

- •Contents
- •Preface
- •Contributors
- •1 Vessels
- •1.1 Aorta, Vena Cava, and Peripheral Vessels
- •Aorta, Arteries
- •Anomalies and Variant Positions
- •Dilatation
- •Stenosis
- •Wall Thickening
- •Intraluminal Mass
- •Perivascular Mass
- •Vena Cava, Veins
- •Anomalies
- •Dilatation
- •Intraluminal Mass
- •Compression, Infiltration
- •1.2 Portal Vein and Its Tributaries
- •Enlarged Lumen Diameter
- •Portal Hypertension
- •Intraluminal Mass
- •Thrombosis
- •Tumor
- •2 Liver
- •Enlarged Liver
- •Small Liver
- •Homogeneous Hypoechoic Texture
- •Homogeneous Hyperechoic Texture
- •Regionally Inhomogeneous Texture
- •Diffuse Inhomogeneous Texture
- •Anechoic Masses
- •Hypoechoic Masses
- •Isoechoic Masses
- •Hyperechoic Masses
- •Echogenic Masses
- •Irregular Masses
- •Differential Diagnosis of Focal Lesions
- •Diagnostic Methods
- •Suspected Diagnosis
- •3 Biliary Tree and Gallbladder
- •3.1 Biliary Tree
- •Thickening of the Bile Duct Wall
- •Localized and Diffuse
- •Bile Duct Rarefaction
- •Localized and Diffuse
- •Bile Duct Dilatation and Intraductal Pressure
- •Intrahepatic
- •Hilar and Prepancreatic
- •Intrapancreatic
- •Papillary
- •Abnormal Intraluminal Bile Duct Findings
- •Foreign Body
- •The Seven Most Important Questions
- •3.2 Gallbladder
- •Changes in Size
- •Large Gallbladder
- •Small/Missing Gallbladder
- •Wall Changes
- •General Hypoechogenicity
- •General Hyperechogenicity
- •General Tumor
- •Focal Tumor
- •Intraluminal Changes
- •Hyperechoic
- •Hypoechoic
- •Nonvisualized Gallbladder
- •Missing Gallbladder
- •Obscured Gallbladder
- •4 Pancreas
- •Diffuse Pancreatic Change
- •Large Pancreas
- •Small Pancreas
- •Hypoechoic Texture
- •Hyperechoic Texture
- •Focal Changes
- •Anechoic Lesion
- •Hypoechoic Lesion
- •Isoechoic Lesion
- •Hyperechoic Lesion
- •Irregular (Complex Structured) Lesion
- •Dilatation of the Pancreatic Duct
- •Marginal/Mild Dilatation
- •Marked Dilatation
- •5 Spleen
- •Nonfocal Changes of the Spleen
- •Diffuse Parenchymal Changes
- •Large Spleen
- •Small Spleen
- •Focal Changes of the Spleen
- •Anechoic Mass
- •Hypoechoic Mass
- •Hyperechoic Mass
- •Splenic Calcification
- •6 Lymph Nodes
- •Peripheral Lymph Nodes
- •Head/Neck
- •Extremities (Axilla, Groin)
- •Abdominal Lymph Nodes
- •Porta Hepatis
- •Splenic Hilum
- •Mesentery (Celiac, Upper and Lower Mesenteric Station)
- •Stomach
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •Small/Large Intestine
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •8 Peritoneal Cavity
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Wall Structures
- •Smooth Margin
- •Irregular Margin
- •Intragastric Processes
- •Intraintestinal Processes
- •9 Kidneys
- •Anomalies, Malformations
- •Aplasia, Hypoplasia
- •Cystic Malformation
- •Anomalies of Number, Position, or Rotation
- •Fusion Anomaly
- •Anomalies of the Renal Calices
- •Vascular Anomaly
- •Diffuse Changes
- •Large Kidneys
- •Small Kidneys
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Irregular Structure
- •Circumscribed Changes
- •Anechoic Structure
- •Hypoechoic or Isoechoic Structure
- •Complex Structure
- •Hyperechoic Structure
- •10 Adrenal Glands
- •Enlargement
- •Anechoic Structure
- •Hypoechoic Structure
- •Complex Echo Structure
- •Hyperechoic Structure
- •11 Urinary Tract
- •Malformations
- •Duplication Anomalies
- •Dilatations and Stenoses
- •Dilated Renal Pelvis and Ureter
- •Anechoic
- •Hypoechoic
- •Hypoechoic
- •Hyperechoic
- •Large Bladder
- •Small Bladder
- •Altered Bladder Shape
- •Intracavitary Mass
- •Hypoechoic
- •Hyperechoic
