

- •Contents
- •Preface
- •Contributors
- •1 Vessels
- •1.1 Aorta, Vena Cava, and Peripheral Vessels
- •Aorta, Arteries
- •Anomalies and Variant Positions
- •Dilatation
- •Stenosis
- •Wall Thickening
- •Intraluminal Mass
- •Perivascular Mass
- •Vena Cava, Veins
- •Anomalies
- •Dilatation
- •Intraluminal Mass
- •Compression, Infiltration
- •1.2 Portal Vein and Its Tributaries
- •Enlarged Lumen Diameter
- •Portal Hypertension
- •Intraluminal Mass
- •Thrombosis
- •Tumor
- •2 Liver
- •Enlarged Liver
- •Small Liver
- •Homogeneous Hypoechoic Texture
- •Homogeneous Hyperechoic Texture
- •Regionally Inhomogeneous Texture
- •Diffuse Inhomogeneous Texture
- •Anechoic Masses
- •Hypoechoic Masses
- •Isoechoic Masses
- •Hyperechoic Masses
- •Echogenic Masses
- •Irregular Masses
- •Differential Diagnosis of Focal Lesions
- •Diagnostic Methods
- •Suspected Diagnosis
- •3 Biliary Tree and Gallbladder
- •3.1 Biliary Tree
- •Thickening of the Bile Duct Wall
- •Localized and Diffuse
- •Bile Duct Rarefaction
- •Localized and Diffuse
- •Bile Duct Dilatation and Intraductal Pressure
- •Intrahepatic
- •Hilar and Prepancreatic
- •Intrapancreatic
- •Papillary
- •Abnormal Intraluminal Bile Duct Findings
- •Foreign Body
- •The Seven Most Important Questions
- •3.2 Gallbladder
- •Changes in Size
- •Large Gallbladder
- •Small/Missing Gallbladder
- •Wall Changes
- •General Hypoechogenicity
- •General Hyperechogenicity
- •General Tumor
- •Focal Tumor
- •Intraluminal Changes
- •Hyperechoic
- •Hypoechoic
- •Nonvisualized Gallbladder
- •Missing Gallbladder
- •Obscured Gallbladder
- •4 Pancreas
- •Diffuse Pancreatic Change
- •Large Pancreas
- •Small Pancreas
- •Hypoechoic Texture
- •Hyperechoic Texture
- •Focal Changes
- •Anechoic Lesion
- •Hypoechoic Lesion
- •Isoechoic Lesion
- •Hyperechoic Lesion
- •Irregular (Complex Structured) Lesion
- •Dilatation of the Pancreatic Duct
- •Marginal/Mild Dilatation
- •Marked Dilatation
- •5 Spleen
- •Nonfocal Changes of the Spleen
- •Diffuse Parenchymal Changes
- •Large Spleen
- •Small Spleen
- •Focal Changes of the Spleen
- •Anechoic Mass
- •Hypoechoic Mass
- •Hyperechoic Mass
- •Splenic Calcification
- •6 Lymph Nodes
- •Peripheral Lymph Nodes
- •Head/Neck
- •Extremities (Axilla, Groin)
- •Abdominal Lymph Nodes
- •Porta Hepatis
- •Splenic Hilum
- •Mesentery (Celiac, Upper and Lower Mesenteric Station)
- •Stomach
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •Small/Large Intestine
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •8 Peritoneal Cavity
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Wall Structures
- •Smooth Margin
- •Irregular Margin
- •Intragastric Processes
- •Intraintestinal Processes
- •9 Kidneys
- •Anomalies, Malformations
- •Aplasia, Hypoplasia
- •Cystic Malformation
- •Anomalies of Number, Position, or Rotation
- •Fusion Anomaly
- •Anomalies of the Renal Calices
- •Vascular Anomaly
- •Diffuse Changes
- •Large Kidneys
- •Small Kidneys
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Irregular Structure
- •Circumscribed Changes
- •Anechoic Structure
- •Hypoechoic or Isoechoic Structure
- •Complex Structure
- •Hyperechoic Structure
- •10 Adrenal Glands
- •Enlargement
- •Anechoic Structure
- •Hypoechoic Structure
- •Complex Echo Structure
- •Hyperechoic Structure
- •11 Urinary Tract
- •Malformations
- •Duplication Anomalies
- •Dilatations and Stenoses
- •Dilated Renal Pelvis and Ureter
- •Anechoic
- •Hypoechoic
- •Hypoechoic
- •Hyperechoic
- •Large Bladder
- •Small Bladder
- •Altered Bladder Shape
- •Intracavitary Mass
- •Hypoechoic
- •Hyperechoic
- •Echogenic
- •Wall Changes
- •Diffuse Wall Thickening
- •Circumscribed Wall Thickening
