

- •Contents
- •Preface
- •Contributors
- •1 Vessels
- •1.1 Aorta, Vena Cava, and Peripheral Vessels
- •Aorta, Arteries
- •Anomalies and Variant Positions
- •Dilatation
- •Stenosis
- •Wall Thickening
- •Intraluminal Mass
- •Perivascular Mass
- •Vena Cava, Veins
- •Anomalies
- •Dilatation
- •Intraluminal Mass
- •Compression, Infiltration
- •1.2 Portal Vein and Its Tributaries
- •Enlarged Lumen Diameter
- •Portal Hypertension
- •Intraluminal Mass
- •Thrombosis
- •Tumor
- •2 Liver
- •Enlarged Liver
- •Small Liver
- •Homogeneous Hypoechoic Texture
- •Homogeneous Hyperechoic Texture
- •Regionally Inhomogeneous Texture
- •Diffuse Inhomogeneous Texture
- •Anechoic Masses
- •Hypoechoic Masses
- •Isoechoic Masses
- •Hyperechoic Masses
- •Echogenic Masses
- •Irregular Masses
- •Differential Diagnosis of Focal Lesions
- •Diagnostic Methods
- •Suspected Diagnosis
- •3 Biliary Tree and Gallbladder
- •3.1 Biliary Tree
- •Thickening of the Bile Duct Wall
- •Localized and Diffuse
- •Bile Duct Rarefaction
- •Localized and Diffuse
- •Bile Duct Dilatation and Intraductal Pressure
- •Intrahepatic
- •Hilar and Prepancreatic
- •Intrapancreatic
- •Papillary
- •Abnormal Intraluminal Bile Duct Findings
- •Foreign Body
- •The Seven Most Important Questions
- •3.2 Gallbladder
- •Changes in Size
- •Large Gallbladder
- •Small/Missing Gallbladder
- •Wall Changes
- •General Hypoechogenicity
- •General Hyperechogenicity
- •General Tumor
- •Focal Tumor
- •Intraluminal Changes
- •Hyperechoic
- •Hypoechoic
- •Nonvisualized Gallbladder
- •Missing Gallbladder
- •Obscured Gallbladder
- •4 Pancreas
- •Diffuse Pancreatic Change
- •Large Pancreas
- •Small Pancreas
- •Hypoechoic Texture
- •Hyperechoic Texture
- •Focal Changes
- •Anechoic Lesion
- •Hypoechoic Lesion
- •Isoechoic Lesion
- •Hyperechoic Lesion
- •Irregular (Complex Structured) Lesion
- •Dilatation of the Pancreatic Duct
- •Marginal/Mild Dilatation
- •Marked Dilatation
- •5 Spleen
- •Nonfocal Changes of the Spleen
- •Diffuse Parenchymal Changes
- •Large Spleen
- •Small Spleen
- •Focal Changes of the Spleen
- •Anechoic Mass
- •Hypoechoic Mass
- •Hyperechoic Mass
- •Splenic Calcification
- •6 Lymph Nodes
- •Peripheral Lymph Nodes
- •Head/Neck
- •Extremities (Axilla, Groin)
- •Abdominal Lymph Nodes
- •Porta Hepatis
- •Splenic Hilum
- •Mesentery (Celiac, Upper and Lower Mesenteric Station)
- •Stomach
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •Small/Large Intestine
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •8 Peritoneal Cavity
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Wall Structures
- •Smooth Margin
- •Irregular Margin
- •Intragastric Processes
