

- •Contents
- •Preface
- •Contributors
- •1 Vessels
- •1.1 Aorta, Vena Cava, and Peripheral Vessels
- •Aorta, Arteries
- •Anomalies and Variant Positions
- •Dilatation
- •Stenosis
- •Wall Thickening
- •Intraluminal Mass
- •Perivascular Mass
- •Vena Cava, Veins
- •Anomalies
- •Dilatation
- •Intraluminal Mass
- •Compression, Infiltration
- •1.2 Portal Vein and Its Tributaries
- •Enlarged Lumen Diameter
- •Portal Hypertension
- •Intraluminal Mass
- •Thrombosis
- •Tumor
- •2 Liver
- •Enlarged Liver
- •Small Liver
- •Homogeneous Hypoechoic Texture
- •Homogeneous Hyperechoic Texture
- •Regionally Inhomogeneous Texture
- •Diffuse Inhomogeneous Texture
- •Anechoic Masses
- •Hypoechoic Masses
- •Isoechoic Masses
- •Hyperechoic Masses
- •Echogenic Masses
- •Irregular Masses
- •Differential Diagnosis of Focal Lesions
- •Diagnostic Methods
- •Suspected Diagnosis
- •3 Biliary Tree and Gallbladder
- •3.1 Biliary Tree
- •Thickening of the Bile Duct Wall
- •Localized and Diffuse
- •Bile Duct Rarefaction
- •Localized and Diffuse
- •Bile Duct Dilatation and Intraductal Pressure
- •Intrahepatic
- •Hilar and Prepancreatic
- •Intrapancreatic
- •Papillary
- •Abnormal Intraluminal Bile Duct Findings
- •Foreign Body
- •The Seven Most Important Questions
- •3.2 Gallbladder
- •Changes in Size
- •Large Gallbladder
- •Small/Missing Gallbladder
- •Wall Changes
- •General Hypoechogenicity
- •General Hyperechogenicity
- •General Tumor
- •Focal Tumor
- •Intraluminal Changes
- •Hyperechoic
- •Hypoechoic
- •Nonvisualized Gallbladder
- •Missing Gallbladder
- •Obscured Gallbladder
- •4 Pancreas
- •Diffuse Pancreatic Change
- •Large Pancreas
- •Small Pancreas
- •Hypoechoic Texture
- •Hyperechoic Texture
- •Focal Changes
- •Anechoic Lesion
- •Hypoechoic Lesion
- •Isoechoic Lesion
- •Hyperechoic Lesion
- •Irregular (Complex Structured) Lesion
- •Dilatation of the Pancreatic Duct
- •Marginal/Mild Dilatation
- •Marked Dilatation
- •5 Spleen
- •Nonfocal Changes of the Spleen
- •Diffuse Parenchymal Changes
- •Large Spleen
- •Small Spleen
- •Focal Changes of the Spleen
- •Anechoic Mass
- •Hypoechoic Mass
- •Hyperechoic Mass
- •Splenic Calcification
- •6 Lymph Nodes
- •Peripheral Lymph Nodes
- •Head/Neck
- •Extremities (Axilla, Groin)
- •Abdominal Lymph Nodes
- •Porta Hepatis
- •Splenic Hilum
- •Mesentery (Celiac, Upper and Lower Mesenteric Station)
- •Stomach
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •Small/Large Intestine
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •8 Peritoneal Cavity
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Wall Structures
- •Smooth Margin
- •Irregular Margin
- •Intragastric Processes
- •Intraintestinal Processes
- •9 Kidneys
- •Anomalies, Malformations
- •Aplasia, Hypoplasia
- •Cystic Malformation
- •Anomalies of Number, Position, or Rotation
- •Fusion Anomaly
- •Anomalies of the Renal Calices
- •Vascular Anomaly
- •Diffuse Changes
- •Large Kidneys
- •Small Kidneys
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Irregular Structure
- •Circumscribed Changes
- •Anechoic Structure
- •Hypoechoic or Isoechoic Structure
- •Complex Structure
- •Hyperechoic Structure
- •10 Adrenal Glands
- •Enlargement
- •Anechoic Structure
- •Hypoechoic Structure
- •Complex Echo Structure
- •Hyperechoic Structure
- •11 Urinary Tract
- •Malformations
- •Duplication Anomalies
- •Dilatations and Stenoses
- •Dilated Renal Pelvis and Ureter
- •Anechoic
- •Hypoechoic
- •Hypoechoic
- •Hyperechoic
- •Large Bladder
- •Small Bladder
- •Altered Bladder Shape
- •Intracavitary Mass
- •Hypoechoic
- •Hyperechoic
- •Echogenic
- •Wall Changes
- •Diffuse Wall Thickening
- •Circumscribed Wall Thickening
- •Concavities and Convexities
- •12.1 The Prostate
- •Enlarged Prostate
- •Regular
- •Irregular
- •Small Prostate
- •Regular
- •Echogenic
- •Circumscribed Lesion
- •Anechoic
- •Hypoechoic
- •Echogenic
- •12.2 Seminal Vesicles
- •Diffuse Change
- •Hypoechoic
- •Circumscribed Change
- •Anechoic
- •Echogenic
- •Irregular
- •12.3 Testis, Epididymis
- •Diffuse Change
- •Enlargement
- •Decreased Size
- •Circumscribed Lesion
- •Anechoic or Hypoechoic
- •Irregular/Echogenic
- •Epididymal Lesion
- •Anechoic
- •Hypoechoic
- •Intrascrotal Mass
- •Anechoic or Hypoechoic
- •Echogenic
- •13 Female Genital Tract
- •Masses
- •Abnormalities of Size or Shape
- •Uterus
- •Abnormalities of Size or Shape
- •Myometrial Changes
- •Intracavitary Changes
- •Endometrial Changes
- •Fallopian Tubes
- •Hypoechoic Mass
- •Anechoic Cystic Mass
- •Solid Echogenic or Nonhomogeneous Mass
- •14 Thyroid Gland
- •Diffuse Changes
- •Enlarged Thyroid Gland
- •Small Thyroid Gland
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Circumscribed Changes
- •Anechoic
- •Hypoechoic
- •Isoechoic
- •Hyperechoic
- •Irregular
- •Differential Diagnosis of Hyperthyroidism
- •Types of Autonomy
- •15 Pleura and Chest Wall
- •Chest Wall
- •Masses
- •Parietal Pleura
- •Nodular Masses
- •Diffuse Pleural Thickening
- •Pleural Effusion
- •Anechoic Effusion
- •Echogenic Effusion
- •Complex Effusion
- •16 Lung
- •Masses
- •Anechoic Masses
- •Hypoechoic Masses
- •Complex Masses
- •Index

