

- •Contents
- •Preface
- •Contributors
- •1 Vessels
- •1.1 Aorta, Vena Cava, and Peripheral Vessels
- •Aorta, Arteries
- •Anomalies and Variant Positions
- •Dilatation
- •Stenosis
- •Wall Thickening
- •Intraluminal Mass
- •Perivascular Mass
- •Vena Cava, Veins
- •Anomalies
- •Dilatation
- •Intraluminal Mass
- •Compression, Infiltration
- •1.2 Portal Vein and Its Tributaries
- •Enlarged Lumen Diameter
- •Portal Hypertension
- •Intraluminal Mass
- •Thrombosis
- •Tumor
- •2 Liver
- •Enlarged Liver
- •Small Liver
- •Homogeneous Hypoechoic Texture
- •Homogeneous Hyperechoic Texture
- •Regionally Inhomogeneous Texture
- •Diffuse Inhomogeneous Texture
- •Anechoic Masses
- •Hypoechoic Masses
- •Isoechoic Masses
- •Hyperechoic Masses
- •Echogenic Masses
- •Irregular Masses
- •Differential Diagnosis of Focal Lesions
- •Diagnostic Methods
- •Suspected Diagnosis
- •3 Biliary Tree and Gallbladder
- •3.1 Biliary Tree
- •Thickening of the Bile Duct Wall
- •Localized and Diffuse
- •Bile Duct Rarefaction
- •Localized and Diffuse
- •Bile Duct Dilatation and Intraductal Pressure
- •Intrahepatic
- •Hilar and Prepancreatic
- •Intrapancreatic
- •Papillary
- •Abnormal Intraluminal Bile Duct Findings
- •Foreign Body
- •The Seven Most Important Questions
- •3.2 Gallbladder
- •Changes in Size
- •Large Gallbladder
- •Small/Missing Gallbladder
- •Wall Changes
- •General Hypoechogenicity
- •General Hyperechogenicity
- •General Tumor
- •Focal Tumor
- •Intraluminal Changes
- •Hyperechoic
- •Hypoechoic
- •Nonvisualized Gallbladder
- •Missing Gallbladder
- •Obscured Gallbladder
- •4 Pancreas
- •Diffuse Pancreatic Change
- •Large Pancreas
- •Small Pancreas
- •Hypoechoic Texture
- •Hyperechoic Texture
- •Focal Changes
- •Anechoic Lesion
- •Hypoechoic Lesion
- •Isoechoic Lesion
- •Hyperechoic Lesion
- •Irregular (Complex Structured) Lesion
- •Dilatation of the Pancreatic Duct
- •Marginal/Mild Dilatation
- •Marked Dilatation
- •5 Spleen
- •Nonfocal Changes of the Spleen
- •Diffuse Parenchymal Changes
- •Large Spleen
- •Small Spleen
- •Focal Changes of the Spleen
- •Anechoic Mass
- •Hypoechoic Mass
- •Hyperechoic Mass
- •Splenic Calcification
- •6 Lymph Nodes
- •Peripheral Lymph Nodes
- •Head/Neck
- •Extremities (Axilla, Groin)
- •Abdominal Lymph Nodes
- •Porta Hepatis
- •Splenic Hilum
- •Mesentery (Celiac, Upper and Lower Mesenteric Station)
- •Stomach
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •Small/Large Intestine
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •8 Peritoneal Cavity
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Wall Structures
- •Smooth Margin
- •Irregular Margin