- •Intraintestinal Processes
- •9 Kidneys
- •Anomalies, Malformations
- •Aplasia, Hypoplasia
- •Cystic Malformation
- •Anomalies of Number, Position, or Rotation
- •Fusion Anomaly
- •Anomalies of the Renal Calices
- •Vascular Anomaly
- •Diffuse Changes
- •Large Kidneys
- •Small Kidneys
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Irregular Structure
- •Circumscribed Changes
- •Anechoic Structure
- •Hypoechoic or Isoechoic Structure
- •Complex Structure
- •Hyperechoic Structure
- •10 Adrenal Glands
- •Enlargement
- •Anechoic Structure
- •Hypoechoic Structure
- •Complex Echo Structure
- •Hyperechoic Structure
- •11 Urinary Tract
- •Malformations
- •Duplication Anomalies
- •Dilatations and Stenoses
- •Dilated Renal Pelvis and Ureter
- •Anechoic
- •Hypoechoic
- •Hypoechoic
- •Hyperechoic
- •Large Bladder
- •Small Bladder
- •Altered Bladder Shape
- •Intracavitary Mass
- •Hypoechoic
- •Hyperechoic
- •Echogenic
- •Wall Changes
- •Diffuse Wall Thickening
- •Circumscribed Wall Thickening
- •Concavities and Convexities
- •12.1 The Prostate
- •Enlarged Prostate
- •Regular
- •Irregular
- •Small Prostate
- •Regular
- •Echogenic
- •Circumscribed Lesion
- •Anechoic
- •Hypoechoic
- •Echogenic
- •12.2 Seminal Vesicles
- •Diffuse Change
- •Hypoechoic
- •Circumscribed Change
- •Anechoic
- •Echogenic
- •Irregular
- •12.3 Testis, Epididymis
- •Diffuse Change
- •Enlargement
- •Decreased Size
- •Circumscribed Lesion
- •Anechoic or Hypoechoic
- •Irregular/Echogenic
- •Epididymal Lesion
- •Anechoic
- •Hypoechoic
- •Intrascrotal Mass
- •Anechoic or Hypoechoic
- •Echogenic
- •13 Female Genital Tract
- •Masses
- •Abnormalities of Size or Shape
- •Uterus
- •Abnormalities of Size or Shape
- •Myometrial Changes
- •Intracavitary Changes
- •Endometrial Changes
- •Fallopian Tubes
- •Hypoechoic Mass
- •Anechoic Cystic Mass
- •Solid Echogenic or Nonhomogeneous Mass
- •14 Thyroid Gland
- •Diffuse Changes
- •Enlarged Thyroid Gland
- •Small Thyroid Gland
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Circumscribed Changes
- •Anechoic
- •Hypoechoic
- •Isoechoic
- •Hyperechoic
- •Irregular
- •Differential Diagnosis of Hyperthyroidism
- •Types of Autonomy
- •15 Pleura and Chest Wall
- •Chest Wall
- •Masses
- •Parietal Pleura
- •Nodular Masses
- •Diffuse Pleural Thickening
- •Pleural Effusion
- •Anechoic Effusion
- •Echogenic Effusion
- •Complex Effusion
- •16 Lung
- •Masses
- •Anechoic Masses
- •Hypoechoic Masses
- •Complex Masses
- •Index
9
Diffuse Changes
■ Diffuse Changes
Large Kidneys
Kidneys |
Anomalies, Malformations |
|||
|
|
|
||
|
|
|
Diffuse Changes |
|
|
|
|
||
|
|
|
|
Large Kidneys |
|
|
|
|
