

- •Contents
- •Preface
- •Contributors
- •1 Vessels
- •1.1 Aorta, Vena Cava, and Peripheral Vessels
- •Aorta, Arteries
- •Anomalies and Variant Positions
- •Dilatation
- •Stenosis
- •Wall Thickening
- •Intraluminal Mass
- •Perivascular Mass
- •Vena Cava, Veins
- •Anomalies
- •Dilatation
- •Intraluminal Mass
- •Compression, Infiltration
- •1.2 Portal Vein and Its Tributaries
- •Enlarged Lumen Diameter
- •Portal Hypertension
- •Intraluminal Mass
- •Thrombosis
- •Tumor
- •2 Liver
- •Enlarged Liver
- •Small Liver
- •Homogeneous Hypoechoic Texture
- •Homogeneous Hyperechoic Texture
- •Regionally Inhomogeneous Texture
- •Diffuse Inhomogeneous Texture
- •Anechoic Masses
- •Hypoechoic Masses
- •Isoechoic Masses
- •Hyperechoic Masses
- •Echogenic Masses
- •Irregular Masses
- •Differential Diagnosis of Focal Lesions
- •Diagnostic Methods
- •Suspected Diagnosis
- •3 Biliary Tree and Gallbladder
- •3.1 Biliary Tree
- •Thickening of the Bile Duct Wall
- •Localized and Diffuse
- •Bile Duct Rarefaction
- •Localized and Diffuse
- •Bile Duct Dilatation and Intraductal Pressure
- •Intrahepatic
- •Hilar and Prepancreatic
- •Intrapancreatic
- •Papillary
- •Abnormal Intraluminal Bile Duct Findings
- •Foreign Body
- •The Seven Most Important Questions
- •3.2 Gallbladder
- •Changes in Size
- •Large Gallbladder
- •Small/Missing Gallbladder
- •Wall Changes
- •General Hypoechogenicity
- •General Hyperechogenicity
- •General Tumor
- •Focal Tumor
- •Intraluminal Changes
- •Hyperechoic
- •Hypoechoic
- •Nonvisualized Gallbladder
- •Missing Gallbladder
- •Obscured Gallbladder
- •4 Pancreas
- •Diffuse Pancreatic Change
- •Large Pancreas
- •Small Pancreas
- •Hypoechoic Texture
- •Hyperechoic Texture
- •Focal Changes
- •Anechoic Lesion
- •Hypoechoic Lesion
- •Isoechoic Lesion
- •Hyperechoic Lesion
- •Irregular (Complex Structured) Lesion
- •Dilatation of the Pancreatic Duct
- •Marginal/Mild Dilatation
- •Marked Dilatation
- •5 Spleen
- •Nonfocal Changes of the Spleen
- •Diffuse Parenchymal Changes
- •Large Spleen
- •Small Spleen
- •Focal Changes of the Spleen
- •Anechoic Mass
- •Hypoechoic Mass
- •Hyperechoic Mass
- •Splenic Calcification
- •6 Lymph Nodes
- •Peripheral Lymph Nodes
- •Head/Neck
- •Extremities (Axilla, Groin)
- •Abdominal Lymph Nodes
- •Porta Hepatis
- •Splenic Hilum
- •Mesentery (Celiac, Upper and Lower Mesenteric Station)
- •Stomach
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •Small/Large Intestine
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •8 Peritoneal Cavity
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Wall Structures
- •Smooth Margin
- •Irregular Margin
- •Intragastric Processes
- •Intraintestinal Processes
- •9 Kidneys
- •Anomalies, Malformations
- •Aplasia, Hypoplasia
- •Cystic Malformation
- •Anomalies of Number, Position, or Rotation
- •Fusion Anomaly
- •Anomalies of the Renal Calices
- •Vascular Anomaly
- •Diffuse Changes
- •Large Kidneys
- •Small Kidneys
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Irregular Structure
- •Circumscribed Changes
- •Anechoic Structure
- •Hypoechoic or Isoechoic Structure
- •Complex Structure
- •Hyperechoic Structure
- •10 Adrenal Glands
- •Enlargement
- •Anechoic Structure
- •Hypoechoic Structure
- •Complex Echo Structure
- •Hyperechoic Structure
- •11 Urinary Tract
- •Malformations
- •Duplication Anomalies
- •Dilatations and Stenoses
- •Dilated Renal Pelvis and Ureter
- •Anechoic
- •Hypoechoic
- •Hypoechoic
- •Hyperechoic
- •Large Bladder
- •Small Bladder
- •Altered Bladder Shape
- •Intracavitary Mass