- •Intragastric Processes
- •Intraintestinal Processes
- •9 Kidneys
- •Anomalies, Malformations
- •Aplasia, Hypoplasia
- •Cystic Malformation
- •Anomalies of Number, Position, or Rotation
- •Fusion Anomaly
- •Anomalies of the Renal Calices
- •Vascular Anomaly
- •Diffuse Changes
- •Large Kidneys
- •Small Kidneys
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Irregular Structure
- •Circumscribed Changes
- •Anechoic Structure
- •Hypoechoic or Isoechoic Structure
- •Complex Structure
- •Hyperechoic Structure
- •10 Adrenal Glands
- •Enlargement
- •Anechoic Structure
- •Hypoechoic Structure
- •Complex Echo Structure
- •Hyperechoic Structure
- •11 Urinary Tract
- •Malformations
- •Duplication Anomalies
- •Dilatations and Stenoses
- •Dilated Renal Pelvis and Ureter
- •Anechoic
- •Hypoechoic
- •Hypoechoic
- •Hyperechoic
- •Large Bladder
- •Small Bladder
- •Altered Bladder Shape
- •Intracavitary Mass
- •Hypoechoic
- •Hyperechoic
- •Echogenic
- •Wall Changes
- •Diffuse Wall Thickening
- •Circumscribed Wall Thickening
- •Concavities and Convexities
- •12.1 The Prostate
- •Enlarged Prostate
- •Regular
- •Irregular
- •Small Prostate
- •Regular
- •Echogenic
- •Circumscribed Lesion
- •Anechoic
- •Hypoechoic
- •Echogenic
- •12.2 Seminal Vesicles
- •Diffuse Change
- •Hypoechoic
- •Circumscribed Change
- •Anechoic
- •Echogenic
- •Irregular
- •12.3 Testis, Epididymis
- •Diffuse Change
- •Enlargement
- •Decreased Size
- •Circumscribed Lesion
- •Anechoic or Hypoechoic
- •Irregular/Echogenic
- •Epididymal Lesion
- •Anechoic
- •Hypoechoic
- •Intrascrotal Mass
- •Anechoic or Hypoechoic
- •Echogenic
- •13 Female Genital Tract
- •Masses
- •Abnormalities of Size or Shape
- •Uterus
- •Abnormalities of Size or Shape
- •Myometrial Changes
- •Intracavitary Changes
- •Endometrial Changes
- •Fallopian Tubes
- •Hypoechoic Mass
- •Anechoic Cystic Mass
- •Solid Echogenic or Nonhomogeneous Mass
- •14 Thyroid Gland
- •Diffuse Changes
- •Enlarged Thyroid Gland
- •Small Thyroid Gland
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Circumscribed Changes
- •Anechoic
- •Hypoechoic
- •Isoechoic
- •Hyperechoic
- •Irregular
- •Differential Diagnosis of Hyperthyroidism
- •Types of Autonomy
- •15 Pleura and Chest Wall
- •Chest Wall
- •Masses
- •Parietal Pleura
- •Nodular Masses
- •Diffuse Pleural Thickening
- •Pleural Effusion
- •Anechoic Effusion
- •Echogenic Effusion
- •Complex Effusion
- •16 Lung
- •Masses
- •Anechoic Masses
- •Hypoechoic Masses
- •Complex Masses
- •Index
15
Pleura and Chest Wall

Chest Wall
Masses
Parietal Pleura
Pleural Effusion
Chest Wall
Rib and Sternal Fractures
Rib and Sternal Metastases