|
|
|
|
|
Small Kidneys |
|
|
|
|
Hypoechoic Structure |
|
|
|
|
Hyperechoic Structure |
|
|
|
|
Irregular Structure |
|
|
|
Circumscribed Changes |
|
|
|
|
||
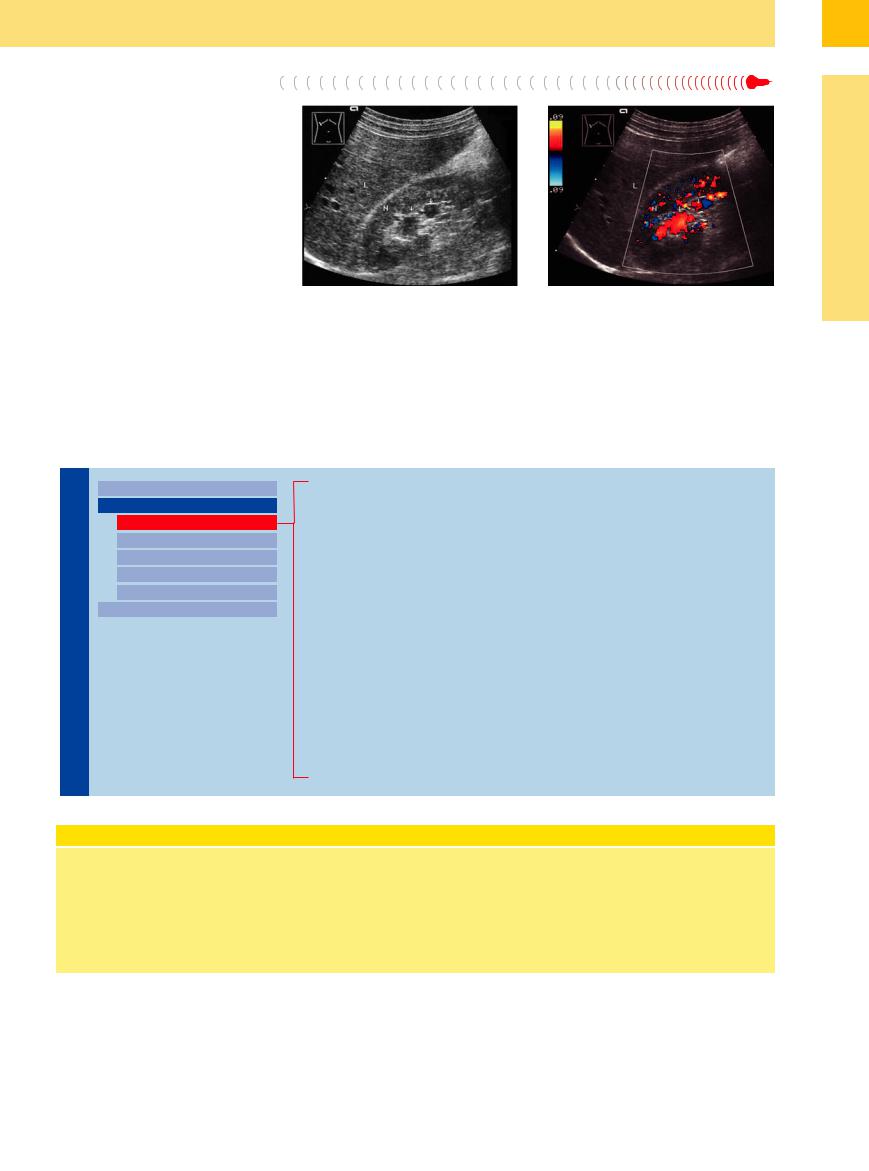
Fig. 9.18 Intrarenal vascular ectasia. Arteriovenous mal- |
b Color duplex sonography (CDS) identifies the cystic |
formation appears as an echo-free mass within the kid- |
masses as ectatic intrarenal arterial vessels, probably |
ney. L = liver; N = kidney. |
arteriovenous malformations of the renal artery. (Doppler |
a B-mode image demonstrates cystic masses in the renal |
spectral analysis with resistance index determination |
sinus echo (arrows). |
yields additional information on the nature of the vascu- |
|
lar ectasia.) |
Constitutional/Acromegaly
Duplex Kidney, Single Kidney
Diabetic Nephropathy
Polycystic Kidney Disease
Acute Renal Failure, Shock Kidney
Septic–Toxic Kidneys
Acute Urinary Retention, Acute Outflow Obstruction
Renal Congestion Due to Heart Failure
Renal Vein Thrombosis
Acute Glomerulonephritis
Acute Pyelonephritis
AIDSand Heroin-induced Nephropathy
Amyloidosis/Paraprotein Kidney
Pyonephrosis
Renal Tumor
Renal Allograft, Allograft Rejection
Sonographic Determination of Renal Size
The sonographic estimation of renal size is unreliable. Whether a kidney appears large or small in ultrasonography depends very much on the selected field of view, i. e., an undersize kidney may appear large because it is displayed at a large scale, and vice versa (Fig. 9.19). For some examinations, then, it is necessary to measure at least the longi-
tudinal renal diameter and parenchymal thickness.
Anatomically, the adult kidney measures 1 cm over the sonographic diameter, 10–11.5 cm in length, 5–7 cm in width, and 3–4 cm in thickness. For physical reasons, radiographic measurements of the kidney add approximately 1.5 cm to its
The individual scatter of measurement is about |
diameters divided by 2. Volume correlates |
0.3–0.5 cm. The parenchymal thickness is in the |
with age, or, even better, with body length. |
range 13–18 mm; small kidneys have less than |
Normal volumes range from 90 to 170 mL; |
12 mm. For specific examinations, volume |
small kidneys less than 80 mL, overlarge kid- |
analysis is preferable: the product of the largest |
neys more than 180 mL (Fig. 9.19). |
longitudinal, transverse, and anteroposterior |
|
length and 1 cm to its width. Sonographic measurements, by contrast, are slightly smaller than the true dimensions because the kidneys occupy planes that are angled laterally and anteromedially and do not coincide precisely with the planes used for routine scanning.