- •Echogenic
- •Wall Changes
- •Diffuse Wall Thickening
- •Circumscribed Wall Thickening
- •Concavities and Convexities
- •12.1 The Prostate
- •Enlarged Prostate
- •Regular
- •Irregular
- •Small Prostate
- •Regular
- •Echogenic
- •Circumscribed Lesion
- •Anechoic
- •Hypoechoic
- •Echogenic
- •12.2 Seminal Vesicles
- •Diffuse Change
- •Hypoechoic
- •Circumscribed Change
- •Anechoic
- •Echogenic
- •Irregular
- •12.3 Testis, Epididymis
- •Diffuse Change
- •Enlargement
- •Decreased Size
- •Circumscribed Lesion
- •Anechoic or Hypoechoic
- •Irregular/Echogenic
- •Epididymal Lesion
- •Anechoic
- •Hypoechoic
- •Intrascrotal Mass
- •Anechoic or Hypoechoic
- •Echogenic
- •13 Female Genital Tract
- •Masses
- •Abnormalities of Size or Shape
- •Uterus
- •Abnormalities of Size or Shape
- •Myometrial Changes
- •Intracavitary Changes
- •Endometrial Changes
- •Fallopian Tubes
- •Hypoechoic Mass
- •Anechoic Cystic Mass
- •Solid Echogenic or Nonhomogeneous Mass
- •14 Thyroid Gland
- •Diffuse Changes
- •Enlarged Thyroid Gland
- •Small Thyroid Gland
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Circumscribed Changes
- •Anechoic
- •Hypoechoic
- •Isoechoic
- •Hyperechoic
- •Irregular
- •Differential Diagnosis of Hyperthyroidism
- •Types of Autonomy
- •15 Pleura and Chest Wall
- •Chest Wall
- •Masses
- •Parietal Pleura
- •Nodular Masses
- •Diffuse Pleural Thickening
- •Pleural Effusion
- •Anechoic Effusion
- •Echogenic Effusion
- •Complex Effusion
- •16 Lung
- •Masses
- •Anechoic Masses
- •Hypoechoic Masses
- •Complex Masses
- •Index
11 Urinary Tract
Urinary Tract |
381 |
||||
|
Malformations |
383 |
|||
|
|||||
|
|
|
Duplication Anomalies |
383 |
|
|
|
|
|||
|
|
|
|
Duplex Kidney |
|
|
|
|
|
|
|
|
|
|
|
Duplex Ureter |
|
|
|
|
|
|
|
|
|
|
|
Bifid Ureter |
|
|
|
Dilatations and Stenoses |
384 |
||
Caliceal and Ureteral Diverticula Megacalicosis
Ureteropelvic Junction Obstruction Ureterovesical Junction Obstruction (Megaureter)
|
Dilated Renal Pelvis and Ureter |
386 |
|||||
|
|||||||
|
|
|
Anechoic |
386 |
|||
|
|
|
|||||
|
|
|
|
|
|
Pyelectasis |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
Subpelvic Ureteral Stenosis |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
Urinary Stone Colic |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
Chronic Urinary Stasis |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
Retroperitoneal Fibrosis |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
(Ormond Disease) |
|
|
|
|
|
|
|
Reflux |
|
|
|
|
Hypoechoic |
392 |
|||
|
|
|
|
|
|
Hemorrhage (Traumatic, Clot) |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
Infected Obstruction |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Suppurative Pyelitis |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
Pyonephrosis |
|
|
Renal Pelvic Mass, Ureteral Mass |
394 |
|||||
|
|||||||
|
|
|
Hypoechoic |
394 |
|||
|
|
|
|||||
|
|
|
|
|
|
Urothelial Carcinoma |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Ureteral Clots |
|
|
|
|
Hyperechoic |
395 |
|||
|
|
|
|
|
|
Caliceal Stones |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Renal Pelvic Stone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Staghorn Calculus |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Ureteral Stone |
|
|
Changes in Bladder Size or Shape |
398 |
|||||
|
|||||||
|
|
|
Large Bladder |
398 |
|||
|
|
|
|||||
|
|
|
|
|
|
Urinary Retention |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Overflow Bladder, |
|
|
|
|
|
|
|
Neurogenic Bladder |
|
|
|
|
Small Bladder |
400 |
|||
|
|
|
|||||
|
|
|
|
|
|