Cutaneous Metastases
Carcinoma of the Chest Wall
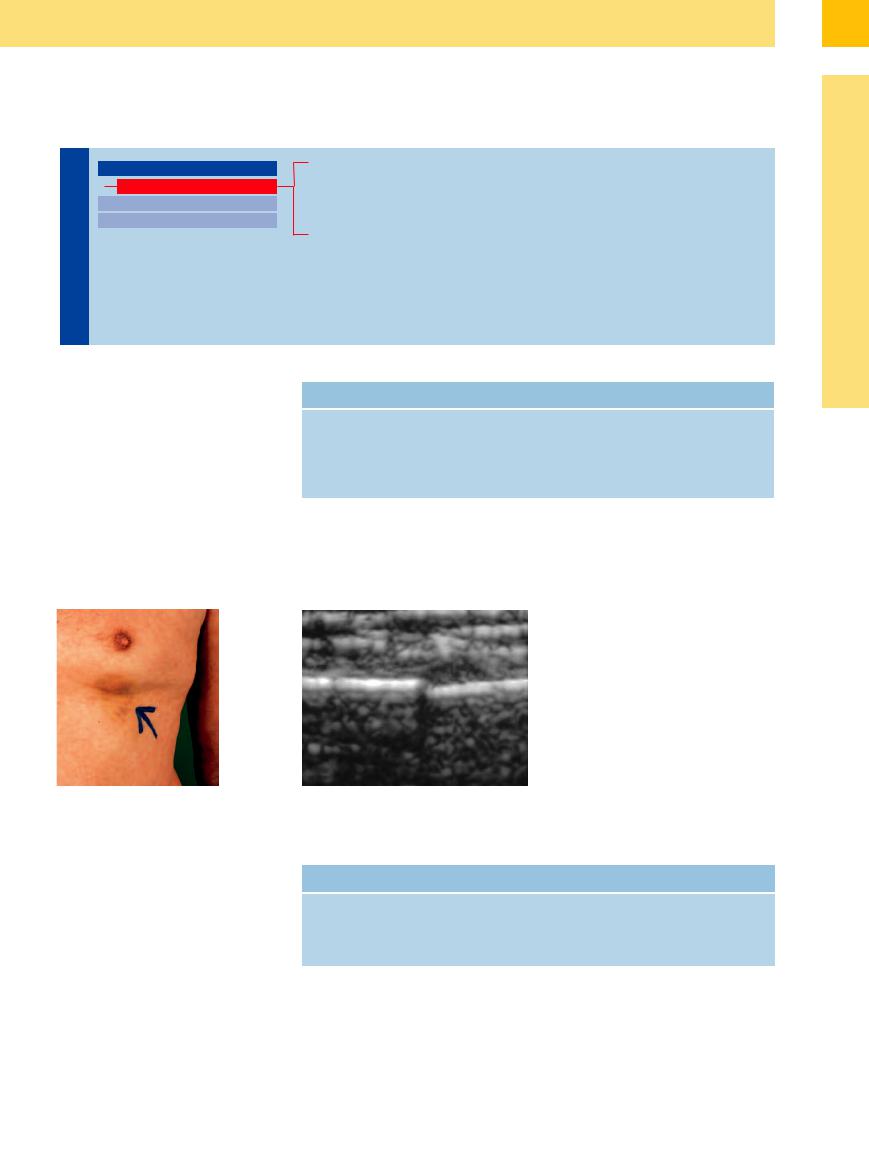
The ultrasound investigation of chest-wall lesions is directed by the physical examination (Fig.15.3). The interpretation depends on the sonographic findings, the clinical data, and also on the result of ultrasound-guided fine-needle aspiration (FNA) or core-needle biopsy. Under the proper conditions, these percutaneous procedures through the chest wall can be done virtually without complications. The main value of chest-wall ultrasound lies in its ability to define the location of masses as intracutaneous, subcutaneous, intramuscular, bony, or pleural.3 The principal masses of the chest wall are reviewed in Table 15.1.
Table 15.1 Differential diagnosis of masses in the chest wall
More common |
Less common |
Rib and sternal fractures |
Abscess |
Cutaneous metastases |
Lipoma |
Rib metastases |
Benign bone tumors |
Carcinoma |
Sarcoma |
|
Malignant mesothelioma |
Fig. 15.3 Fractured rib.
a A man 50 years of age presented with localized leftsided chest pain (arrow) following a fall.
b Minimally displaced rib fracture appears sonographically as a discontinuity in the cortical echo.
Rib and Sternal Fractures














































Bony thoracic lesions can be difficult to diagnose on radiographs because minimally displaced fractures are occasionally obscured by superimposed shadows.
Sonographic features. Fractures of the bony ribs and sternum can be visualized with ultrasound ( 15.2a–c). A discontinuity in the linear cortical echo serves as a direct fracture sign. Indirect fracture signs are local hematoma (
15.2a–c). A discontinuity in the linear cortical echo serves as a direct fracture sign. Indirect fracture signs are local hematoma ( 15.2 d–f) and a pneumothorax or hematothorax. It is not always possible to distinguish between traumatic and pathological fractures
15.2 d–f) and a pneumothorax or hematothorax. It is not always possible to distinguish between traumatic and pathological fractures
Table 15.2 Sonographic fracture signs4
Direct fracture signs
Disruption of the cortical echo
Gap between the bone ends (step-o )
by ultrasound ( 15.2c). The callus that forms during fracture healing can also be defined sonographically (
15.2c). The callus that forms during fracture healing can also be defined sonographically ( 15.2 g–l). The accuracy of
15.2 g–l). The accuracy of
Indirect fracture signs
Local hematoma
Pleural e usion
Pneumothorax
Hematothorax
ultrasound in the diagnosis of thoracic fractures is superior to that of conventional radiographs (Table 15.2).