329
9
Kidneys
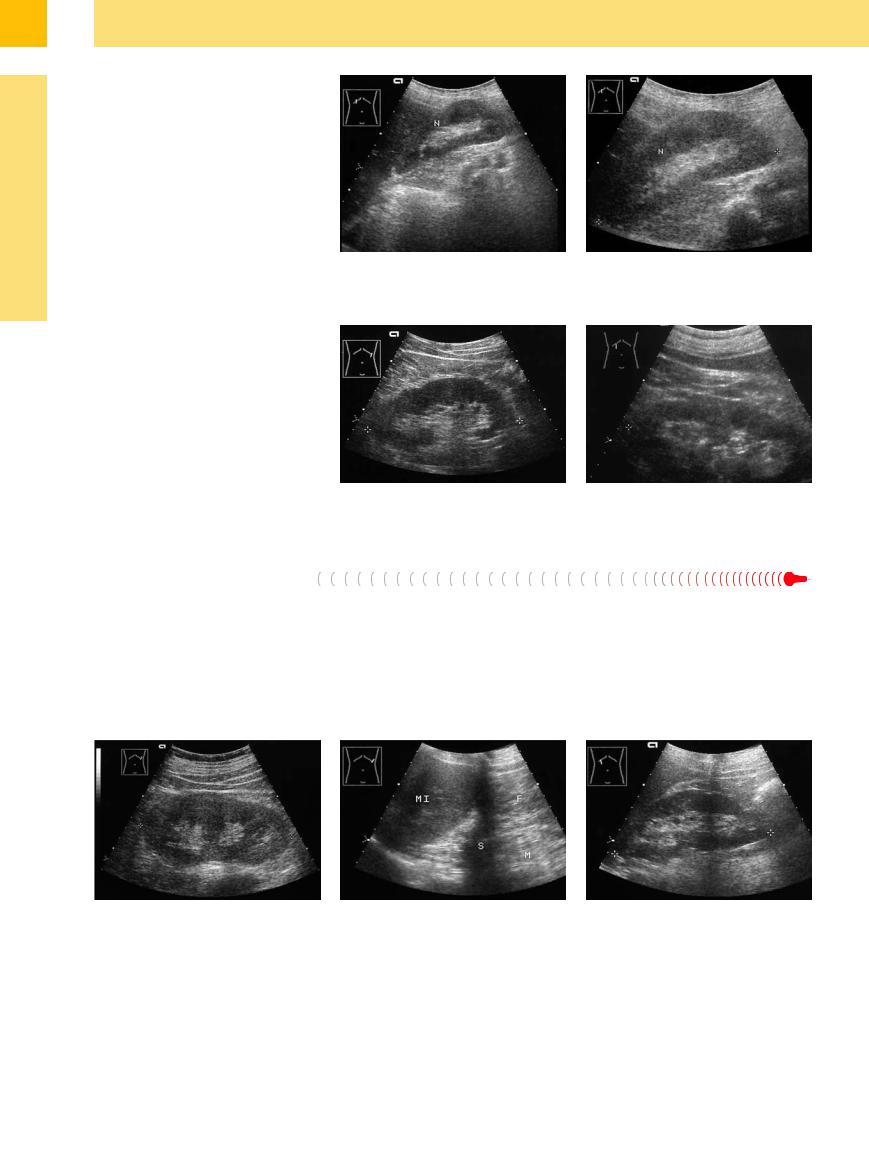
Fig. 9.19 Subjective assessment of renal size.
a In a large field of view, the kidney (N) appears small in relation to the overall image.
b The kidney (N) appears larger in an enlarged view. According to measurements, this kidney is small but still within normal limits for the patient’s body size.
Constitutional/Acromegaly













































Renal size is dependent on the patient’s constitution or body size. As a result, the renal dimensions may be greater or less than normal. Lengths from 9.6 to 13 cm may still be considered normal, depending on body size (Fig. 9.20). Nomograms plotted for children show a direct correlation with body size.
Fig. 9.20 |
b Enlarged kidneys in acromegaly (13.7 cm). |
a Constitutionally large kidney (13.5 cm, |
contralateral |
13.0 cm) in a 47-year-old man with a height of 196 cm and body weight of 111 kg.
Duplex Kidney, Single Kidney
Kidney
Duplex kidney. One of the most common types of renal enlargement involves duplex kidneys, whose sonographic features are described above. Their shape in ultrasound resembles that of a pretzel. The longitudinal diameter may be normal or increased up to 15 cm, with a normal width. The overall thickness may be increased if the duplicated kidneys are ar-
ranged side by side (Fig. 9.21), creating a tu- mor-like appearance. The moieties can be distinguished from a tumor by color Doppler sonography, which shows a normal duplex vascular pattern.
Single kidney. A single kidney undergoes compensatory physiological enlargement in re-
sponse to contralateral hypoplasia or aplasia, contralateral nephrectomy, a nonfunctioning opposite kidney, or a renal allograft (Fig. 9.22).