9
Kidneys
Renal Tumor





















































The characteristic appearance of a malignant renal tumor is that of a circumscribed hypoechoic mass. Renal cell carcinoma (RCC) appears as a sharply circumscribed bulge in the renal outline, while urothelial carcinoma forms a hypoechoic mass in the central sinus echo. With extensive tumor infiltration, the kidney appears substantially enlarged and broadened. Its structure is markedly nonhomogeneous owing to intrarenal pyelectasis and the presence of calcifications (Fig. 9.32).
Fig. 9.32 Greatly enlarged kidney completely permeated by tumor. The kidney shows a heterogeneous, predominantly hypoechoic structure. Histological diagnosis: highgrade non-Hodgkin lymphoma.
Renal Allograft, Allograft Rejection
Rejection 








































As a solitary functioning kidney, the renal allograft is enlarged owing to adaptive hypertrophy. Additional enlargement occurs in association with allograft rejection. Enlargement is not a dependable sign of rejection, however. A more definitive sign is occlusive vasculopathy, which can be demonstrated with Doppler ultrasound.
Complications consist of renal artery stenosis, renal vein thrombosis, and arteriovenous fistulas. The RI in these cases is greater than 0.9 and the pulsatility index (PI) is greater than 1.6. Published values of sensitivity and specificity range from 14% to 98% (Fig. 9.33).
Fig. 9.33 Renal transplant. The allograft is enlarged to 13.0 cm, with accentuated renal columns (C) and prominent hypoechoic medullary pyramids (arrows).
Small Kidneys
Kidneys |
Anomalies, Malformations |
|||
|
|
|
||
|
|
|
Diffuse Changes |
|
|
|
|
||
|
|
|
|
Large Kidneys |
|
|
|
|
Small Kidneys |
|
|
|
|
|
|
|
|
|
Hypoechoic Structure |
|
|
|
|
Hyperechoic Structure |
|
|
|
|
Irregular Structure |
|
|
|
Circumscribed Changes |
|
|
|
|
||
Hypoplasia
Renal Artery Stenosis, Embolism
Arteriosclerosis, Arteriolosclerosis (Ischemic Nephropathy)
Chronic Pyelonephritis
Analgesic Nephropathy
Chronic Glomerulonephritis
Diabetic Nephropathy
Hypoplasia






















































Renal hypoplasia is characterized by a small |