Empty Bladder |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Residual Urine |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Shrunken Bladder |
|
|
|
|
Altered Bladder Shape |
401 |
|||
Partially Contracted Bladder
Diverticulum, Pseudodiverticulum
Indented Bladder,
Operated Bladder
|
Intracavitary Mass |
402 |
|||
|
|||||
|
|
Hypoechoic |
402 |
||
|
|
||||
|
|
|
|
Blood Clots |
|
|
|
|
|
|
|
|
|
|
|
Bladder Sludge |
|
|
|
|
|
|
|
|
|
|
|
Bladder Papilloma |
|
|
|
|
|
|
|
|
|
|
|
Polypoid Bladder Carcinoma |
|
|
|
|
|
|
|
|
|
|
|
Mesenchymal Tumors |
|
|
|
Hyperechoic |
406 |
||
|
|
||||
|
|
|
|
Urinary Catheter |
|
|
|
|
|
|
|
|
|
|
|
Blood Clots |
|
|
|
|
|
|
|
|
|
|
|
Polypoid Bladder Tumor |
|
|
|
|
|
|
|
|
|
|
|
Benign Prostatic Hyperplasia |
|
|
|
|
|
|
|
|
|
|
|
Lipoma, Fibroma, Myoma, |
|
|
|
|
|
|
|
|
|
|
|
Hemangioma |
|
|
|
|
|
Ureterocele |
|
|
|
|
|
|
|
|
|
|
|
Artifacts |
|
|
|
Echogenic |
408 |
||
|
|
|
|
Foreign Bodies |
|
|
|
|
|
|
|
|
|
|
|
Bladder Calculi |
|
|
|
|
|
|
|
|
|
Wall Changes |
410 |
||||
|
|
||||||
|
|
|
Diffuse Wall Thickening |
410 |
|||
|
|
|
|||||
|
|
|
|
|
|
Bladder-Wall Hypertrophy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Flat Bladder Tumor |
|
|
|
|
Circumscribed Wall Thickening |
411 |
|||
|
|
|
|||||
|
|
|
|
|
|
Bladder-Wall Hypertrophy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Bladder-Wall Edema |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Bladder Carcinoma |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Blood Clots |
|
|
|
|
|
Concavities and Convexities |
413 |
||
|
|
|
|
||||
|
|
|
|
|
|
Ureteroceles |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Diverticula |
|
11 Urinary Tract
G. Schmidt
The excretory portion of the urinary tract be- |
open into the minor calices at the tips of the |
||
gins with the collecting ducts of the renal pa- |
papillae. The papillae are lined with a single |
||
renchyma, where the secondary urine is |
layer of epithelium that becomes stratified in |
||
formed through reabsorption. |
These |
ducts |
its further course and lines a total of 8–10 |
unite to form 10–30 papillary |
ducts, |
which |
minor calices, which collect the urine like fun- |
nels. They unite to form major calices, from which urine drains into the renal pelvis and thence to the ureter, bladder, and urethra.
Anatomy























































Shapes and sizes
●Shape of the renal pelvis
●Ureteral length and diameter
●Shape, volume, and size of the urinary bladder
Shape of the renal pelvis. The renal pelvis presents a spectrum of shapes ranging from the tubular (dendritic) form to the sac-like “ampullary” form. The latter type usually appears as a fluid-filled space in ultrasound, whereas the normal, non–fluid-filled pyelocaliceal system is not visible sonographically.
The renal pelvis is lined by a thin mucosa composed of special stratified, transitional epithelium (“urothelium,” which also lines the ureter and bladder) and a muscular layer composed of smooth muscle fibers. The mucosa can be distinguished from the renal sinus echo complex only when it is inflamed and swollen or when the pyelocaliceal system is filled with fluid (Fig.11.1).
Ureteral length and diameter. The ureter similarly consists of an inner layer of mucosa, an
intermediate layer of smooth muscle fibers, and an outer adventitial layer. Normally it is not visualized with ultrasound because of the lack of contrast with the surrounding retroperitoneal tissue. The ureter is 30 cm long and 4–7 mm in diameter.