Fig. 9.21 Large duplex kidney with multiple parenchymal |
Fig. 9.22 Renal aplasia. |
b Compensatory enlargement of the right kidney |
bands. |
a Absent left kidney, empty renal fossa below the spleen |
(12.3 cm, cursors). |
|
(MI) on the left side. F = fatty tissue; M = musculature; S = |
|
|
shadow. |
|
330
9
Diffuse Changes
is why early detection at the hyperperfusion stage critically influences the prognosis. Other criteria of diabetic nephropathy are not present in stages I and II, and the only sign of hyperperfusion is an elevated creatinine clearance rate in excess of 120 mL/min.
Sonographic features. In ultrasound, the renal parenchyma is thickened and often shows increased sonodensity. The medullary pyramids appear bulky and less echogenic than the adja-
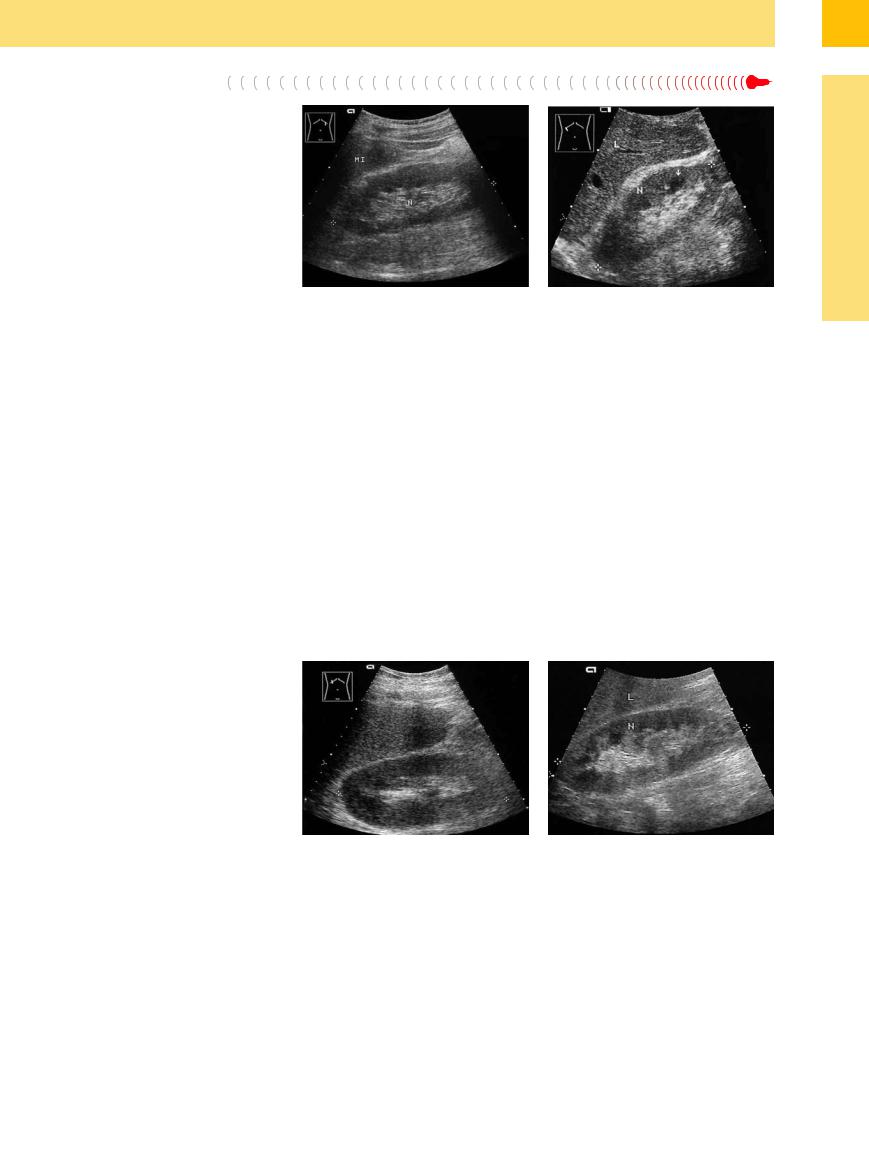
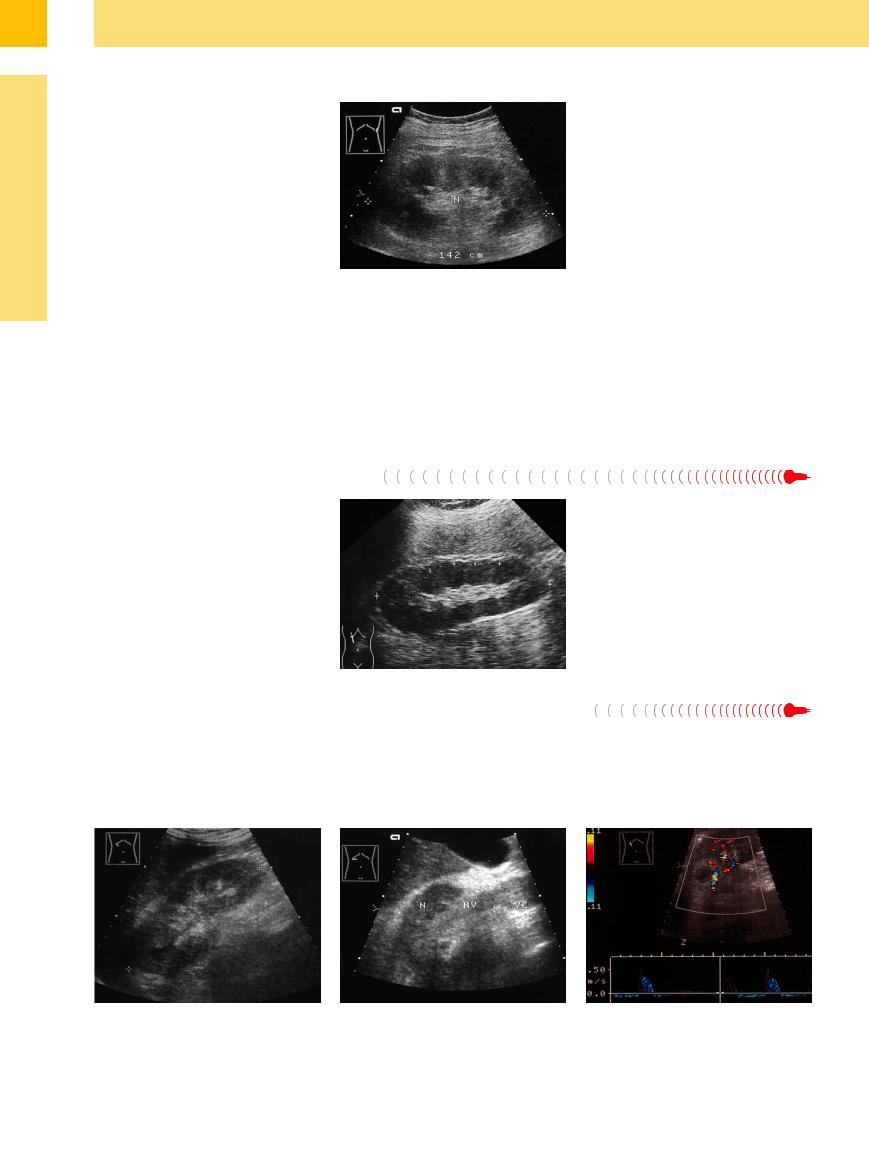
Fig. 9.23 Stage IV diabetic nephropathy with a large kidney (N, 12.1 cm) and proteinuria. Long history of type II diabetes mellitus. Six months later, persistent diarrhea and reversible decompensation with creatinine of 8 mg/ dL. MI = spleen.
cent parenchyma, which often but not always shows increased echogenicity. The kidney should therefore be measured in patients evaluated for diabetic nephropathy. It is not until an advanced stage, when the patient requires hemodialysis, that the kidney shrinks in size and
Fig. 9.24 Diabetic nephropathy. Large kidney (N, 12.5 cm) with prominent hypoechoic medullary pyramids (arrow). L = liver.
shows obvious structural changes. Other signs of diabetic nephropathy are swollen, hypoechoic medullary pyramids. In advanced stages (Mogensen stages IV–V, here with manifest renal failure), the parenchyma shows increased echogenicity (Fig. 9.23, Fig. 9.24).
Polycystic Kidney Disease














































Besides multiple anechoic lesions and ill-de- fined borders, polycystic kidneys are conspicuous by their enormous enlargement due to the mass effect of the cysts (Fig. 9.8).
Acute Renal Failure, Shock Kidney
Shock Kidney 









































In the setting of acute renal failure and renal shock or severe hypovolemia, ultrasound usually shows an increased parenchymal volume and a decrease (or increase) in echogenicity with enlargement of the kidneys and consequent narrowing of the sinus echo complex (Fig. 9.25).
