

2 Liver
Liver 57
|
|
|
|
Diffuse Changes in |
70 |
||||||||||
|
|
Hepatic Parenchyma |
|||||||||||||
|
|
|
|
|
|
|
Enlarged Liver |
70 |
|||||||
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Congested Liver |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fatty Liver |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fatty Liver Hepatitis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fatty Cirrhosis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Diffuse Infiltration |
|
|
|
|
|
|
|
|
Small Liver |
76 |
|||||||
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Atrophy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cirrhosis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Resection |
|
|
|
|
|
|
|
Homogeneous Hypoechoic |
77 |
||||||||
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
Texture |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Acute Liver Congestion |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Amyloidosis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Acute Hepatitis |
|
|
|
|
|
|
|
Homogeneous Hyperechoic |
79 |
||||||||
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
Texture |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fatty Liver |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hemochromatosis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fibrosis |
|
|
|
|
|
|
|
Regionally Inhomogeneous |
80 |
||||||||
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
Texture |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Focal Fatty Infiltration |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Necrosis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Portal Venous Gas Embolism |
|
|
|
|
|
|
|
Diffuse Inhomogeneous Texture |
82 |
||||||||
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Chronic Hepatitis |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cirrhosis |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Disseminated Tumor Growth |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Diffuse Tumor Growth |
|
|
|
|
Localized Changes in |
86 |
|||||||||||
|
|
||||||||||||||
|
|
Hepatic Parenchyma |
|||||||||||||
|
|
|
|
|
|
Anechoic Masses |
88 |
||||||||
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cysts |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Polycystic Liver Disease |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hemorrhage/Hematoma |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Bilioma |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Abscess |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hydatid Cysts |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hereditary Hemorrhagic |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Telangiectasia/Hepatic Peliosis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Lipoma |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Lymphoma |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Metastases |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Vessels/Bile Ducts |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
96 |
|
|
|
|
|
|
|
Hypoechoic Masses |
|||||||||
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Metastasis |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Lymphoma |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Abscess |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hematoma |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Complicated Cyst |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Adenoma |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Focal Nodular Hyperplasia |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hepatocellular Carcinoma |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Lipoma |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Atypical Hemangioma |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Focal Fatty Change |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Bile Ducts/Vessels |
|
|
|
|
|
|
|
Isoechoic Masses |
101 |
||||||||
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Focal Nodular Hyperplasia |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Adenoma |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hepatocellular Carcinoma |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Metastasis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Atypical Hemangioma |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hematoma |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
“Hepatized” Gallbladder |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Bile Ducts/Vessels |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
 Localized Changes in
Localized Changes in
Hepatic Parenchyma (Continued)
|
|
|
Hyperechoic Masses |
107 |
||||
|
|
|
|
|
|
|
Hemangioma |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
Bile Duct Hamartomas |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
Porphyria |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
Regenerative Nodules |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hepatocellular Carcinoma |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Focal Nodular Hyperplasia |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Metastasis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Abscess |
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Necrosis |
|
|
|
|
|
|
|
|
Diaphragmatic Slips |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
Round Ligament of the Liver |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
Focal Fatty Change |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
Bile Ducts/Vessels |
|
|
|
Echogenic Masses |
114 |
|||||
|
|
|
|
|
|
|
“Comet Tails” |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Calcification |
|
|
|
|
|
|
|
|
Calculus |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Foreign Body |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Air |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
Irregular Masses |
117 |
|||||
|
|
|
|
|
|
|
Hepatocellular Carcinoma |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Thorotrastosis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Diffuse Metastasis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Alveolar Hydatid Disease |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Liver Injuries in Multiple Trauma |
|
|
Differential Diagnosis of Focal Lesions |
119 |
||||||
|
||||||||
|
|
Diagnostic Methods |
119 |
|||||
|
|
|
|
|
|
|
Ultrasonography |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MRI |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PET |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Scintigraphy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Laparoscopy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Needle Biopsy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Angiography |
|
|
|
|
|
|
||||
|
|
Suspected Diagnosis |
121 |
|||||
|
|
|
|
|
|
|
Hemangioma |
|
|
|
|
|
|
|
|
Focal Nodular Hyperplasia |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hepatocellular Carcinoma |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Metastasis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2Liver
M.W.M. Brandt
The liver is the largest gland as well as the largest single organ in the human body, weighing 1500–1800 g (accounting for about 2.3–3% of body weight). Blood, primarily from the splanchnic region, flows through the liver, where numerous substances are recovered and metabolized. Apart from breaking down and synthesizing substances, the liver is a key element in storage pathways (glycogen, fat). It either releases these metabolites directly into the bloodstream or excretes them via the bile (1500 mL/day). In addition, the liver is characterized by its organ-specific macrophages (Kupffer cells), which are an integral part of the human macrophage system (reticuloendothelial system, RES). In summary, this organ plays a vital role not only in metabolic detoxification but also in the synthesis de novo and storage of proteins, sugar molecules, and fat as well as in the secretion of digestive juices.
In order to carry out these varied functions, the anatomy of the liver is based on the socalled hepatic lobules with their functional unit, the hepatic acinus, according to Rappaport (Fig. 2.1). Splanchnic blood flowing through a branch of the portal vein passes through three successive metabolic zones where the substances transported by the blood are metabolized. All products synthesized by the liver are passed into the bloodstream through the central vein or excreted via a countercurrent mechanism into the bile ducts that parallel the terminal portal branches (Fig. 2.2).
