

- •Contents
- •Preface
- •Contributors
- •1 Vessels
- •1.1 Aorta, Vena Cava, and Peripheral Vessels
- •Aorta, Arteries
- •Anomalies and Variant Positions
- •Dilatation
- •Stenosis
- •Wall Thickening
- •Intraluminal Mass
- •Perivascular Mass
- •Vena Cava, Veins
- •Anomalies
- •Dilatation
- •Intraluminal Mass
- •Compression, Infiltration
- •1.2 Portal Vein and Its Tributaries
- •Enlarged Lumen Diameter
- •Portal Hypertension
- •Intraluminal Mass
- •Thrombosis
- •Tumor
- •2 Liver
- •Enlarged Liver
- •Small Liver
- •Homogeneous Hypoechoic Texture
- •Homogeneous Hyperechoic Texture
- •Regionally Inhomogeneous Texture
- •Diffuse Inhomogeneous Texture
- •Anechoic Masses
- •Hypoechoic Masses
- •Isoechoic Masses
- •Hyperechoic Masses
- •Echogenic Masses
- •Irregular Masses
- •Differential Diagnosis of Focal Lesions
- •Diagnostic Methods
- •Suspected Diagnosis
- •3 Biliary Tree and Gallbladder
- •3.1 Biliary Tree
- •Thickening of the Bile Duct Wall
- •Localized and Diffuse
- •Bile Duct Rarefaction
- •Localized and Diffuse
- •Bile Duct Dilatation and Intraductal Pressure
- •Intrahepatic
- •Hilar and Prepancreatic
- •Intrapancreatic
- •Papillary
- •Abnormal Intraluminal Bile Duct Findings
- •Foreign Body
- •The Seven Most Important Questions
- •3.2 Gallbladder
- •Changes in Size
- •Large Gallbladder
- •Small/Missing Gallbladder
- •Wall Changes
- •General Hypoechogenicity
- •General Hyperechogenicity
- •General Tumor
- •Focal Tumor
- •Intraluminal Changes
- •Hyperechoic
- •Hypoechoic
- •Nonvisualized Gallbladder
- •Missing Gallbladder
- •Obscured Gallbladder
- •4 Pancreas
- •Diffuse Pancreatic Change
- •Large Pancreas
- •Small Pancreas
- •Hypoechoic Texture
- •Hyperechoic Texture
- •Focal Changes
- •Anechoic Lesion
- •Hypoechoic Lesion
- •Isoechoic Lesion
- •Hyperechoic Lesion
- •Irregular (Complex Structured) Lesion
- •Dilatation of the Pancreatic Duct
- •Marginal/Mild Dilatation
- •Marked Dilatation
- •5 Spleen
- •Nonfocal Changes of the Spleen
- •Diffuse Parenchymal Changes
- •Large Spleen
- •Small Spleen
- •Focal Changes of the Spleen
- •Anechoic Mass
- •Hypoechoic Mass
- •Hyperechoic Mass
- •Splenic Calcification
- •6 Lymph Nodes
- •Peripheral Lymph Nodes
- •Head/Neck
- •Extremities (Axilla, Groin)
- •Abdominal Lymph Nodes
- •Porta Hepatis
- •Splenic Hilum
- •Mesentery (Celiac, Upper and Lower Mesenteric Station)
- •Stomach
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •Small/Large Intestine
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •8 Peritoneal Cavity
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Wall Structures
- •Smooth Margin
- •Irregular Margin
- •Intragastric Processes
- •Intraintestinal Processes
- •9 Kidneys
- •Anomalies, Malformations
- •Aplasia, Hypoplasia
- •Cystic Malformation
- •Anomalies of Number, Position, or Rotation
- •Fusion Anomaly
- •Anomalies of the Renal Calices
- •Vascular Anomaly
- •Diffuse Changes
- •Large Kidneys
- •Small Kidneys
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Irregular Structure
- •Circumscribed Changes
- •Anechoic Structure
- •Hypoechoic or Isoechoic Structure
- •Complex Structure