Fig. 9.25
a Acute prerenal renal failure. Creatinine 8.2 mg/dL (al- cohol-related disease, persistent vomiting and diarrhea). The kidney is greatly enlarged (16.1 cm) with a hypoechoic, ill-defined structure.
b Sepsis, alcohol-related disease, kidney (N) enlarged to 13.0 cm. Renal echogenicity is slightly decreased. The medullary pyramids are swollen and very hypoechoic.
L = liver.
331
9
Kidneys
Septic–Toxic  Kidneys
Kidneys 
















































Renal enlargement also occurs occasionally in |
Fig. 9.26 Septic–toxic kidneys with renal failure: greatly |
|
sepsis. The kidneys tend to show increased |
enlarged kidney (N) with parenchymal swelling. The me- |
|
dullary pyramids are markedly enlarged and hypoechoic. |
||
echogenicity, probably due to a suppurative |
||
|
||
leukocytic reaction to septicopyemic foci in |
|
|
the organs. The reaction may also be a result |
|
|
of dehydration (Fig. 9.26). |
|
Acute Urinary Retention,  Acute Outflow Obstruction
Acute Outflow Obstruction































In this situation as well, the kidneys often react with enlargement and decreased echogenicity due to interstitial edema. The medullary pyramids may show signs of conspicuous swelling. Often the bladder is greatly distended. The sonographic renal changes are the same as those seen in renal congestion resulting from heart failure.
Renal Congestion Due to Heart Failure
The fluid build-up that occurs in severe congestive heart failure leads to swelling and increased echogenicity of the renal parenchyma secondary to edema and hemorrhage. This swelling is another cause of renal enlargement (Fig. 9.27).
Renal Vein Thrombosis
Thrombosis 
























Acute renal vein thrombosis also leads to en- |
● |
A broadened renal vein that contains intra- |
largement and unilateral hypoechoic swelling |
|
luminal echoes and is devoid of color flow |
of the parenchyma (Fig. 9.28). The diagnosis is |
● |
A high resistance index (RI, after Pourcelot: |
supported by: |
|
(Vmax − Vmin)/Vmax in the intrarenal renal ar- |
|
|
teries |
Fig. 9.27 Acute prerenal renal failure: enlarged kidneys (13.0 cm), hypoechoic parenchyma, and swollen, hypoechoic medullary pyramids (arrows).
●Reverse flow (hard, negative systolic signal in the renal artery)
Fig. 9.28 |
b Respective renal vein and caval thrombosis. |
c Spectral analysis in renal vein thrombosis indicates an |
a Renal vein thrombosis secondary to suppurative pyeli- |
|
extremely high resistance index of 0.96. |
tis. The kidney is greatly enlarged to 14.2 cm (cursors) |
|
|