513
15
Pleura and Chest Wall
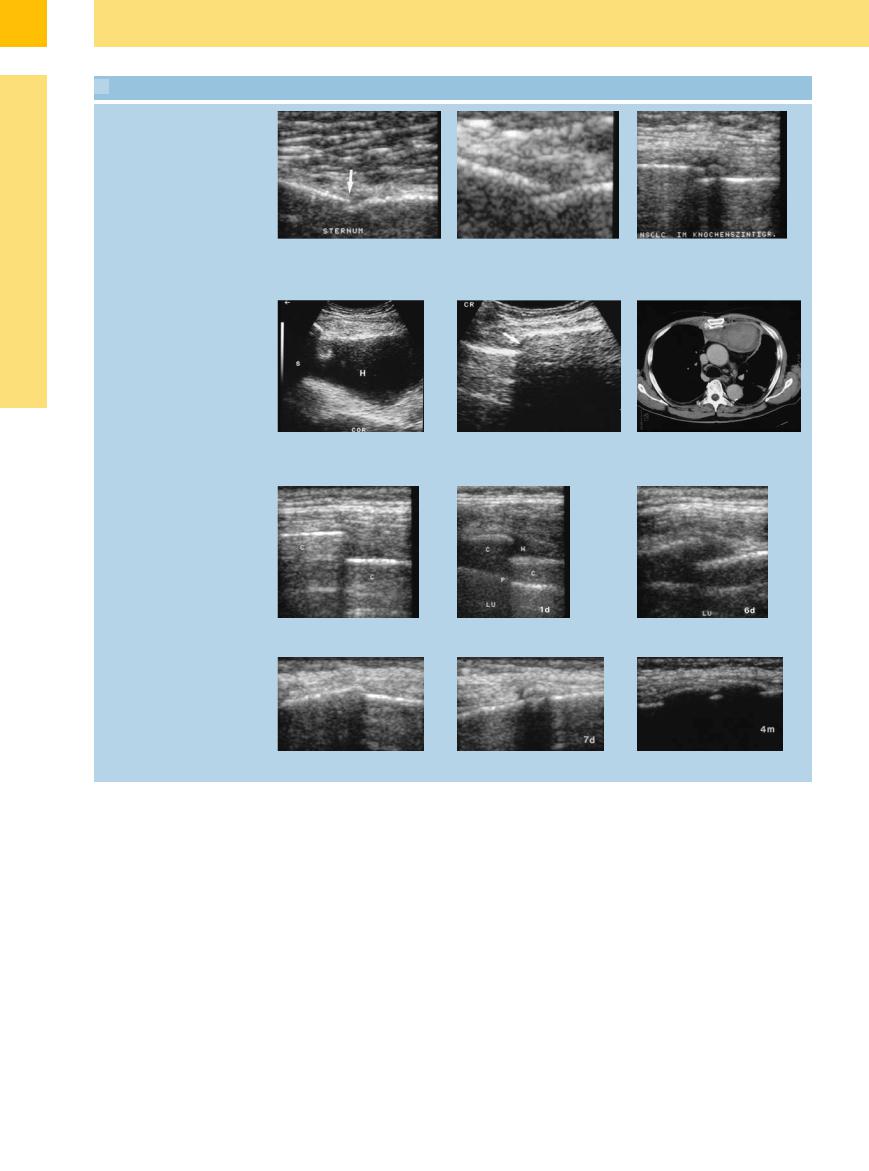
 15.2 Rib Fractures
15.2 Rib Fractures
Direct fracture sign: bony discontinuity
a and b Plasmacytoma, osteoporosis, and chest pain in a 78-year-old woman. Longitudinal scan shows disruption of the sternal cortical echo by a fracture.
Indirect fracture sign: hematoma
d–f Thoracic trauma in an 83-year-old man.
d and e Largely echo-free parasternal mass consistent with a hematoma (H). S = shadowing; COR = heart.
Follow-ups
c Bronchial carcinoma and scintigraphically confirmed rib metastasis in a 52- year-old man. Step-o with soft-tissue lesion consistent with a fracture.
f CT demonstrates a left parasternal hematoma.
g–i A 60-year-old woman with bronchial asthma and chest pain after a fit of coughing. Ultrasound (g) shows a displaced rib fracture. Appearance after 1 day (h) and 1 week (i). H= hematoma; C = rib; P = pleura–lung boundary; LU = lung.
j–l Serial scans document the healing of a traumatic rib fracture with callus formation.
Rib and Sternal Metastases













































The ultrasound examination is directed by the frequent presence of localized pain. It should be noted that, in principle, a benign/malignant differentiation cannot be made based on ultrasound findings alone ( 15.3 l).
15.3 l).