Shape, volume, and size of the bladder. The bladder wall consists of a thick muscular coat along with a mucous and submucous layer and a serosal layer. The three-layered structure of the bladder wall can be recognized in ultrasound, especially in relation to the fluid-filled lumen.
The body or corpus of the bladder forms the anterosuperior roof, and the base or fundus of the bladder forms the posteroinferior floor. From the fundus, the bladder tapers in a funnel shape across the bladder neck to the urethra, which opens at the apex of the bladder trigone. The ureters pierce the muscular bladder wall and enter the bladder lumen at the ureteral orifices, located at the lateral angles of the trigone on the posterior wall of the fundus (Fig.11.2, Fig.11.3). Sonographically, the submucous segments of the ureters appear as
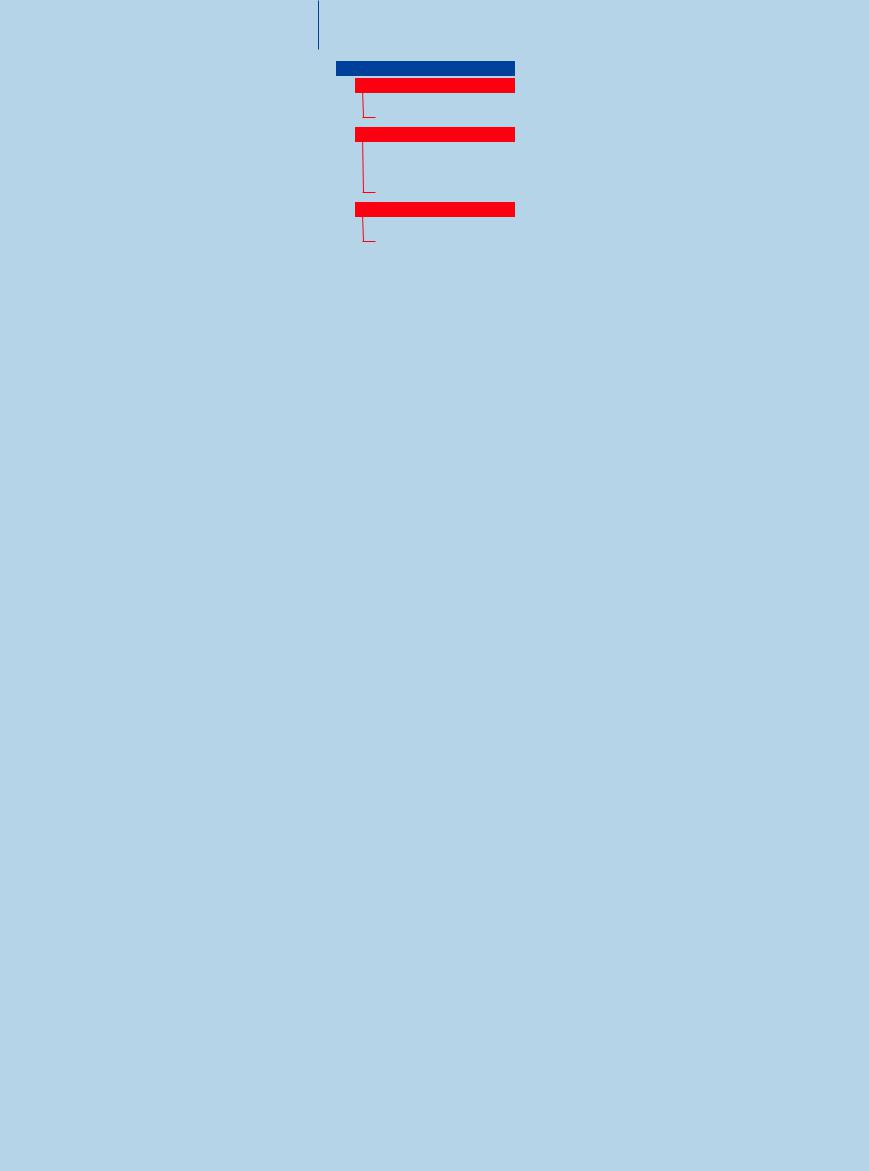
Fig. 11.2 Urinary bladder. |
b Full bladder in a longitudinal scan through the lower |
a Normal full bladder (HB) in a transverse scan through |
abdomen: oval shape with a tapered anterosuperior roof |
the lower abdomen: squared-off shape with rounded |
and posteroinferior floor. Normal wall thickness (cursors). |
corners. |
|
Fig. 11.1 Acute suppurative pyelitis with pelvic dilatation and hypoechoic wall thickening (cursors).
prominent ureteral ridges that protrude into the bladder lumen (Fig.11.3).