Fig. 2.1 Hepatic lobule and acinus according to Kiernan and Rappaport. The gray hepatic lobule of Kiernan is characterized by its central vein and the peripheral portal areas; the colored hepatic acinus of Rappaport has a terminal branch of the portal vein in its center while the central veins (of the hepatic lobule) are on its periphery, and in between there are three distinct metabolic zones: zone 1 is rich and zone 3 poor in nutrients.
Fig. 2.2 Schematic diagram of a hepatic sinusoid together with a portal triad. In the sinusoids, blood from the terminal branch of the portal vein (joined in the portal triad by the artery and the bile duct) flows through the three successive metabolic zones into the central vein. Excretion into the bile ducts paralleling the branches of the portal vein is by countercurrent principle.
Topography 





















































The liver is located in the right hypochondrium, protected by the ribs (Fig. 2.3). Its general shape is that of a pyramid, with the base pointing to the right side of the body. The average transverse diameter is 25–30 cm, the cephalocaudal length is 12–20 cm, and the normal anteroposterior diameter is 6–10 cm. The superior aspect (diaphragmatic surface) borders the diaphragm and is composed of a fixed and a mobile part; parts of the anterior aspect are in contact with the abdominal wall. The inferior surface of the liver points in a posterocaudal direction; on the left and in the middle the inferior aspect is in contact with the gastric wall, while on the lateral right side it borders the hepatic flexure of the colon. The gallbladder is attached to the inferior surface of the liver in the midclavicular line. The right dorsal aspect of the liver is anterior to the upper pole of the right kidney. The porta hepatis is situated in the middle of the inferior surface, anterior to the caudate lobe (see below) and the dorsal vena cava (Fig. 2.4); the porta hepatis contains the hepatic artery proper and its two branches, the left and right hepatic artery, the extrahepatic bile duct, lymphatic vessels, and nerves.
Fig. 2.3 Topography. Location of the liver in the right hypochondrium, protected by the lower right ribs; note the relationship with the diaphragm, right kidney, major retroperitoneal vessels, colon, and stomach.
Fig. 2.4 Schematic anatomy of the porta hepatis. Aorta and vena cava are posterior; the portal vein is on the right, coursing obliquely and anteriorly to the vena cava. The portal vein is posterior to the hepatic artery and medial to the extrahepatic bile duct.