- •Hypoechoic
- •Hyperechoic
- •Echogenic
- •Wall Changes
- •Diffuse Wall Thickening
- •Circumscribed Wall Thickening
- •Concavities and Convexities
- •12.1 The Prostate
- •Enlarged Prostate
- •Regular
- •Irregular
- •Small Prostate
- •Regular
- •Echogenic
- •Circumscribed Lesion
- •Anechoic
- •Hypoechoic
- •Echogenic
- •12.2 Seminal Vesicles
- •Diffuse Change
- •Hypoechoic
- •Circumscribed Change
- •Anechoic
- •Echogenic
- •Irregular
- •12.3 Testis, Epididymis
- •Diffuse Change
- •Enlargement
- •Decreased Size
- •Circumscribed Lesion
- •Anechoic or Hypoechoic
- •Irregular/Echogenic
- •Epididymal Lesion
- •Anechoic
- •Hypoechoic
- •Intrascrotal Mass
- •Anechoic or Hypoechoic
- •Echogenic
- •13 Female Genital Tract
- •Masses
- •Abnormalities of Size or Shape
- •Uterus
- •Abnormalities of Size or Shape
- •Myometrial Changes
- •Intracavitary Changes
- •Endometrial Changes
- •Fallopian Tubes
- •Hypoechoic Mass
- •Anechoic Cystic Mass
- •Solid Echogenic or Nonhomogeneous Mass
- •14 Thyroid Gland
- •Diffuse Changes
- •Enlarged Thyroid Gland
- •Small Thyroid Gland
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Circumscribed Changes
- •Anechoic
- •Hypoechoic
- •Isoechoic
- •Hyperechoic
- •Irregular
- •Differential Diagnosis of Hyperthyroidism
- •Types of Autonomy
- •15 Pleura and Chest Wall
- •Chest Wall
- •Masses
- •Parietal Pleura
- •Nodular Masses
- •Diffuse Pleural Thickening
- •Pleural Effusion
- •Anechoic Effusion
- •Echogenic Effusion
- •Complex Effusion
- •16 Lung
- •Masses
- •Anechoic Masses
- •Hypoechoic Masses
- •Complex Masses
- •Index
4 Pancreas
Pancreas 169
|
|
|
Diffuse Pancreatic Change |
170 |
||||||||||
|
|
|
||||||||||||
|
|
|
|
|
|
Large Pancreas |
170 |
|||||||
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Acute Pancreatitis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Chronic Pancreatitis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Tumor Invasion |
|
|
|
|
|
|
|
Small Pancreas |
172 |
|||||||
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
The Aging Pancreas |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pancreatic Atrophy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Post-pancreatic Necrosis/Pancreatectomy |
|
|
|
|
|
|
|
Hypoechoic Texture |
173 |
|||||||
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Juvenile Pancreas |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
Acute Pancreatitis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Early/Recurrent |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Chronic Pancreatitis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Autoimmune Pancreatitis |
|
|
|
|
|
|
|
|
Hyperechoic Texture |
175 |
||||||
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Fibromatosis/Lipomatosis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
Fibrosis in Hemochromatosis/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
Cystic Fibrosis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Chronic Pancreatitis |
|
|
|
Focal Changes |
179 |
|||||||||||
|
|
|||||||||||||
|
|
|
|
|
|
|
Anechoic Lesion |
179 |
||||||
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Cysts |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
Pseudocysts |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Fluid Collections/Necrosis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
Vessels/Duct System |
|
|
|
|
|
|
|
Hypoechoic Lesion |
182 |
|||||||
|
|
|
|
|
|
|||||||||
Neuroendocrine Tumors
Pancreatic Cancer
Metastasis, Malignant Lymphoma,
