-shaped) is largely preserved (image courtesy of Dr. B. Frentzel-Beyme, Berlin, Germany).
d Irregularly marginated tumor of the right adrenal gland located posterior to the right lobe of the liver: metastatic colon carcinoma.
b Hypoechoic enlarged adrenal gland with infiltration of the diaphragm: metastasis of a bronchial carcinoma. Transverse scan.
e Metastases are generally hypovascular in the color Doppler image, whereas adrenal adenomas may be hypervascular. Metastatic tumor of the right adrenal gland.
c Large hypoechoic, partially irregular metastasis from bronchial carcinoma on the left side (the same patient as in b; bilateral metastasis occurs in 50%).
f Hypoechoic smoothly margined adrenal metastases from bronchial carcinoma.
Adrenal Carcinoma 

















































Adrenal carcinoma is usually hypoechoic with |
Fig. 10.15 Adrenal carcinoma may be hypoechoic or may |
|
irregular margins. It frequently infiltrates its |
have a complex echo structure. Usually it is relatively |
|
large when diagnosed (in this case 8 cm × 9 cm) and has |
||
surroundings, and metastases can be demon- |
||
irregular margins. |
||
strated in the adrenal region and in other or- |
||
|
||
gans (e. g., the liver; Fig.10.15). |
|
Incidentaloma




















































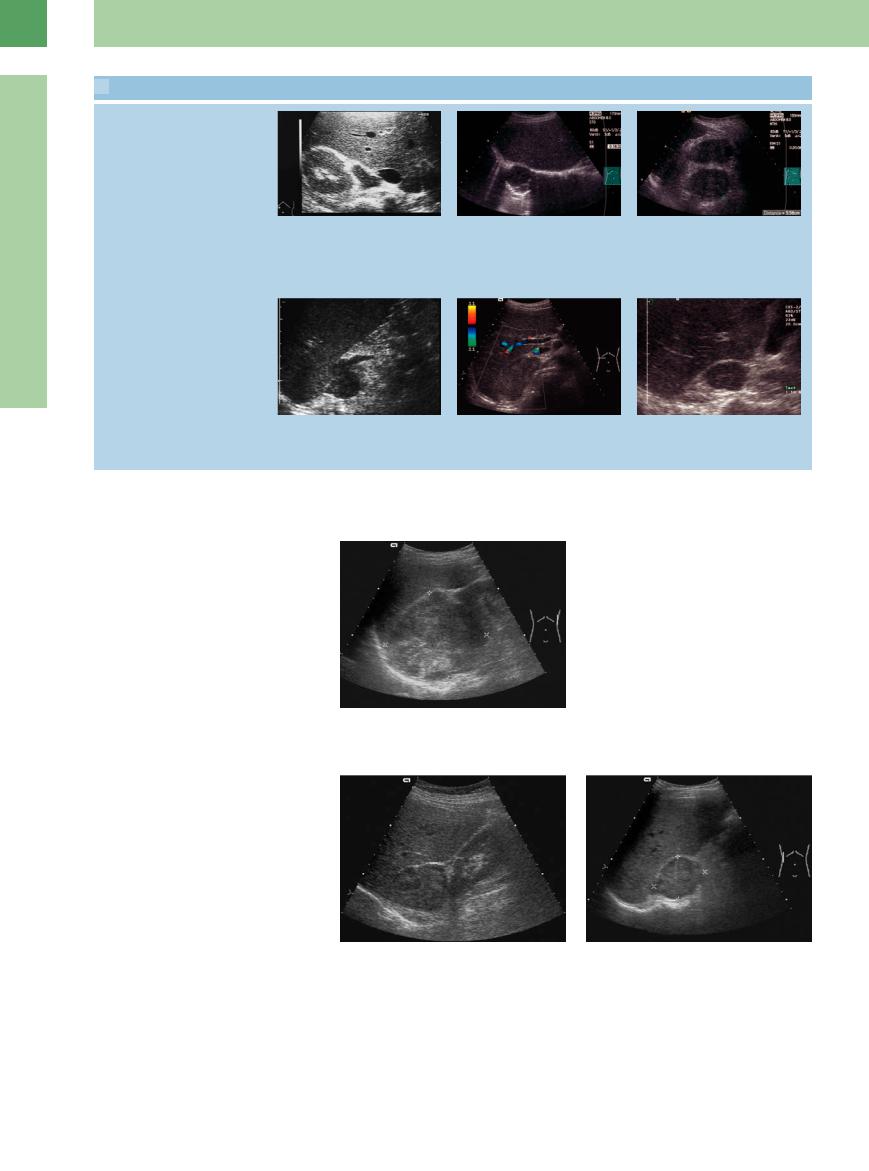
An incidentaloma is an adrenal tumor that is detected incidentally in an asymptomatic patient. Incidentalomas are found in 1% of CT examinations.10 They are much less common in ultrasound examinations, if only because of the difficulty in defining small lesions (Fig.10.16). The predominantly hypoechoic tumors listed in Table 10.2 account for the great majority of incidentalomas. Figure 10.17 shows the algorithm used in the investigation of incidentalomas. The recommended endocrine work-up is detailed in Table 10.3. In some cases, ultrasound-guided fine-needle aspiration can also aid in the evaluation of incidentalomas (Fig.10.18).
Hypoechoic tumors of the adrenal region require differentiation from other masses in that region such as a renal tumor (Fig.10.19), accessory spleen (Fig.10.20), lymphoma (Fig.10.21), and gastric folds.
Fig. 10.16 |
b Hypoechoic tumor detected incidentally in the right |
a Approximately 5 cm hypoechoic mass above the right |
adrenal region. Because of its irregular margins, biopsy |
kidney: typical incidentaloma without associated symp- |
was performed. Result: metastasis from a previously un- |
toms, detected at routine upper abdominal ultrasound. |
diagnosed bronchial carcinoma. |
Histology identified the lesion as an adrenal adenoma |
|
(most common incidentaloma). |
|
372