2
Liver
57
2
Liver
Table 2.1 Hepatic segments |
|
|
|
|
Segment |
Location |
Topography, boundary |
Name |
Tributary |
I |
Left medial, posterior, |
Anterior to vena cava, posterior to segment IVa |
Caudate lobe |
Left portal vein branch |
|
anterior to vena cava |
|
|
|
II |
Left lateral, superior, |
Superior to segment I , medial to segment IVa, |
Superior part is anatomic |
Left portal vein branch |
|
subcardial |
forms superior left medial margin |
left lobe |
|
III |
Left lateral, inferior |
Inferior to segment II, medial to segment IVb, |
Inferior part is anatomic |
Left portal vein branch III |
|
|
forms inferior left medial margin |
left lobe |
|
IV |
Left medial, anterior |
Right lateral to round ligament and lateral to |
Quadrate lobe |
Left portal vein branch IV |
|
|
segment II/III, medial to segment V |
|
|
V |
Right medial, inferior |
Medial to segment VI/VII, superior to |
Forms gallbladder fossa |
Right portal vein branch |
|
|
gallbladder |
|
|
VI |
Right lateral, inferior |
Inferior to segment VII, lateral to segment V, |
|
Right portal vein branch |
|
|
forms right lateral margin |
|
|
VII |
Right lateral, superior, |
Superior to segment VI, lateral to segment VIII, |
|
Right portal vein branch |
|
subphrenic |
subphrenic, forms right lateral superior margin |
|
|
VIII |
Right medial superior, |
Superior to segment V, medial to segment VII, |
|
Right portal vein branch |
|
subphrenic |
subphrenic |
|
|
Anatomy























































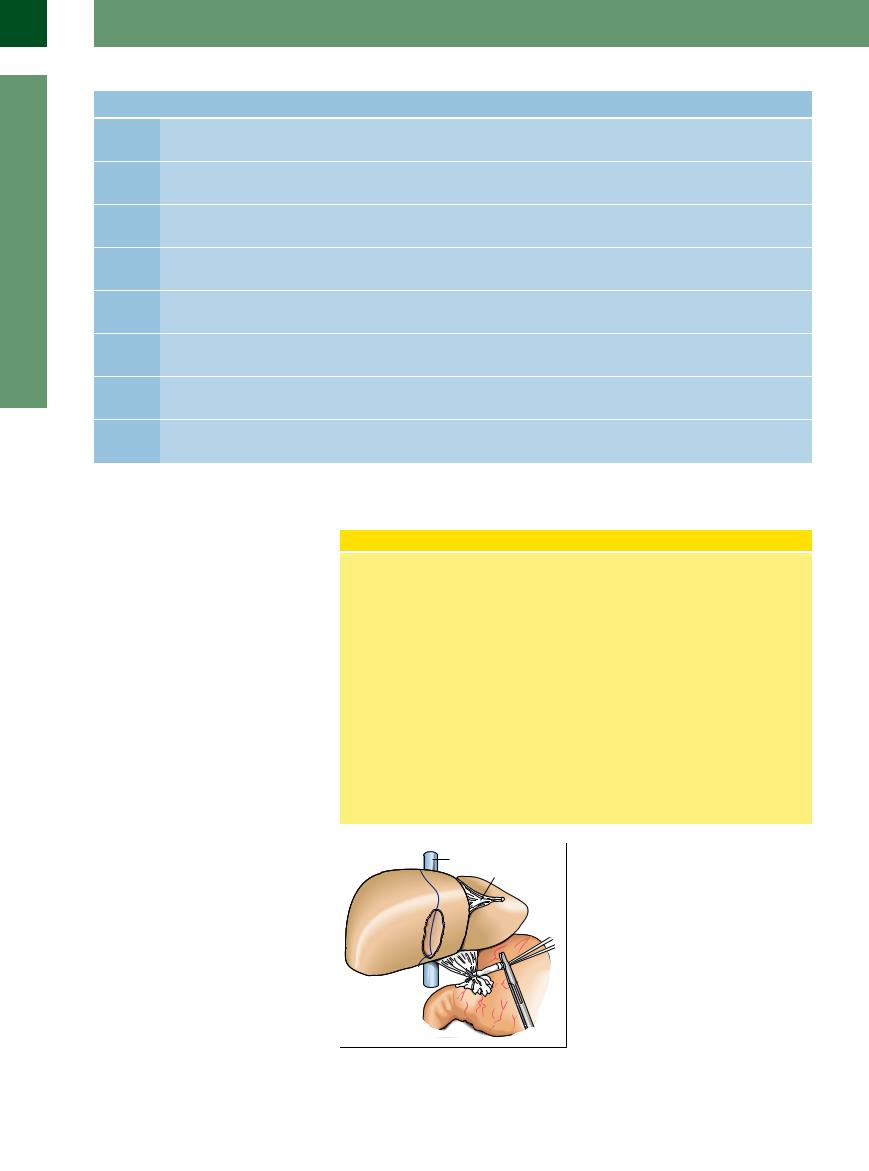
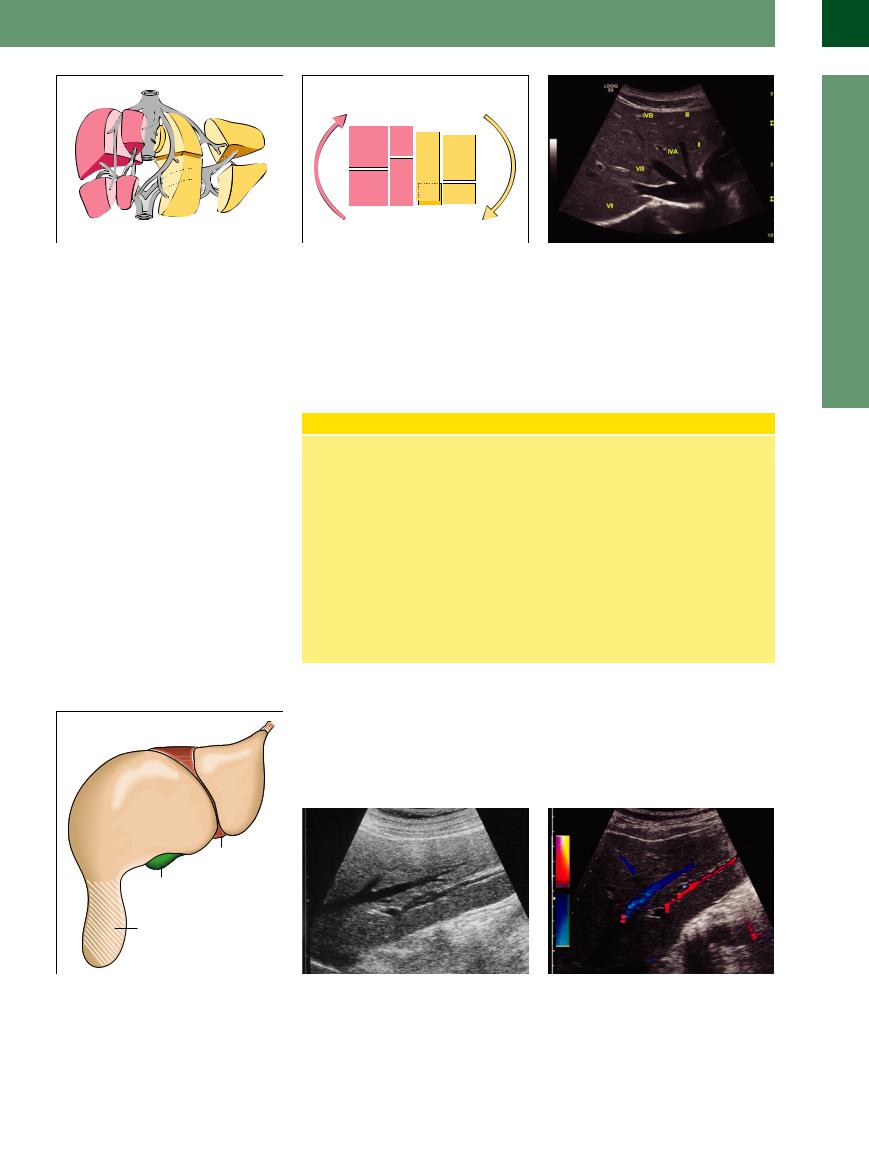
From a macroscopic anatomical point of view, the liver is subdivided into a larger right lobe (representing the base of the pyramid) and a smaller left hepatic lobe (the apex of the pyramid), with the falciform ligament (containing the round ligament or ligamentum teres) dividing the two lobes (Fig. 2.5). In terms of its microanatomy, the liver is made up of eight functionally separate segments that follow the vascular tree (Fig. 2.6; Table 2.1). If circumscribed masses or pathological findings can be correlated to a specific segment, this is extremely helpful in preoperative and intraoperative diagnosis as well as for possible resectability or any planned interventional angiographic procedures. However, since anatomical variants are numerous and not particularly infrequent, segmental correlation is not always certain and thus may be of only limited value in some cases.