- •Concavities and Convexities
- •12.1 The Prostate
- •Enlarged Prostate
- •Regular
- •Irregular
- •Small Prostate
- •Regular
- •Echogenic
- •Circumscribed Lesion
- •Anechoic
- •Hypoechoic
- •Echogenic
- •12.2 Seminal Vesicles
- •Diffuse Change
- •Hypoechoic
- •Circumscribed Change
- •Anechoic
- •Echogenic
- •Irregular
- •12.3 Testis, Epididymis
- •Diffuse Change
- •Enlargement
- •Decreased Size
- •Circumscribed Lesion
- •Anechoic or Hypoechoic
- •Irregular/Echogenic
- •Epididymal Lesion
- •Anechoic
- •Hypoechoic
- •Intrascrotal Mass
- •Anechoic or Hypoechoic
- •Echogenic
- •13 Female Genital Tract
- •Masses
- •Abnormalities of Size or Shape
- •Uterus
- •Abnormalities of Size or Shape
- •Myometrial Changes
- •Intracavitary Changes
- •Endometrial Changes
- •Fallopian Tubes
- •Hypoechoic Mass
- •Anechoic Cystic Mass
- •Solid Echogenic or Nonhomogeneous Mass
- •14 Thyroid Gland
- •Diffuse Changes
- •Enlarged Thyroid Gland
- •Small Thyroid Gland
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Circumscribed Changes
- •Anechoic
- •Hypoechoic
- •Isoechoic
- •Hyperechoic
- •Irregular
- •Differential Diagnosis of Hyperthyroidism
- •Types of Autonomy
- •15 Pleura and Chest Wall
- •Chest Wall
- •Masses
- •Parietal Pleura
- •Nodular Masses
- •Diffuse Pleural Thickening
- •Pleural Effusion
- •Anechoic Effusion
- •Echogenic Effusion
- •Complex Effusion
- •16 Lung
- •Masses
- •Anechoic Masses
- •Hypoechoic Masses
- •Complex Masses
- •Index

10 Adrenal Glands
Adrenal Glands |
367 |
||||||
|
Enlargement |
369 |
|||||
|
|||||||
|
|
|
|
Anechoic Structure |
369 |
||
|
|
|
|
||||
|
|
|
|
|
|
Adrenal Cyst |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Intra-adrenal Hemorrhage |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Adrenal Abscess |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cystic Tumor |
|
|
|
|
Hypoechoic Structure |
370 |
|||
|
|
|
|||||
|
|
|
|
|
|
Hyperplasia |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Adenoma |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Metastasis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Lymphoma |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Adrenal Carcinoma |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Incidentaloma |
|
|
|
|
Complex Echo Structure |
374 |
|||
|
|
|
|||||
|
|
|
|
|
|
Metastasis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pheochromocytoma |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Carcinoma |
|
|
|
|
Hyperechoic Structure |
375 |
|||
|
|
|
|
|
|
Lipoma, Myelolipoma |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Calcification |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Metastasis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pheochromocytoma |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Neuroblastoma |
|

10Adrenal Glands
D. Nuernberg
Anatomy























































Shape
●Right: linear or V-shaped
●Left: V- or Y-shaped
Size
●Wings are 2–3 cm long and 6–8 mm thick
The adrenal glands are small, cap-like glandular organs situated in close proximity to the kidneys. Often these “suprarenal” glands are incorrectly looked for above the kidneys, but the term “adrenal” correctly implies that each gland is predominantly medial to the upper pole of the associated kidney. The right adrenal gland has a linear or V shape, while the left
adrenal gland is more V- or Y-shaped. The wings of each gland are 2–3 cm long and 6–8 mm thick. Their function is hormone production. The adrenal cortex secretes cortisol, aldosterone, and sex hormones, while the adrenal medulla secretes epinephrine and norepinephrine.