|
|
|
|
|
|
|
10 |
|
Table 10.2 Spectrum and incidence of incidentalomas14 |
|
|
|
|
Enlargement |
|||
Diagnosis |
Imaging and |
Imaging and |
Operation15 |
|||||
|
||||||||
|
operation13 |
operation8 |
|
Mantero 2000 |
|
|||
|
Reincke 1995 |
Allolio 2001 |
|
|
|
|||
|
n |
% |
n |
% |
n |
% |
|
|
Overall |
172 |
|
267 |
|
380 |
|
|
|
Adrenal adenoma |
134 |
77.9 |
230 |
86.1 |
198 |
52.1 |
|
|
Nonfunctioning adrenal adenoma |
119 |
69.2 |
206 |
77.2 |
137 |
36.0 |
|
|
Adrenal carcinoma |
1 |
0.6 |
1 |
0.4 |
47 |
12.4 |
|
|
Adrenal hyperplasia |
– |
|
3 |
1.1 |
– |
|
|
|
Pheochromocytoma |
5 |
2.9 |
7 |
2.6 |
42 |
11.0 |
|
|
Ganglioneuroma |
2 |
1.2 |
3 |
1.1 |
15 |
3.9 |
|
|
Myelolipoma |
6 |
3.5 |
9 |
3.4 |
30 |
7.9 |
Fig. 10.17 Algorithm for investigating an adrenal inciden- |
|
taloma.13 |
||||||||
|
|
|
|
|
|
|
||
Adrenal cyst |
5 |
2.9 |
6 |
2.2 |
20 |
5.3 |
|
|
Metastasis |
1 |
0.6 |
3 |
1.1 |
7 |
1.8 |
|
|
Others |
2 |
1.2 |
5 |
1.9 |
21 |
5.5 |
|
|
Table 10.3 Endocrine laboratory work-up of adrenal incidentaloma13
Initial work-up
Mandatory |
● Free catecholamines in 24h urine |
|
● Serum cortisol in dexamethasone suppression test (1 mg) |
Optional |
● Plasma renin activity after 30 min rest period |
|
● Potassium excretion in 24h urine |
Extended work-up if initial findings are abnormal |
|
Preclinical Cushing syndrome |
● High-dose dexamethasone suppression test (8 mg) |
|
● CRH stimulation test |
Conn syndrome |
● Aldosterone-18-glucuronide in 24h urine |
●Plasma renin activity and aldosterone at rest and orthostasis
●Selective renal vein catheterization with bilateral blood sampling for aldosterone and cortisol in adrenal venous blood
Fig. 10.18 Algorithm for “sonographic” adrenal tumors and the use of ultrasound-guided fine-needle aspiration.12
Ultrasound-guided Fine-needle Aspiration of an Adrenal Lesion
Given the frequency of incidentally de- |
requiring treatment. The sensitivity of adre- |
tected adrenal tumors, every case should |
nal usFNA is between 90% and 95%, and it |
undergo an initial endocrine work-up. If the |
can furnish material for cytological or pref- |
tumor cannot be positively identified by |
erably histological analysis with a relatively |
laboratory tests and imaging (ultrasound, |
low risk of complications. The procedure is |
CT), ultrasound-guided fine-needle aspira- |
performed in a lateral position. Access is |
tion (usFNA) can supply a diagnosis in cases |
more favorable for a right-sided lesion |
than a left-sided lesion, and the complication rate is also somewhat higher on the left side. usFNA is particularly indicated for the
oncological investigation of tumors larger than 3 cm (Fig. 10.18).9,11
373