Couinaud Segmental Anatomy of the Liver
The microanatomy of the liver consists of eight functionally different segments. When viewed from the front/below they are counted clockwise: the left hepatic lobe made up of segments I–IV and the right lobe of segments V–VIII. Compared to the anatomical division of the liver along the falciform ligament (including the ligamentum teres) into a smaller left lobe (only segments II and III) and a larger right lobe (segments V–VIII plus segments I and IVa/ b), Couinaud segmental anatomy follows the vascular tree (Fig. 2.6, Fig. 2.7). Here the ramifications and branches of the portal vein (accompanied by the branches of the hepatic artery and the bile ducts = portal triad) are the central structures of each segment, while the hepatic veins run-
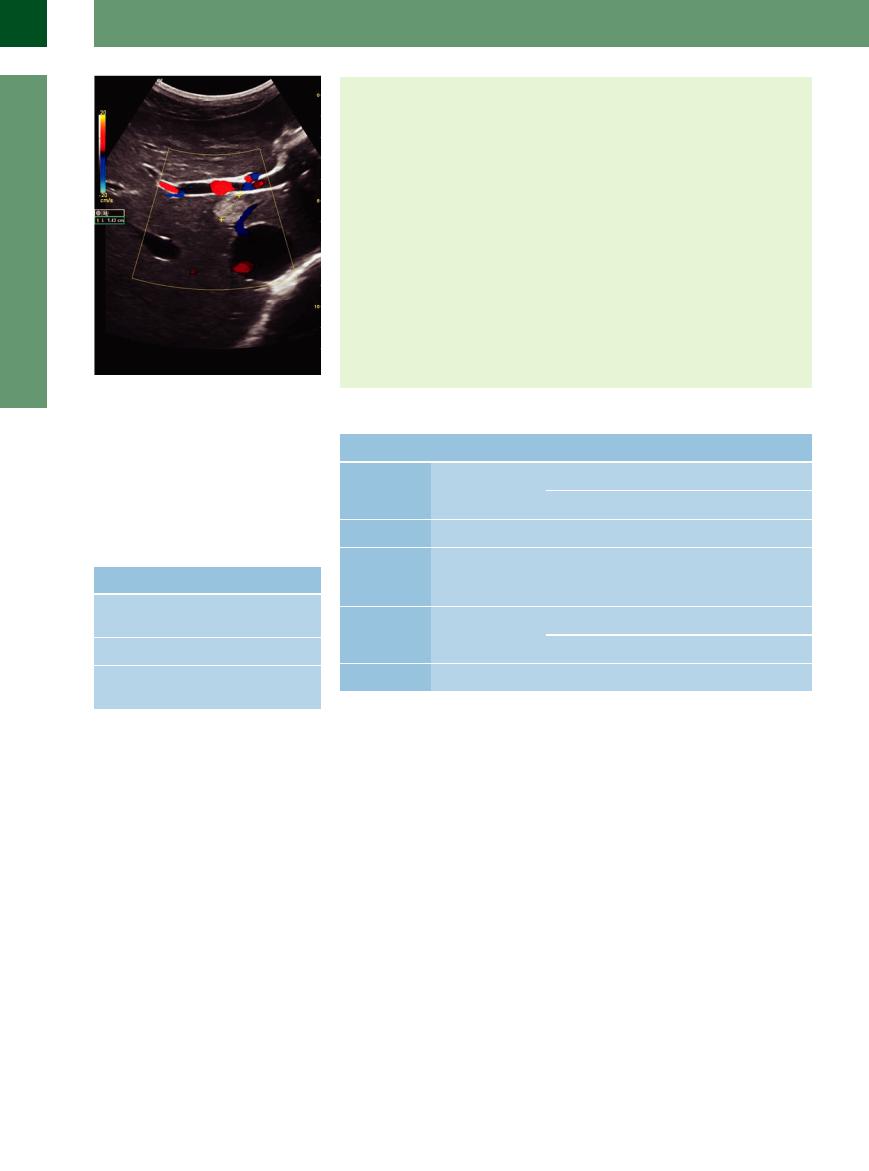
ning between the segments drain the blood (Fig. 2.8). There are three major hepatic veins—right (lateral right), middle, and left (medial)—all joining the vena cava posteriorly at the bare area of the superior aspect of the liver below the diaphragm. The middle hepatic vein divides the angiographic right hepatic lobe from the left lobe. The left hepatic vein drains between double segments II/III as well as IVa/IVb of the left lobe. The right hepatic vein drains between double segments VI/VII and V/ VIII. Segment I is the caudate lobe and is part of the left hepatic lobe draining the blood directly in to the vena cava. Segment IV corresponds to the quadrate lobe, while segment V forms the base of the gallbladder fossa.