The size of the bladder depends on its degree of distension. This also determines the shape of the bladder, which may appear round, squared with rounded corners, or elliptical (Fig.11.2). The wall thickness of the full bladder is 1–3 mm. An urge to urinate is felt when the bladder is filled to approximately 350 mL, but the bladder can easily accommodate twice that volume.
c Diagram showing the anatomy and relations of the bladder, seminal vesicles, urethra, and prostate.
11
Urinary Tract
381
11
Urinary Tract
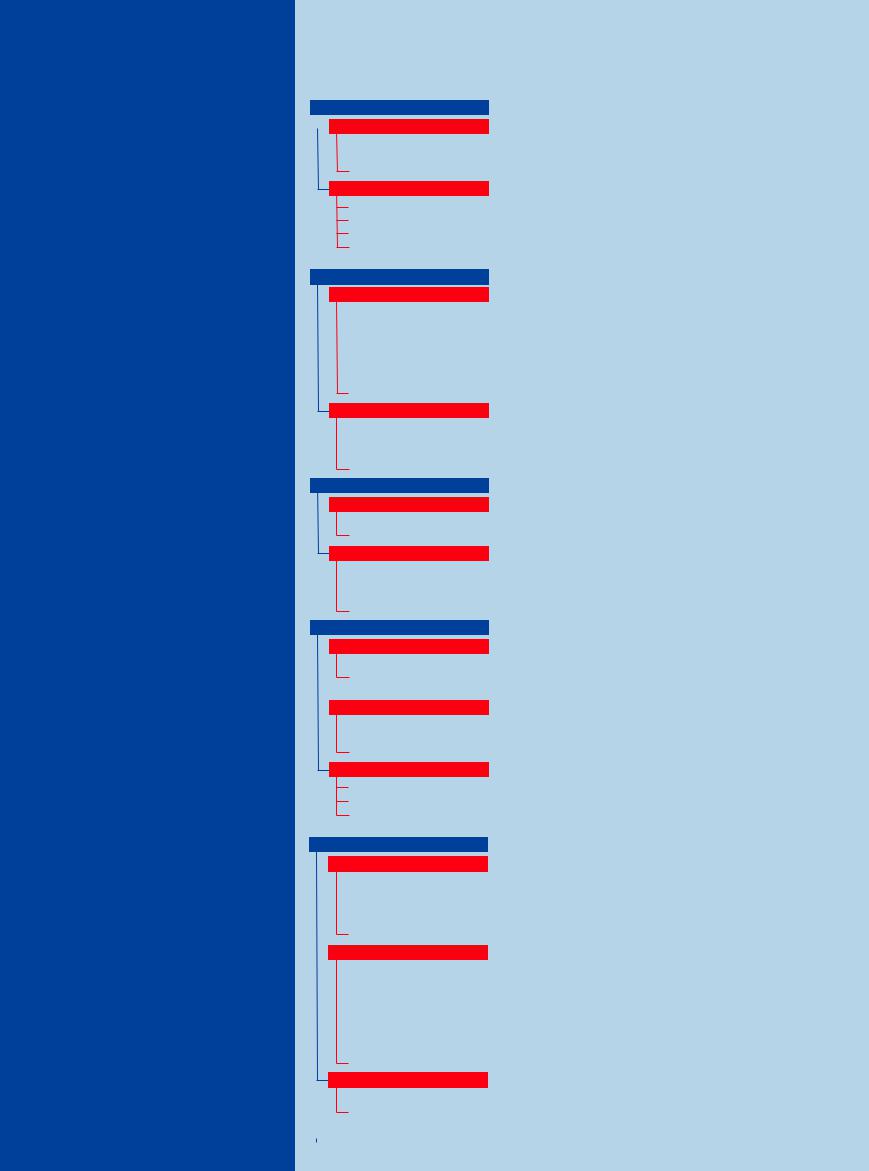
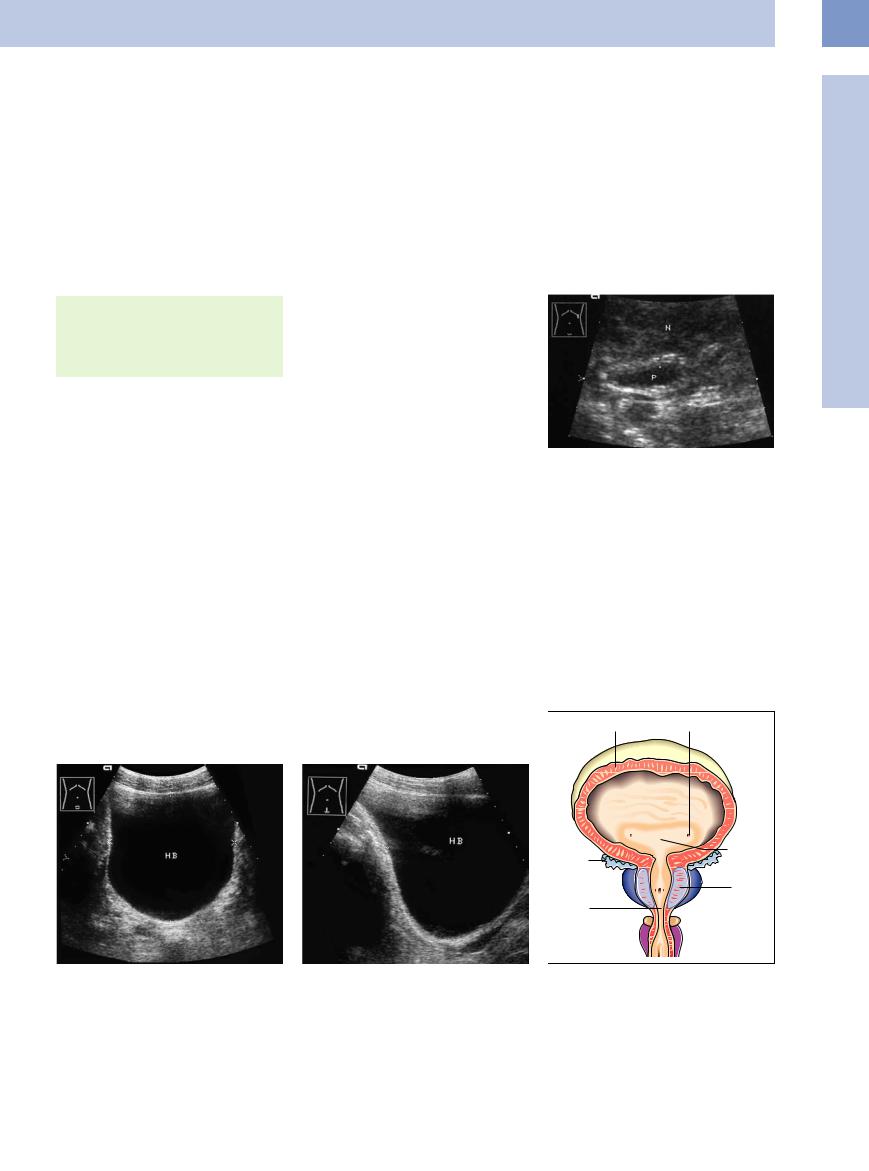
Fig. 11.3 Ureteral orifices at the lateral angles of the trigone (arrows) with a prominent “ureteral bud.” SB = seminal vesicle; R = rectum; HB = urinary bladder; P = pelvis.
a Transverse scan.
b Longitudinal scan.