enlargement and often showing ectopia or |
forms of small kidney with associated struc- |
kidney with essentially normal parenchyma |
malrotation. These features serve to distinguish |
tural and contour changes (see Fig. 9.7). |
accompanied by compensatory contralateral |
a hypoplastic kidney from other, secondary |
|
Renal Artery Stenosis, Embolism
Stenosis, Embolism










































When a small kidney is due to renal artery |
vascular hypertension is diagnosed, these ves- |
pear normal or thinned in ultrasound. The |
stenosis, generally the stenosis is severe and |
sels should be included in diagnostic consider- |
structure is largely normal. The maximum |
of long duration and is associated with chronic |
ations. |
flow velocity rises to values in excess of |
hypertension. Renal artery stenosis may be |
|
180 cm/s at the stenosis, and there is concom- |
classified as atherosclerotic (85% of cases) or |
Sonographic features. The length of the kidney |
itant spectral broadening and aliasing. The RI |
fibromuscular (15%). Accessory renal arteries |
may be reduced to less than 9 cm in higher- |
associated with stenosis or occlusion of the |
occur in up to 28% of cases, so that when reno- |
grade stenosis, and the parenchyma may ap- |
segmental arteries is less than 0.5 with a sen- |
334
9
Diffuse Changes
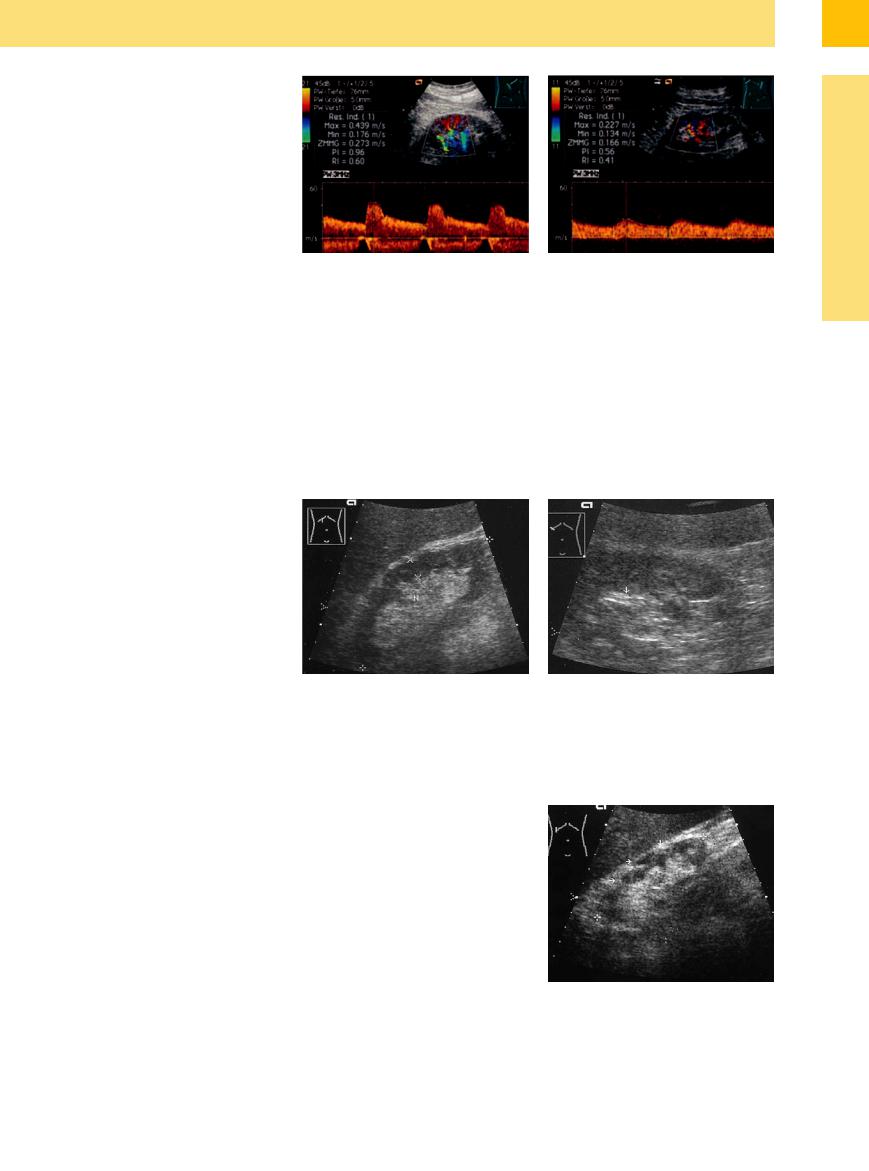
An occlusion is present when:
●Color coding and flow signals are absent
●There is markedly decreased flow velocity and RI of intrarenal branches, and
●Renal length is decreased to less than 9 cm
Fig. 9.34 Doppler spectrum of the intrarenal artery. a right side: Normal Doppler spectrum. RI 0.60. Intrarenal normal systolic flow velocity (Vmax 44 cm/s).
With a renal arterial trunk embolism, a large portion of the kidney may become anemic and diminished in size, accompanied by an increase in echogenicity (Fig. 9.34).
b left side: Intrarenal low systolic flow velocity (Vmax 23 cm/s), prolonged acceleration time and lowered RI (0.41): renal artery stenosis on the left side.
Arteriosclerosis, Arteriolosclerosis
Arteriolosclerosis (Ischemic Nephropathy)
(Ischemic Nephropathy) 



