Fig. 2.5 Liver anatomy. Inferior view: the round ligament (falciform) separates the anatomical left hepatic lobe (LL) from the lateral anatomical right lobe, which is larger and is shown with the gallbladder fossa on its inferior aspect. The vena cava can be seen posteriorly. The dotted line marks the imaginary plane running through the gallbladder fossa and vena cava, which is considered the dividing line between the vascular tree of the left and right branches of the portal vein.
58
 Morphology
Morphology














































 2.1; Table 2.3).
2.1; Table 2.3). 


 2.1 Extrinsic Criteria
2.1 Extrinsic Criteria


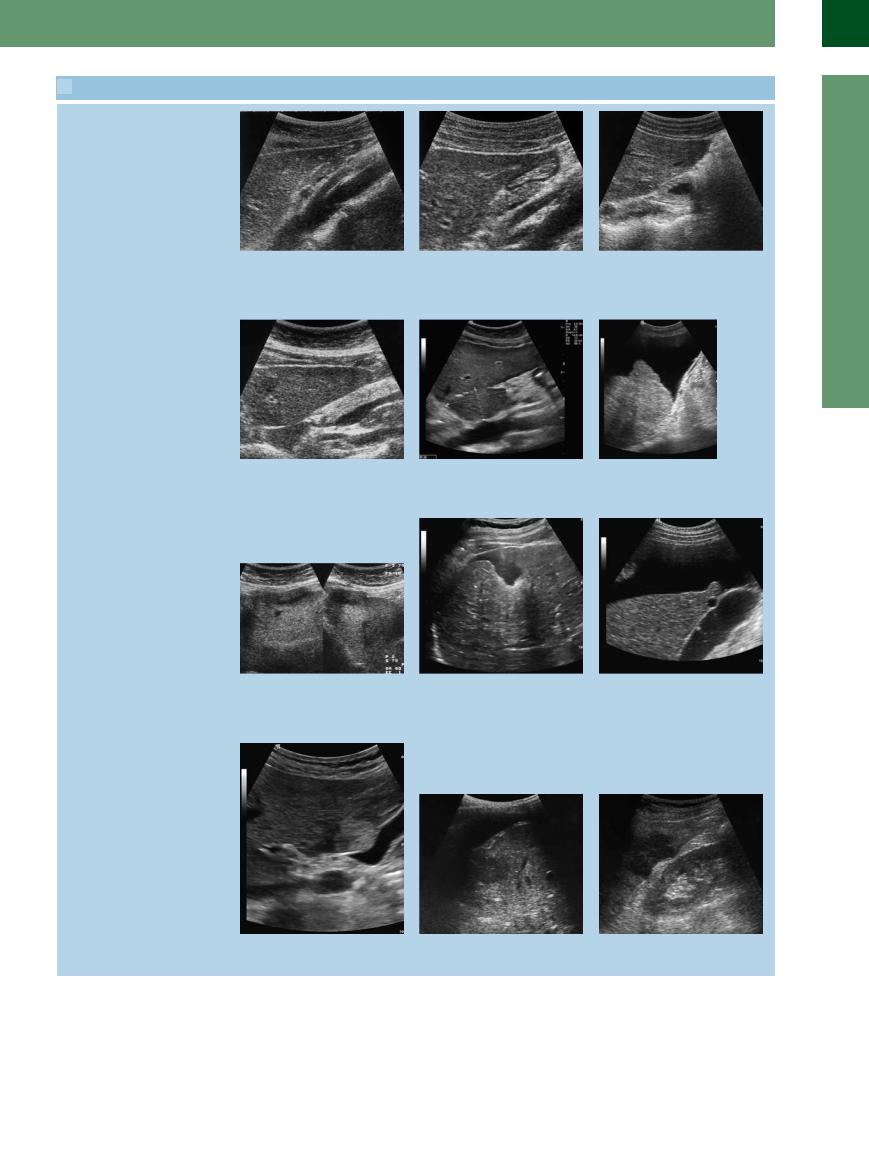