Inflammatory Lymph Node
Abscess
Hemorrhagic/Infected
Cyst/Pseudocyst
Focal (Segmental)
Pancreatitis/Ventral Anlage
|
Isoechoic Lesion |
186 |
||
|
||||
|
|
|
Pancreatic Cancer |
|
|
|
|
|
|
|
|
|
Malignant Lymphoma |
|
|
|
|
|
|
|
|
|
Focal Pancreatitis |
|
|
|
|
|
|
|
|
|
Pancreas Divisum |
|
|
|
|
|
|
|
|
|
Annular Pancreas |
|
|
Hyperechoic Lesion |
179 |
||
|
||||
Calcification/Intraductal Calculus
Calcified Splenic Artery
Microcalcification,
Fat Necrosis
Intraductal Gas/Stent
Focal Fatty Infiltration
Irregular (Complex Structured) |
|
Lesion |
191 |
Chronic Pancreatitis
Focal Chronic Pancreatitis
Pseudocyst/Intracystic Hemorrhage
Cystic Neoplasias (Cystadenoma/
Cystadenocarcinoma)
|
Dilatation of the Pancreatic Duct |
195 |
||
|
||||
|
|
|
Marginal/Mild Dilatation |
196 |
|
|
|
||
Postprandial
Bile Duct Disorder
Acute/Recurrent Pancreatitis,
Pancreas Divisum
Chronic Pancreatitis
Periampullary Cancer,
Cancer of the Pancreatic Head
|
|
|
197 |
Marked Dilatation |
|||
Chronic Pancreatitis
Intraductal Mass
Pancreatic Cancer

4Pancreas
G. Schmidt, A. Holle
Anatomy























































Size
●Head: 2.5–3 cm
●Body: < 1.8–2 cm
●Tail: 2.5–3 cm
Shape
●Dumbbell
●Tadpole (pollywog)
The structure of the pancreas shows it to be a composite tubuloalveolar gland. Its size may vary significantly, depending on age and its intrinsic physiological variation in shape; in elderly people the organ becomes smaller and may even atrophy.
Embryonically the pancreas consists of a ventral and a dorsal primordium. Their two ducts, the pancreatic duct (Wirsung’s duct) and the accessory pancreatic duct (duct of Santorini), join together to form a common duct, the main pancreatic duct. The remaining pan-
creatic duct in the pancreatic head drains to the ampulla of Vater. During embryonic development, the accessory pancreatic duct shrinks and drains to the minor papilla. Incomplete fusion leads to pancreas divisum, and a persistent ventral anlage ventrally to the duodenum leads to an annular pancreas.
The variants in shape (dumbbell and tadpole, Fig. 4.1) are characterized by their differences in the size of the pancreatic head and tail. Most confrom to the dimensions given above.
Microstructure. The enzyme-producing terminal segments of the glands are termed acini (“berries”). The interstices house blood vessels, fibroblasts, and strands of collagen, and this interstitial connective tissue becomes denser with age. During embryological development the pancreatic duct becomes the main drainage. Accessory ducts, termed interlobular excretory ductules, branch off it orthogonally. Further branching to the acini within the lo-
bules leads to the so-called intralobular ductules. The lobules of the pancreas are separated from the surrounding tissue not by a firm capsule but by tenuous strands of connective tissue. This explains the blurred outline of the organ in the ultrasound image.
Function. The pancreas is composed of two quite separate types of glandular tissue—the exocrine and the endocrine. The exocrine gland produces a viscous glassy mucus excreted by the acini via excretory ductules into the pancreatic duct. The 0.5–2 million pancreatic islets of Langerhans, diameter 100–200 μm, are cell clusters mainly found in the body and tail of the organ, which constitute the endocrine part of the glandular tissue. They secrete insulin, glucagon, somatostatin, pancreatic polypeptide, and other active peptide hormones and neuropeptides directly into the bloodstream.