with a hazy, irregular hypoechoic structure. |
|
|
332
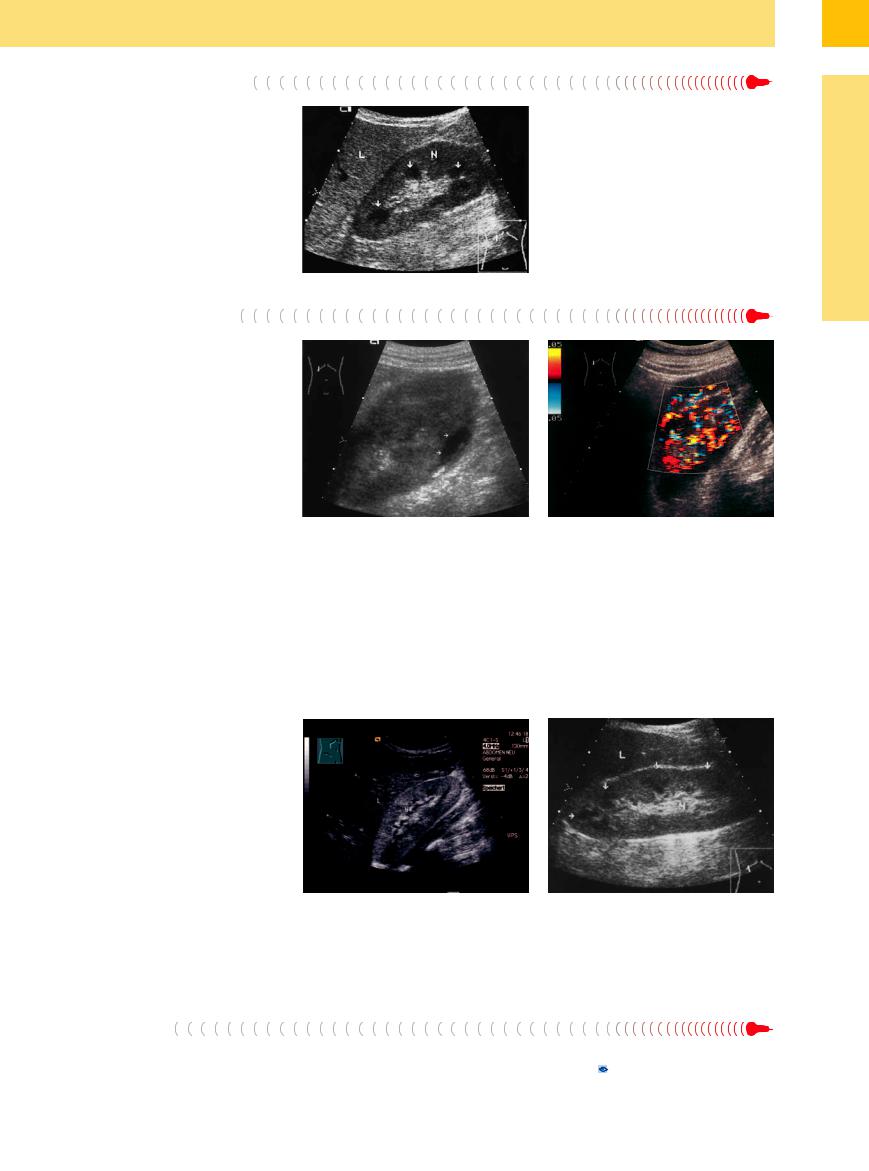
Fig. 9.29 Acute IgA nephritis: slightly enlarged, swollen kidney (N) with prominent medullary pyramids (arrows).
A different picture is seen with severe acute |
|
|
septic pyelonephritis, in which one or both |
|
|
kidneys are enlarged and generally show a de- |
|
|
crease in parenchymal echogenicity. Often |
|
|
there are accompanying abscesses, pyonephro- |
|
|
sis, or merely circumscribed anechoic to hyper- |
|
|
echoic lesions in the parenchyma, renal pelvis, |
|
|
or renal sinus representing abscesses or in- |
|
|
fected, purulent urine. Swelling of the renal |
|
|
pelvic walls is also occasionally |
seen |
|
(Fig. 9.30). Other characteristic findings are ur- |
|
|
othelial thickening to more than 2 mm and |
|
|
hypoechoic foci in the parenchyma |
(see |
|
Fig.11.1, p. 381). |
Fig. 9.30 |
b CDS shows inflammatory hypervascularity. |
|
a Acute septic pyelonephritis: slightly enlarged kidney |
|
with swollen, hypoechoic parenchyma. The sinus echo has largely disappeared. Focal abscess (arrows).
AIDSand Heroin-induced Nephropathy
Nephropathy 






































As in other forms of renal enlargement, these |
heightens the contrast with the unchanged, |
cases show increased cortical echogenicity that |
hypoechoic medullary pyramids. |
Amyloidosis/Paraprotein Kidney 










































The sonographic changes in amyloidosis are like those seen in AIDS-related and heroin-re- lated nephropathy and acute glomerulonephritis. These conditions are not distinguishable by their sonographic features (Fig. 9.31,
Fig. 9.50).
|
Fig. 9.31 |
b Paraprotein kidney (lymphoplasmacytic immunocy- |
|
a Amyloidosis of the kidney (AA—amyloid with general- |
toma with Bence Jones proteinuria). Enlarged kidney (N) |
|
ized amyloid deposits in Mediterranean fever). Intensive |
shows slightly increased echogenicity relative to the liver |
|
hyperechoic kidney (N). L = liver. |
(L). The medullary pyramids (arrows) are markedly swol- |
|
|
len and show patchy low echogenicity due to protein- |
|
|
filled tubules, with the formation of hyaline casts in the |
|
|
distal tubules (creatinine 3.0 mg/dL). |
Pyonephrosis |
|
|
If the purulent collection in the renal pelvis |
largement. The affected kidney has a tumor- |
ically indistinguishable from a large tumor |
takes up the entire central echo complex, the |
like appearance and is in fact sonomorpholog- |
(Fig. 9.76; 11.3 g–i, p. 394). |
pyonephrotic mass leads to overall renal en- |
|
|
9
Diffuse Changes
333