While arteriolosclerosis leads to a decrease in renal size with thinning of the cortex, arteriosclerosis causes an irregular surface with areas of parenchymal thinning, but an overall normal renal size. The echogenicity is normal or slightly hyperechoic (due to sclerosis) and the parenchyma is frequently narrowed. The surface appears smooth when arteriolosclerosis is predominant; in arteriosclerosis the surface appears coarse, with a scarred contour, and thickened segmental arteries showing bright double echoes with a central, narrow echofree band can be seen in the renal sinus.
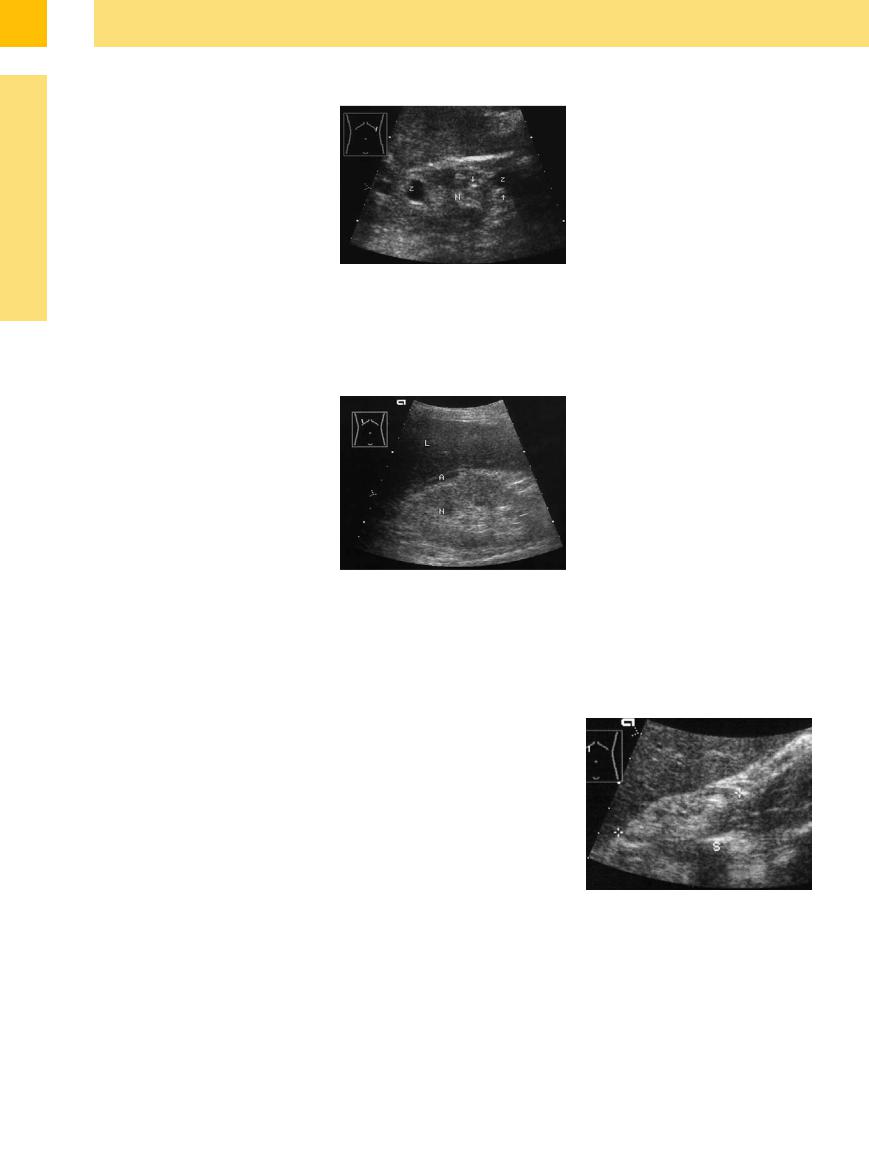
Similar changes are seen as a result of multiple infarcts in panarteritis nodosa (Fig. 9.35).
Fig. 9.35
a Retraction of the kidney surface and parenchymal scars and rarefaction by arteriosclerosis.10
Chronic Pyelonephritis 















