 2.2 Assessing the Hepatic Parenchyma
2.2 Assessing the Hepatic Parenchyma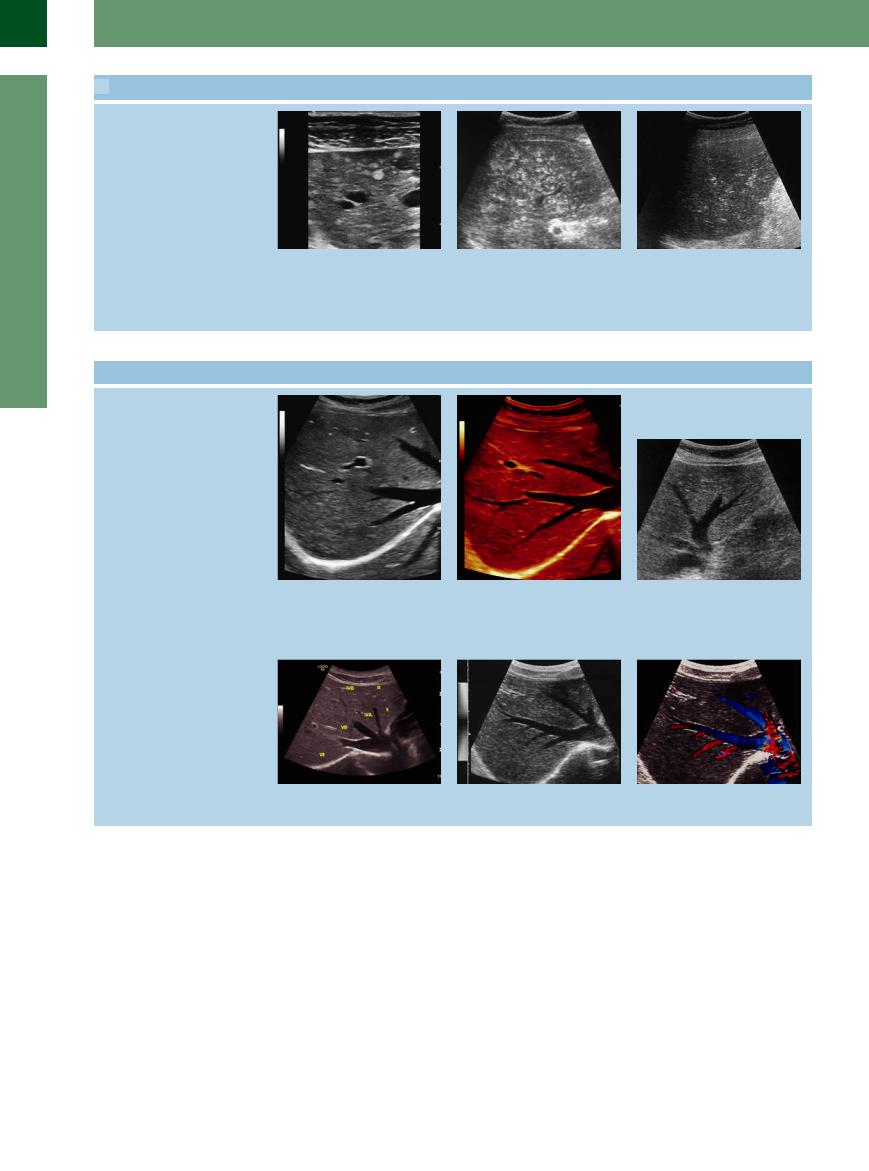
 2.2 Assessing the Hepatic Parenchyma (Continued)
2.2 Assessing the Hepatic Parenchyma (Continued) 2.3 Hepatic Veins
2.3 Hepatic Veins 2.3 Hepatic Veins (Continued)
2.3 Hepatic Veins (Continued)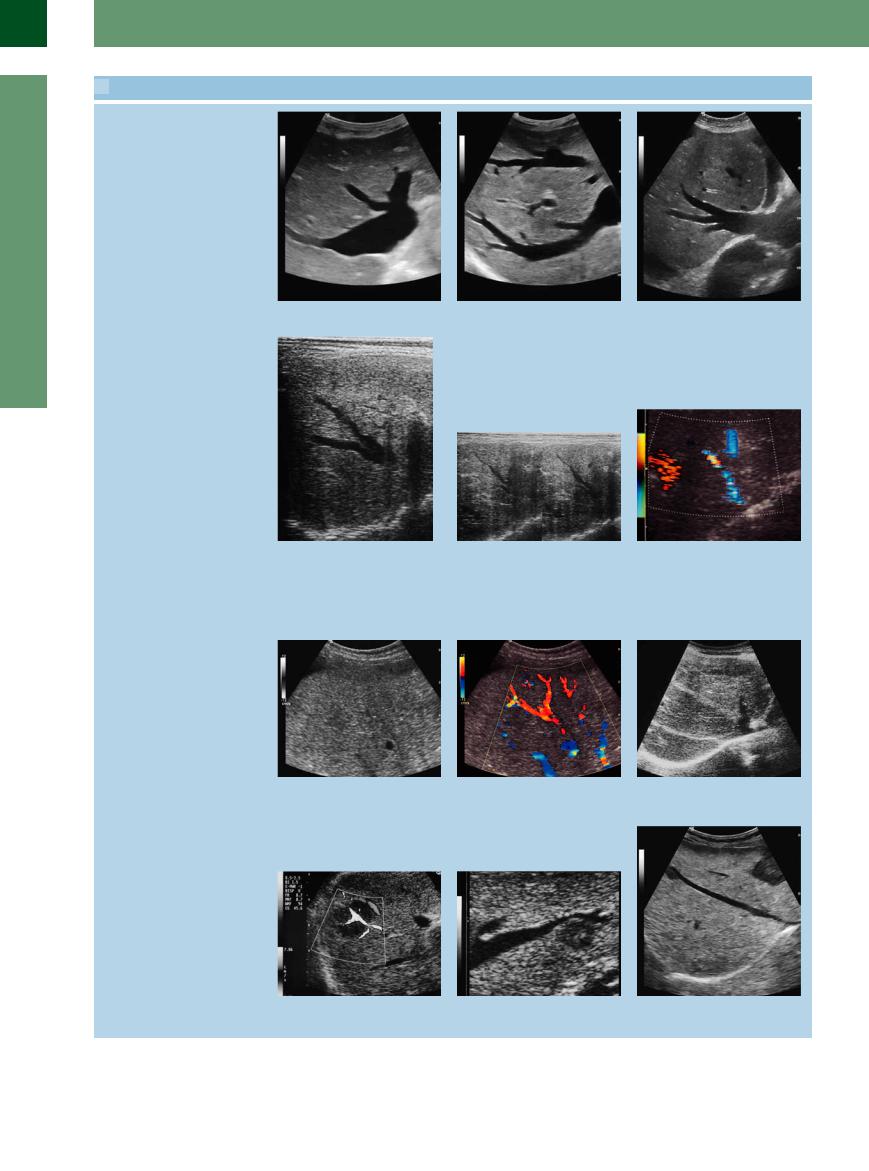