Ultrasound Topography
Topography















































Landmarks
●Right side: kidney and inferior vena cava
●Left side: aorta, lower pole of spleen, upper pole of kidney
Visualization
●Right side: subcostal flank scan or oblique scan
●Left side: intercostal flank scan through the spleen
Fig. 10.1 Cross-sectional diagram at the level of the adrenal glands. The adrenal glands are the Y-shaped structures lying anteromedial to the kidneys. Pa = pancreas; rK = right kidney; lK = left kidney; A = aorta; V = inferior vena cava; SC = spinal column.
The adrenal glands are located within the retroperitoneum. The right adrenal gland lies superomedial to the right kidney and posterolateral to the inferior vena cava. These are the principal landmarks on the right side. Typically the right adrenal gland is visualized behind the right lobe of the liver and anterior to the inferior (lumbar) crus of the diaphragm. The most favorable planes for ultrasound scanning are a right subcostal flank scan or oblique subcostal scan.
The left adrenal gland is inherently more difficult to scan than the right because it lacks the acoustic window of the liver and is ob-
Fig. 10.2 Diagram of the adrenal glands showing their relations to neighboring organs.
scured by air in the stomach. It is imaged with an intercostal flank scan directed through the spleen. The key landmarks are the aorta medially and the lower pole of the spleen or upper renal pole laterally.1–3
Not infrequently, the adrenal glands extend down to the level of the renal hilum. Besides the kidneys, they are bordered by the liver and inferior vena cava on the right side and by the aorta and tail of the pancreas on the left side (Fig.10.1, Fig.10.2). The adrenal region on each side appears as a triangular echogenic area bordered by the landmarks noted above
(Fig.10.3, Fig.10.4).
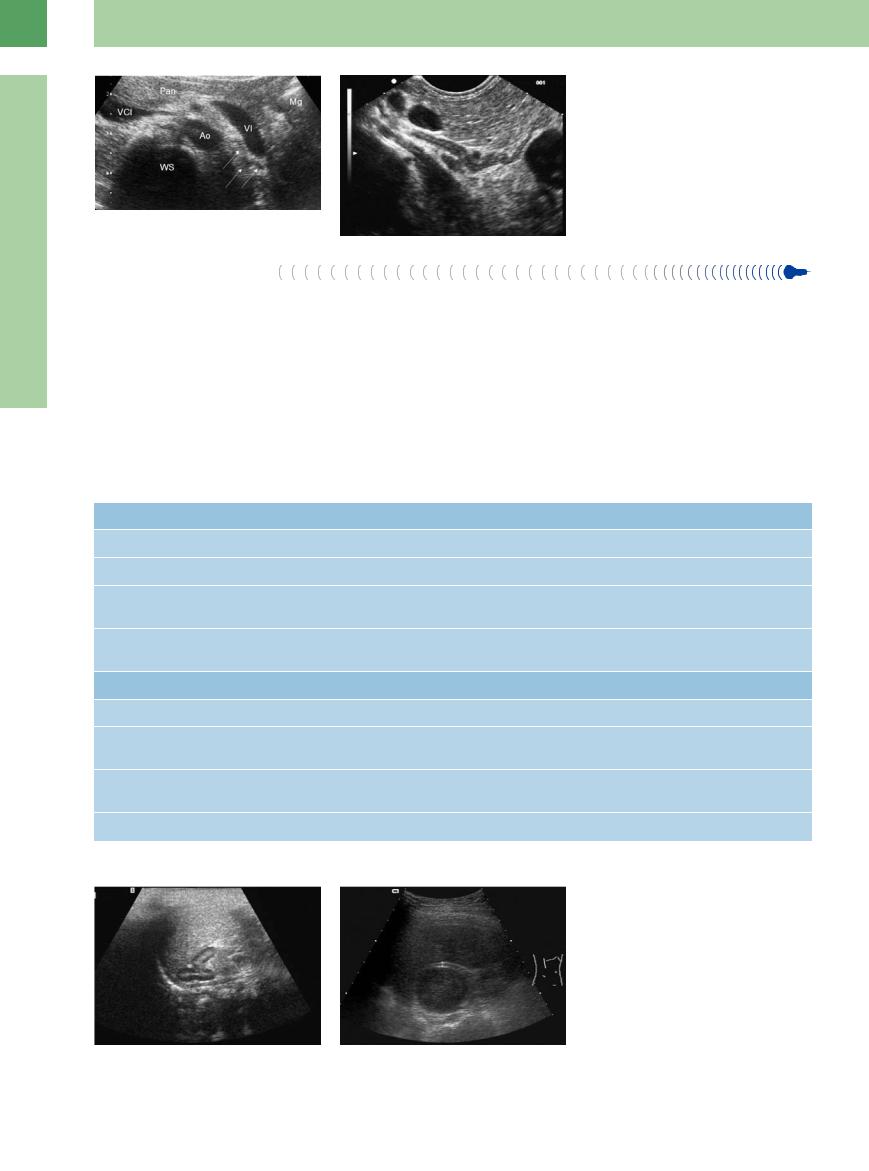
Fig. 10.3 The normal adrenal gland is visible behind the right liver lobe, lateral to the vena cava, in front of the crura of the diaphragm and medial of the right kidney. Lower crura seen as hypoechoic belt with a hint of their multilayered nature (arrow).
10
Adrenal Glands
367
10
Adrenal Glands
ditions, a high-resolution transducer, and a meticulous examination by a knowledgeable sonographer are required. It is more accurate, then, to speak of evaluating the “adrenal region” rather than the glands themselves. CT can consistently define the normal-size adrenal glands, giving this study a priority role in the primary imaging of these structures.