Chronic pyelonephritis is a chronic interstitial (bacterial), episodic inflammatory process characterized by the scarring and destruction of renal parenchyma. In bilateral cases that have progressed to a stage requiring dialysis, the kidneys are significantly smaller than normal, especially in their longitudinal dimension.5 Additional features are focal changes such as stones (33%) and cysts (31%) and changes in cortical structure with a significant increase in echogenicity ( 9.2 g). In interstitial renal diseases, a correlation exists between the echogenicity of the renal cortex and histological changes such as sclerosis, tubular atrophy, hyaline casts, and focal leukocyte infiltration.6
9.2 g). In interstitial renal diseases, a correlation exists between the echogenicity of the renal cortex and histological changes such as sclerosis, tubular atrophy, hyaline casts, and focal leukocyte infiltration.6
A small or atrophic kidney in pyelonephritis is more commonly unilateral than bilateral, and it can be difficult in these cases to establish a cause. In the advanced stage of renal atrophy when the longitudinal size of the kidney has dwindled to approximately 6–7 cm, ultrasound is generally no longer helpful in diagnosing the cause. In addition to these changes, abscesses may form in the renal pelvis, appearing as hypoechoic masses. This is especially common in diabetics with an acute infection (Fig. 9.36,
Fig. 9.61,  9.5 d).
9.5 d).
b Wall thickening of the renal segmental artery (probably equivalent to fibrosis/sclerosis, arrow): hyperechoic double band with a central anechoic lumen.10
Fig. 9.36 Reduced kidney (84.5 mm, cursors) focal hyperechoic scars (arrows). Clinically: recurrent chronic pyelonephritis, ultimately with insufficiency.
335
9
Kidneys
Analgesic Nephropathy















