Sonographic features. With metastasis to the bony thorax, ultrasound will often show a rel-
atively long break in the cortical echo ( 15.3a,b,d–f). Some sites allow complete through-transmission of sound waves (
15.3a,b,d–f). Some sites allow complete through-transmission of sound waves ( 15.3i). Tumor extension into the soft tissue is seen with metastatic carcinoma and multiple myeloma (
15.3i). Tumor extension into the soft tissue is seen with metastatic carcinoma and multiple myeloma ( 15.3a,b,i–k). On color Doppler examination, prominent vascular signals are observed in bony metastases (
15.3a,b,i–k). On color Doppler examination, prominent vascular signals are observed in bony metastases ( 15.3k).
15.3k).
Ultrasonography has a limited role in the diagnosis of bony metastases and should be considered only an adjunct to conventional studies.4 It can be helpful in monitoring response to treatment and for planning radiotherapy portals in selected cases.
514
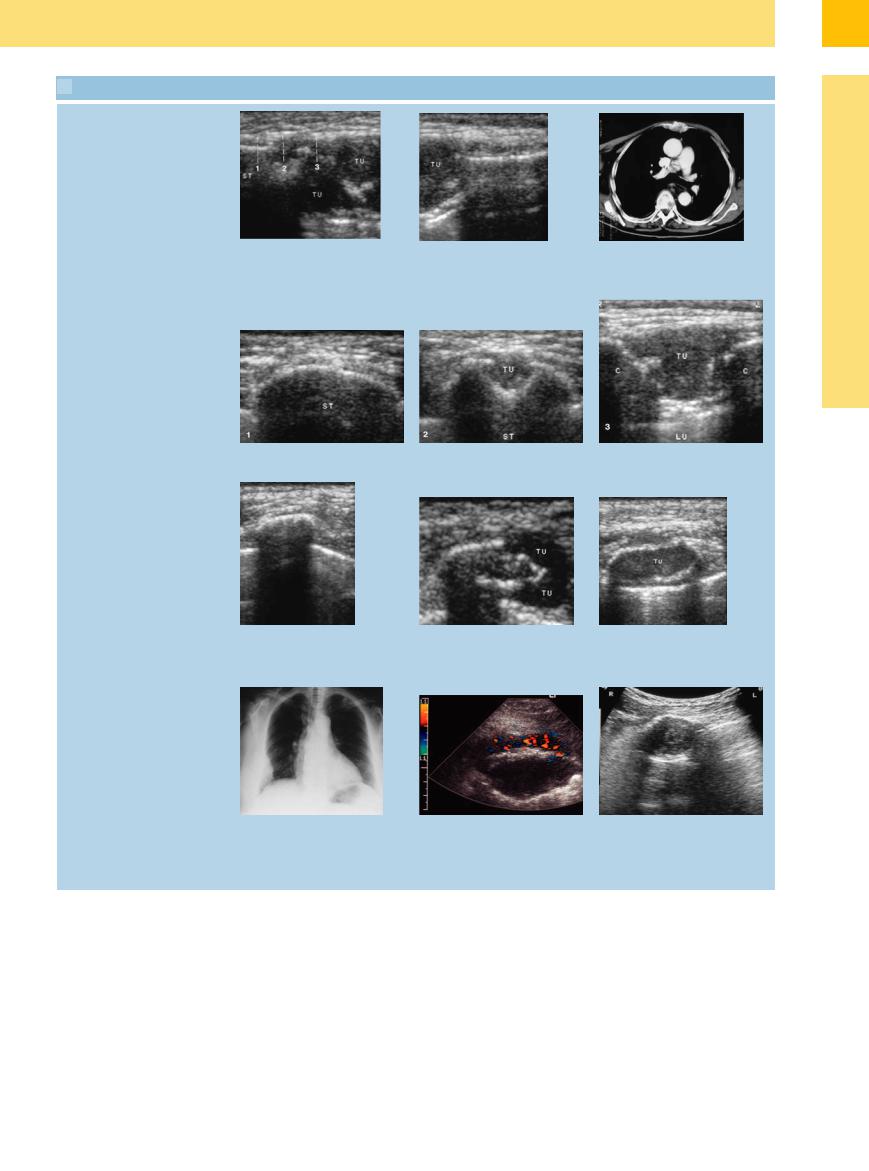
 15.3 Rib and Sternal Metastases
15.3 Rib and Sternal Metastases
Sternal metastasis
a–c Sternal metastasis from bronchial carcinoma. |
c CT appearance of sternal metastasis. |
a and b Longitudinal scan. The sternum has been engulfed and consumed by a |
|
metastasis approximately 5 cm in size. |
|
15
Chest Wall
d–f Transverse scans show varying degrees of destruction including the still-intact sternum and the start of tumor involvement. ST = sternum; TU = tumor; C = rib; LU = lung.