row, oblong shape with a hypoechoic cortex and medulla. The adrenal glands can almost always be visualized in newborns. The physiological hypertrophy at this stage of life results in relatively large glands that are easily identified on ultrasound and show clear corticomedullary differentiation (Fig.10.5a).
In adults, however, the adrenal glands are usually visualized only when they are en-
Fig. 10.4
a In transverse section the left adrenal gland is posterior to the splenic vein and lateral to the aorta. The gland itself is often not visualized (image courtesy of Dr. Christian Jenssen, Strausberg, Germany).
b Best visibility of the left adrenal gland is achieved by endosonography. Both lobes are marked very finely and multilayered. In the center the normal adrenal gland can reach a thickness of 9–10 mm.
nal glands may or may not be associated with endocrine symptoms (Table 10.1). Examination of the adrenal region is indicated for the staging of oncological disease and in endocrinological investigations. Adrenal abnormalities are often detected incidentally, however. In the absence of an underlying disease, an incidentally detected solid adrenal mass is called an incidentaloma (Fig.10.5b).
Table 10.1 Sonographic features of adrenal diseases with or without endocrine symptoms13
Diseases with endocrine symptoms |
Sonographic appearance |
Addison disease |
Adrenal atrophy not detectable with ultrasound; possible calcifications as evidence of prior tuberculosis |
Conn disease |
Unilateral adenomas, usually < 2 cm, not detectable with ultrasound |
Cushing syndrome |
In 80% of cases, bilateral hyperplasia due to pituitary (75%) or paraneoplastic (5%) ACTH overproduction; |
|
hyperplasia is usually not detectable with ultrasound |
Pheochromocytoma |
Can be localized with ultrasound in 80–90% of cases; extra-adrenal location is di cult, usually prevents |
|
identification |
Diseases without endocrine symptoms |
|
Adrenal adenoma |
Most common solid mass |
Adrenal carcinoma |
Often quite large (several centimeters) despite absence of symptoms; sometimes detected incidentally |
|
at ultrasound |
Adrenal metastases |
Common with bronchial carcinoma, malignant lymphoma, breast cancer, renal cancer, pancreatic cancer, |
|
and melanoma |
Adrenal tumors and cysts |
Detectable at 1–1.5 cm on the right side, at 1.5–2 cm on the left side |
|
Fig. 10.5 |
|
a Normal adrenal gland of an infant, consisting of a |
|
hyperechoic medulla and hypoechoic cortex. |
|
b Medial to the upper pole of the right kidney is a sharply |
|
circumscribed, hypoechoic mass: typical adrenal inciden- |
|
taloma. |
368