The term analgesic nephropathy refers to a chronic, noninfective, interstitial, bilateral nephritis that is incited by the use of analgesic medication. The histological features are a lu- men-occluding capillary sclerosis, tubular and papillary necrosis, and papillary necrosis with calcification of the papillary tips.
The sonographic features reflect the histological changes in the form of decreased renal size, increased echogenicity, wavy contours, and fine calcifications at the tips of the medullary pyramids. Some cases present with secondary microcysts, usually resulting from the cystic degeneration of medullary pyramids, or with tubular retention cysts (detectable in 50% of cases) (Fig. 9.37).7
Fig. 9.37 Analgesic nephropathy (N). Marked parenchymal rarefaction with a hazy structure and fine calcifications projected over the papillary tips (arrows). Secondary cyst (Z). Patient had a 30-year history of daily analgesic use and known pyelonephritis. Creatinine 4.8 mmol/L. Harmonic imaging.
Chronic Glomerulonephritis 












































Chronic glomerulonephritis and diabetic nephropathy (glomerulosclerosis) are both characterized by a decrease in renal size that does not occur until an advanced stage. In both diseases, the longitudinal diameter of the kidney is within normal limits in patients who have reached the dialysis stage.7 The authors found cystic lesions in 14% of cases.
Sonographically, the kidney shows markedly increased echogenicity due to glomerular hyalinization and tubular atrophy. The medullary pyramids may still be appreciated as hypoechoic areas, but in most cases they disappear owing to histologically demonstrable tubular atrophy. In advanced stages the renal structural changes may no longer be helpful in identifying the cause of the disease (Figs. 9.38, 9.41, 9.42).
Fig. 9.38 Small, hyperechoic right kidney (N) due to an unknown cause. Left-sided hydronephrosis (following ureteral ligation). Renal failure with creatinine of 5.6 mg/dL. L = liver; A = ascites.
Diabetic Nephropathy
















































In our own observations of diabetics with nephropathy, we found that the renal volumes in diabetic nephropathy patients with stage I–IV disease2 (Table 9.3) were consistently above normal, with volumes in excess of 200 mL. In stage V disease, the kidneys return to either a normal or slightly decreased size, and small kidneys are not seen until the later dialysis stage.
Ultrasound at that stage demonstrates rarefied areas in the cortex and increased echogenicity. Microcysts are also found, consisting mainly of medullary pyramids that have undergone cystic degeneration. The end stage is marked by atrophic kidneys with complete parenchymal destruction, and the genesis of the disease can no longer be determined by sonographic findings (Fig. 9.39).
Fig. 9.39 Atrophic kidney (cursors) in diabetic nephropathy requiring dialysis. The kidney, which is very difficult to identify, has an irregular structure and contains calcifications with acoustic shadows (S).
336
Kidneys

Anomalies, Malformations
Diffuse Changes
Large Kidneys
Small Kidneys
Hypoechoic Structure
Hyperechoic Structure
Irregular Structure
Circumscribed Changes
Acute Renal Failure
Acute Nephritis
Right Ventricular Failure
Renal Vein Thrombosis
renal size. Thus, some of the following disornoted that while the features listed are suggestect the disease in question.
Acute Renal Failure 

















































If there are any characteristic changes in acute renal failure, they are renal enlargement and decreased echogenicity. In many cases, however, no significant abnormalities are seen (Fig. 9.25).
Acute Nephritis 



















































Besides renal enlargement, decreased parenchymal echogenicity is frequently seen as a result of inflammatory edema (Fig. 9.29).
Right Ventricular Failure 














































Characteristic features are enlargement and decreased echogenicity, accompanied by congestion of the vena cava and renal veins (Fig. 9.27).
Renal Vein Thrombosis
Thrombosis 















































Renal vein thrombosis may be unilateral or bilateral. Besides the enlargement noted above, the renal parenchyma generally appears hypoechoic (Fig. 9.28). Color Doppler evaluation and above all CEUS of the renal veins are definitive for the diagnosis of renal vein thrombosis.
9
Diffuse Changes
337