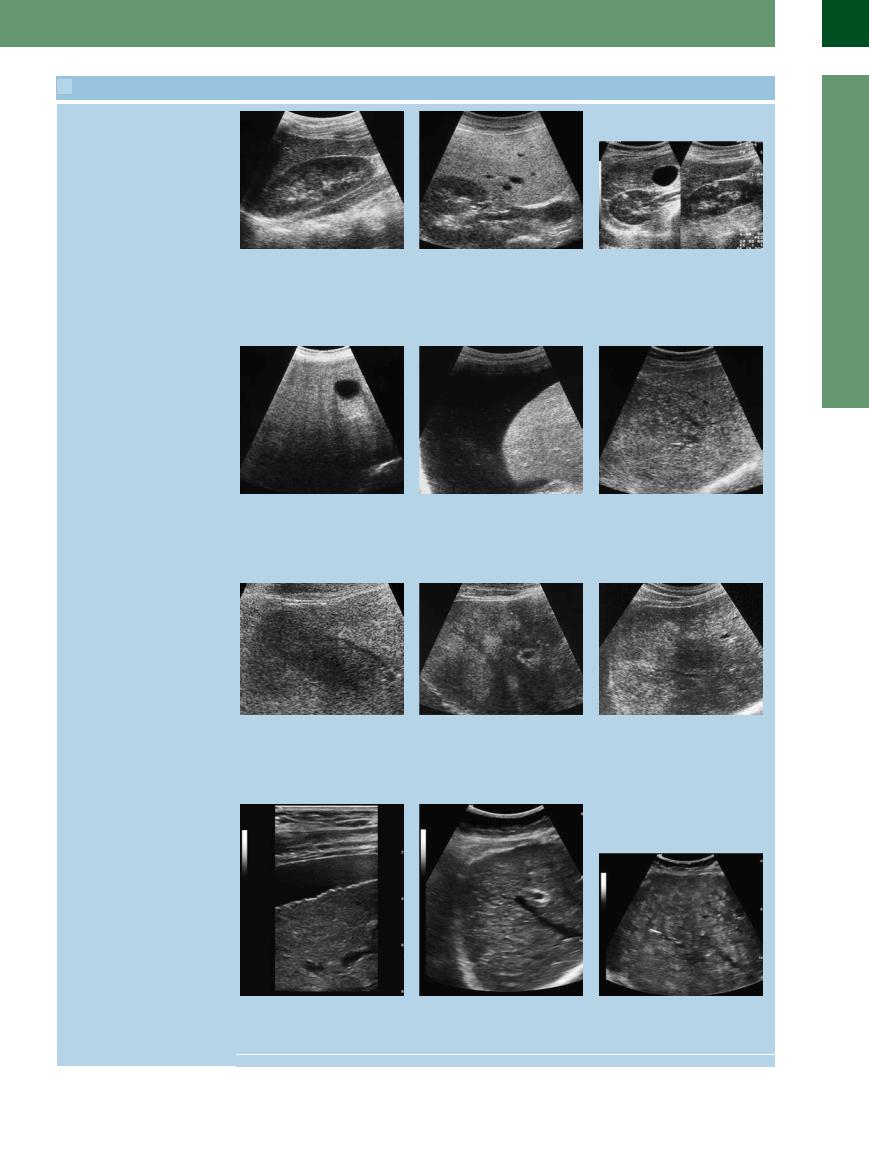
 2.4 Pathologic Liver Findings
2.4 Pathologic Liver Findings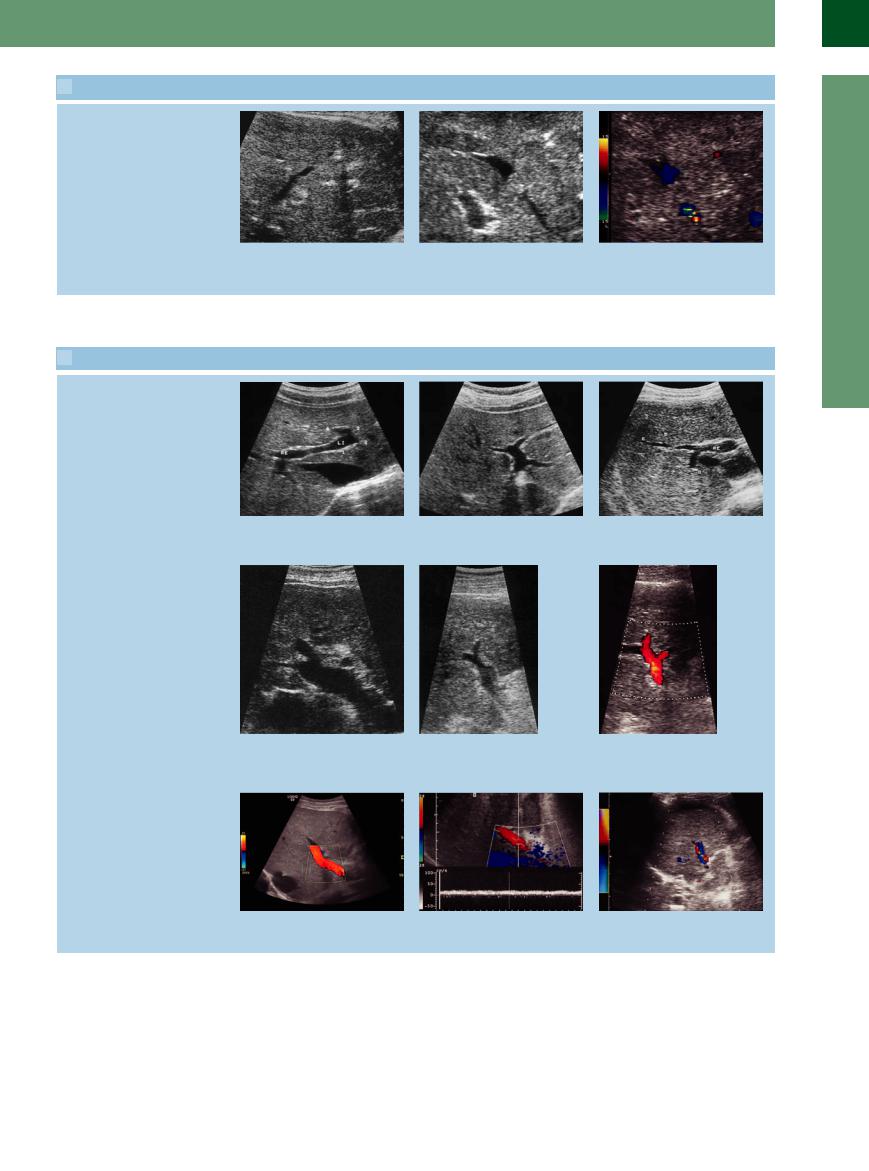
 2.4 Pathologic Liver Findings (Continued)
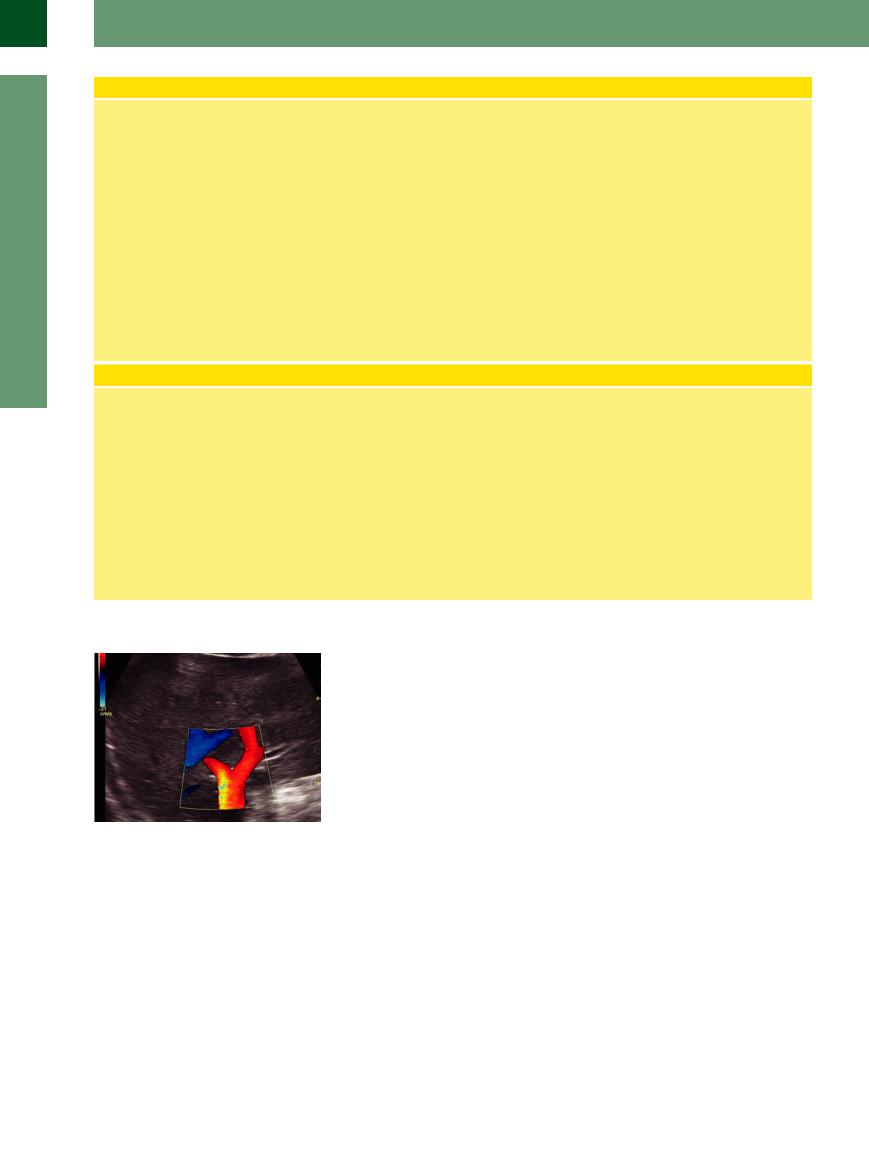
2.4 Pathologic Liver Findings (Continued) 2.5 Portal Veins
2.5 Portal Veins