Bone destruction
g–i Normal rib and rib metastasis in |
h Rib metastasis from bronchial carcino- |
transverse section. |
ma. Incipient cortical destruction and |
g Normal rib. |
tumor formation (TU) consistent with a |
|
rib metastasis. |
j–k Plasmacytoma in a 73-year-old wom- |
k Transverse scan of a rib shows cortical |
an. |
destruction and a large soft-tissue mass. |
j Chest radiograph shows a soft-tissue |
TU = tumor; LU = lung. Color Doppler |
lesion in the right lateral chest wall. |
detects flow signals in the tumor tissue. |
i Plasmacytoma (TU) in a 69-year-old man. Almost complete sound transmission through the infiltrated rib, consistent with tumor infiltration.
l Benign di erential diagnosis: 30-year- old man presented with a tumor in the right anterior chest wall. Ultrasound shows a complex solid lesion arising from the rib. Histology: fibrous dysplasia (Ja e–Lichtenstein dysplasia of bone).
Cutaneous Metastases
Metastases 















































The ultrasound investigation of cutaneous metastases is directed by any palpable abnormalities that are noted on physical examination. The palpable mass may have a rounded or flattened shape ( 15.4a–n).
15.4a–n).
A benign tumor (lipoma, granuloma, sebaceous cyst) in any given case can be confirmed only by histological examination ( 15.4o). Lipomas usually present sonographically as
15.4o). Lipomas usually present sonographically as
mobile, hyperechoic lesions with smooth margins. Granulomas are difficult to distinguish from cutaneous metastases by their ultrasound features. Granulomas frequently develop in scarred areas and usually show no vascularity on color Doppler examination.
Cutaneous metastases typically have a round to oval shape and are usually hypoechoic. Flow signals can be detected by color
Doppler. Percutaneous biopsy is almost never performed, because local excision is the method of choice for establishing the diagnosis. For axillary lymph nodes and lymph node metastases see Chapter 6, “Extremities (Axilla, Groin).”
515
15
Pleura and Chest Wall
 15.4 Cutaneous Metastases
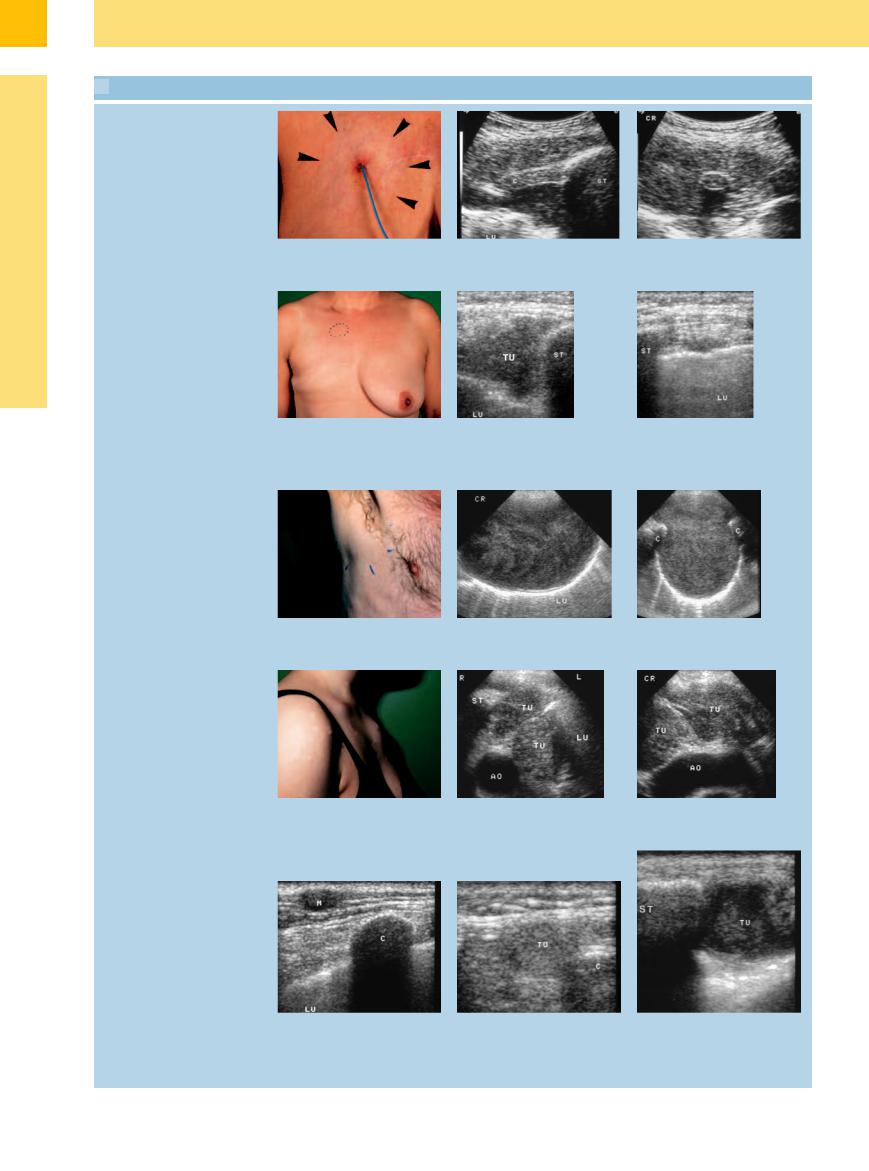
15.4 Cutaneous Metastases
High-grade lymphoma
a An area of palpable induration (arrows) |
b and c Longitudinal and transverse scans show a homogeneous hypoechoic lesion in |
was noted around a Groshong catheter |
the area of the cartilaginous rib (C) junction. Histology confirmed invasion by |