Topography 






























Locations
●Ureteropelvic junction
●Ureter anterior to the iliac vessels
●Prevesical ureter
●Bladder in the lesser pelvis
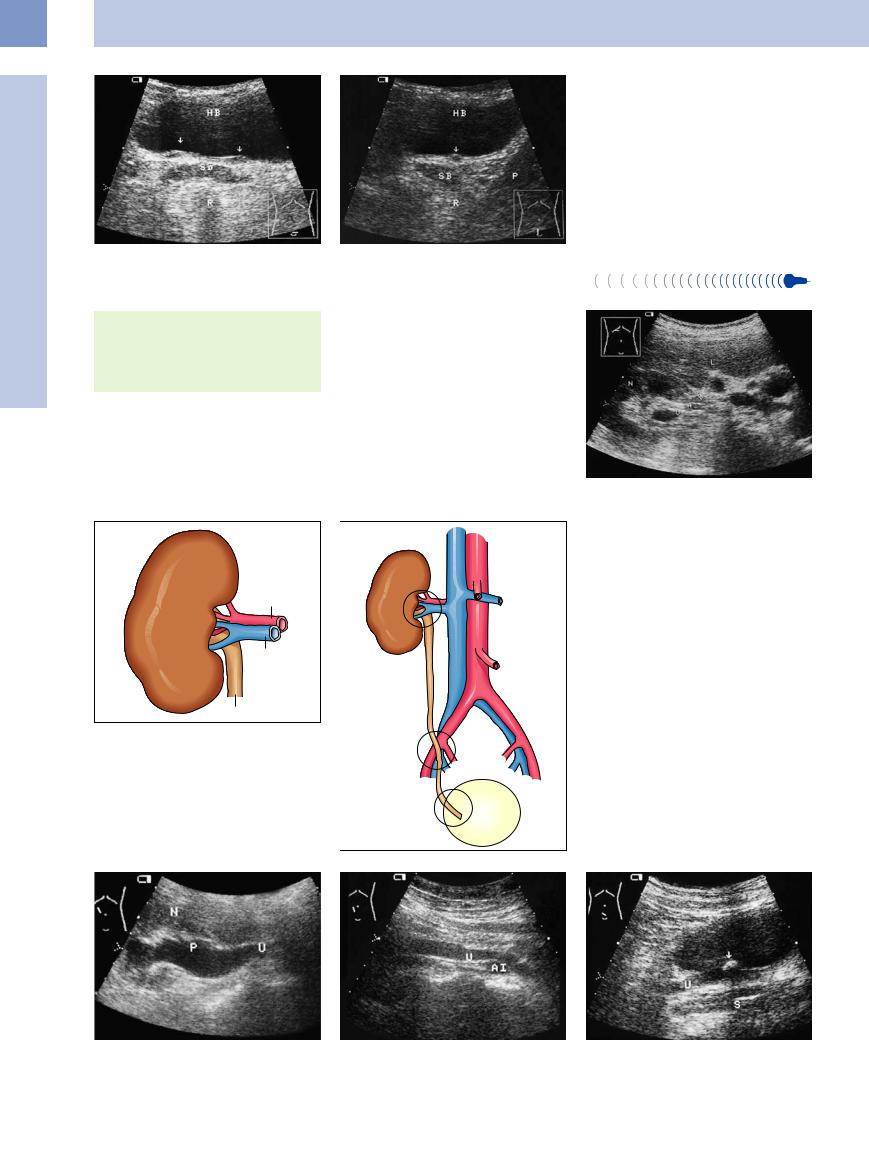
Ureteropelvic junction and course of the ureter. The ureter leaves the renal hilum posterior to the renal vein and artery. Hence it is best to scan the ureter from behind with the ultrasound beam directed anteriorly (Fig.11.4, Fig.11.5). The ureter descends anteriorly to
Fig. 11.5 Course and relations of the ureter. a Proximal ureter.
the iliopsoas muscle, following the lordotic curvature of the lumbar spine. Initially it takes a steep anterior and inferomedial course, then turns distally toward the lateral border of the bladder. As it descends, it crosses over the iliac vessels at the level of the origin of the deep iliac artery, follows the wall of the lesser pelvis, and finally opens into the bladder at the laterobasal ureteral ridges (Fig.11.5).
Bladder. Figure 11.3 and Fig.11.6 illustrate the relations of the bladder to the organs of the lesser pelvis and to the male reproductive tract.
Fig. 11.4 Transverse scan of the right kidney (N). From anterior to posterior: the renal vein (V) followed by the renal artery (A) and upper ureter (U). L = liver.
fb Course from the renal pelvis to the bladder trigone. 1 = ureteropelvic junction area; 2 = ureter crossing over the iliac vessels; 3 = supravesical segment.
c–e Course of the ureter (U) is visualized by ultrasound due to obstruction by a prevesical ureteral stone (arrow); acoustic shadow (S).
c Junction of the ureter (U) with the dilated renal pelvis |
d Ureteral segment anterior to the iliac artery (AI). |
e Prevesical ureter. |
(P). N = kidney. |
|
|
382