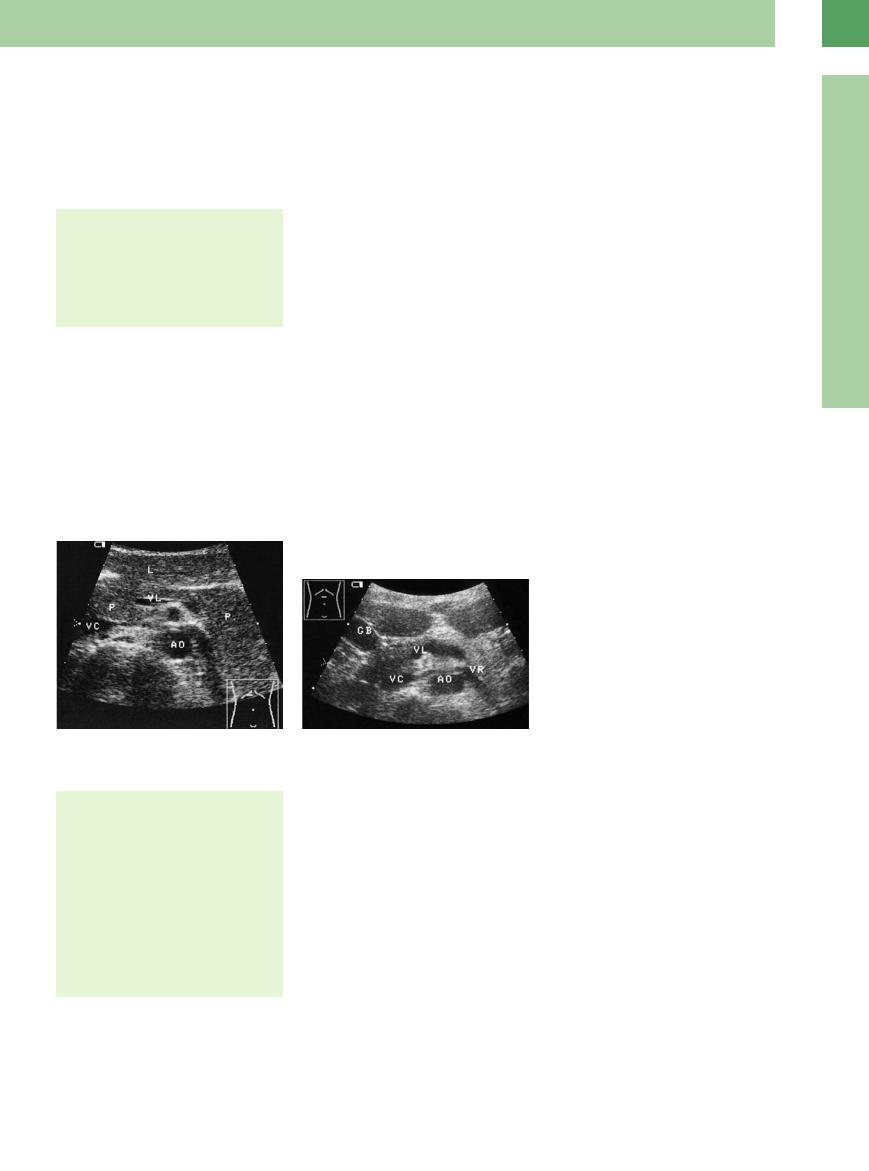
Fig. 4.1 Variant configurations of the pancreas. GB = gallbladder; VR = left renal vein; L = liver; VL = splenic vein; VC = vena cava; AO = aorta.
a Dumbbell: slender body and prominent head as well as tail of the pancreas (P).
b Tadpole: prominent pancreatic head, small body and tail.
4
Pancreas
Topography 





















































Topographic relationships
●Retroperitoneal location anterior to the upper lumbar spine
●Head—anterior to the inferior vena cava
●Body—transverse in the middle of the upper abdomen anterior to the aorta
●Tail—reaches the hilum of the spleen
Ultrasound landmark structures
●Portal vein confluence and its tributaries
●Inferior vena cava
●Vessels of the celiac axis
The pancreas lies transversely and somewhat obliquely in the retroperitoneum, directly anterior to the spine at the level of the second lumbar vertebra. The head of the pancreas nes-
tles in the posterocaudad concavity of the duodenum; the pancreatic body traverses the spine and courses along the anterior margin of the left kidney, while the tail reaches cephalad into the hilum of the spleen (Figs. 4.2, 4.3, 4.4).
Borders. The posterior borders are defined by the spine and the lumbar part of the diaphragm, abdominal aorta, and inferior vena cava, all anterior to the spine. Most of the anterior aspect of the pancreas is covered by the stomach. The omental bursa is formed by the posterior wall of the stomach (up to the lesser curvature) and the anterior aspect of the pancreas. From the border between the head and body of the pancreas to the left, there is the cavity of the omental bursa or lesser sac, which in acute pancreatitis may fill up with exudate.
Posterior to the head of the pancreas, the distal segment of the common bile duct (CBD) and the prepapillary section of the pancreatic duct course together for part of the way to the papilla of Vater, in 75% of cases within a common trough, in the other 25% intrapancreatically.
Blood supply. The origins of the celiac axis and the superior mesenteric artery lie cephalad to the pancreas. Since the celiac axis runs in an anterosuperior direction and the superior mesenteric artery posteroinferior to the pancreas, the organ is caught in a kind of vise. If these vessels are infiltrated in pancreatic cancer, the tumor is no longer amenable to resection. The superior mesenteric artery and vein run in the pancreatic incision across the uncinate process, the latter resting posterior to these vessels.
169