site in a 53-year-old woman. |
lymphoma. LU = lung; ST = sternum. |
Breast carcinoma
d A poorly demarcated area of palpable firmness (dotted circle) was noted in the right parasternal region of a 53-year-old woman.
Plasmacytoma
e Ultrasound shows a triangular hypoechoic lesion (TU) to the right of the sternum (ST), consistent with chest-wall infiltration by known breast carcinoma. LU = lung.
f Left parasternal region appears normal. LU = lung; ST = sternum; TU = tumor.
g Palm-size mass in the right lateral chest wall of a 64-year-old man.
h and i Longitudinal and transverse scans show a large, hypoechoic mass. The ribs (C) appear normal. Histology confirmed soft-tissue infiltration by plasmacytoma. LU = lung.
Hodgkin disease
j Left parasternal swelling in a 20-year-old woman.
k and l Multiple nodular chest-wall tumors arising from the anterior mediastinum (TU). Diagnosis was confirmed by ultrasound-guided core biopsy. ST = sternum; AO = aorta; LU = lung.
Bronchial carcinoma and liposarcoma
m A 53-year-old man with bronchial carcinoma and a subcutaneous nodule on the left side of the chest. Ultrasound reveals a hypoechoic cutaneous metastasis (M). C = rib; LU = lung.
n A 65-year-old man with a firm mass in the left posterior chest wall. Ultrasound shows a rounded, echogenic tumor mass (TU). Excision confirmed the diagnosis of liposarcoma. C= rib.
o Di erentiation from benign lesions: tuberculous abscess in a 30-year-old HIVpositive man. Transverse and longitudinal ultrasound scans show a left parasternal mass (TU) that is fluctuant on compression.
516
15
Chest Wall
and infiltrates neighboring tissues (nerve plexus, rib, spinal column; Fig.15.5).5
Other malignant tumors of the chest wall, such as sarcomas and malignant lymphomas, have a similar sonographic appearance. Ultra- sound-guided percutaneous biopsy is the method of choice for confirming the diagnosis.
Fig. 15.4 Bronchial carcinoma in a 78-year-old man.
a Chest radiograph shows diffuse opacification of the left upper lung field.
b Ultrasound shows a hypoechoic tumor mass (TU) that has penetrated the pleura (arrow) and invaded the chest wall. LU = lung.
Fig. 15.5 A 62-year-old man with right shoulder pain. a Palpable mass in the right supraclavicular fossa.
b Right-sided meiosis, ptosis, and enophthalmos (Horner syndrome).
c and d Posteroanterior scans of the ribs (C) show a destructive lesion (TU) infiltrating the soft tissues, consistent with a Pancoast tumor.
517