- •Hyperechoic Structure
- •10 Adrenal Glands
- •Enlargement
- •Anechoic Structure
- •Hypoechoic Structure
- •Complex Echo Structure
- •Hyperechoic Structure
- •11 Urinary Tract
- •Malformations
- •Duplication Anomalies
- •Dilatations and Stenoses
- •Dilated Renal Pelvis and Ureter
- •Anechoic
- •Hypoechoic
- •Hypoechoic
- •Hyperechoic
- •Large Bladder
- •Small Bladder
- •Altered Bladder Shape
- •Intracavitary Mass
- •Hypoechoic
- •Hyperechoic
- •Echogenic
- •Wall Changes
- •Diffuse Wall Thickening
- •Circumscribed Wall Thickening
- •Concavities and Convexities
- •12.1 The Prostate
- •Enlarged Prostate
- •Regular
- •Irregular
- •Small Prostate
- •Regular
- •Echogenic
- •Circumscribed Lesion
- •Anechoic
- •Hypoechoic
- •Echogenic
- •12.2 Seminal Vesicles
- •Diffuse Change
- •Hypoechoic
- •Circumscribed Change
- •Anechoic
- •Echogenic
- •Irregular
- •12.3 Testis, Epididymis
- •Diffuse Change
- •Enlargement
- •Decreased Size
- •Circumscribed Lesion
- •Anechoic or Hypoechoic
- •Irregular/Echogenic
- •Epididymal Lesion
- •Anechoic
- •Hypoechoic
- •Intrascrotal Mass
- •Anechoic or Hypoechoic
- •Echogenic
- •13 Female Genital Tract
- •Masses
- •Abnormalities of Size or Shape
- •Uterus
- •Abnormalities of Size or Shape
- •Myometrial Changes
- •Intracavitary Changes
- •Endometrial Changes
- •Fallopian Tubes
- •Hypoechoic Mass
- •Anechoic Cystic Mass
- •Solid Echogenic or Nonhomogeneous Mass
- •14 Thyroid Gland
- •Diffuse Changes
- •Enlarged Thyroid Gland
- •Small Thyroid Gland
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Circumscribed Changes
- •Anechoic
- •Hypoechoic
- •Isoechoic
- •Hyperechoic
- •Irregular
- •Differential Diagnosis of Hyperthyroidism
- •Types of Autonomy
- •15 Pleura and Chest Wall
- •Chest Wall
- •Masses
- •Parietal Pleura
- •Nodular Masses
- •Diffuse Pleural Thickening
- •Pleural Effusion
- •Anechoic Effusion
- •Echogenic Effusion
- •Complex Effusion
- •16 Lung
- •Masses
- •Anechoic Masses
- •Hypoechoic Masses
- •Complex Masses
- •Index
7
Gastrointestinal Tract
Hypertrophic Pyloric Stenosis 











































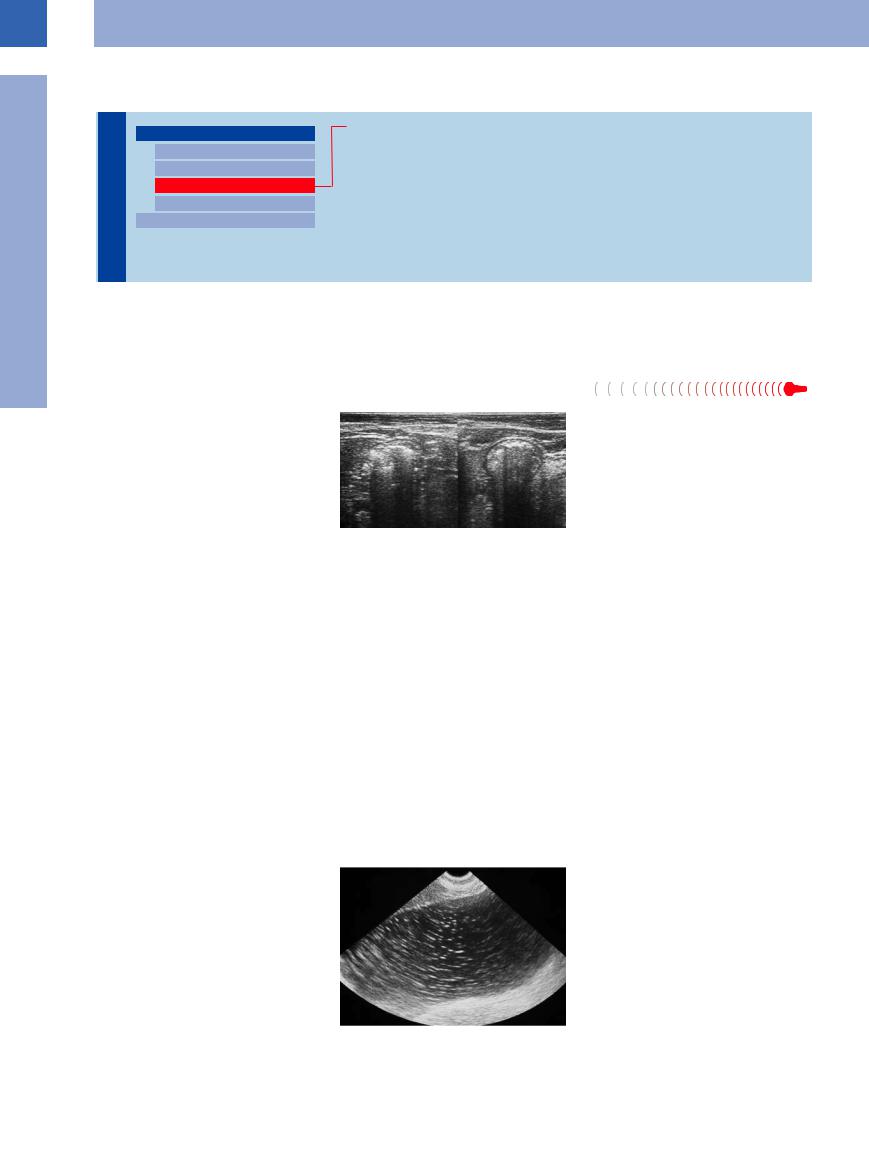
Hypertrophic pyloric stenosis (Fig. 7.13) is a relatively common condition affecting the newborn. Recurrent projectile vomiting is almost pathognomonic. On ultrasonography, the pylorus appears as a circumscribed lengthy circular thickening of the muscle, the total pyloric diameter being in excess of 12 mm and the pyloric canal being compressed (so-called “cervix sign”); in addition, the stomach will display marked fluid retention.
Fig. 7.13 Hypertrophic pyloric stenosis. So-called cervix sign with marked circumscribed thickening of the lamina propria mucosae and tight pyloric canal, accompanied by gastric distension and fluid retention.
Extended Wall Changes
Tract |
Stomach |
Carcinoma/Scirrhus |
|
Focal Wall Changes |
Lymphoma |
||
Gastrointestinal |
Extended Wall Changes |
Gastritis |
|
Dilated Lumen |
Congestion, Edema |
||
|
|||
|
Narrowed Lumen |
||
|
Peritoneal Carcinomatosis |
||
|
Small/Large Intestine |
||
|
|
||
Carcinoma/Scirrhus |
|
||
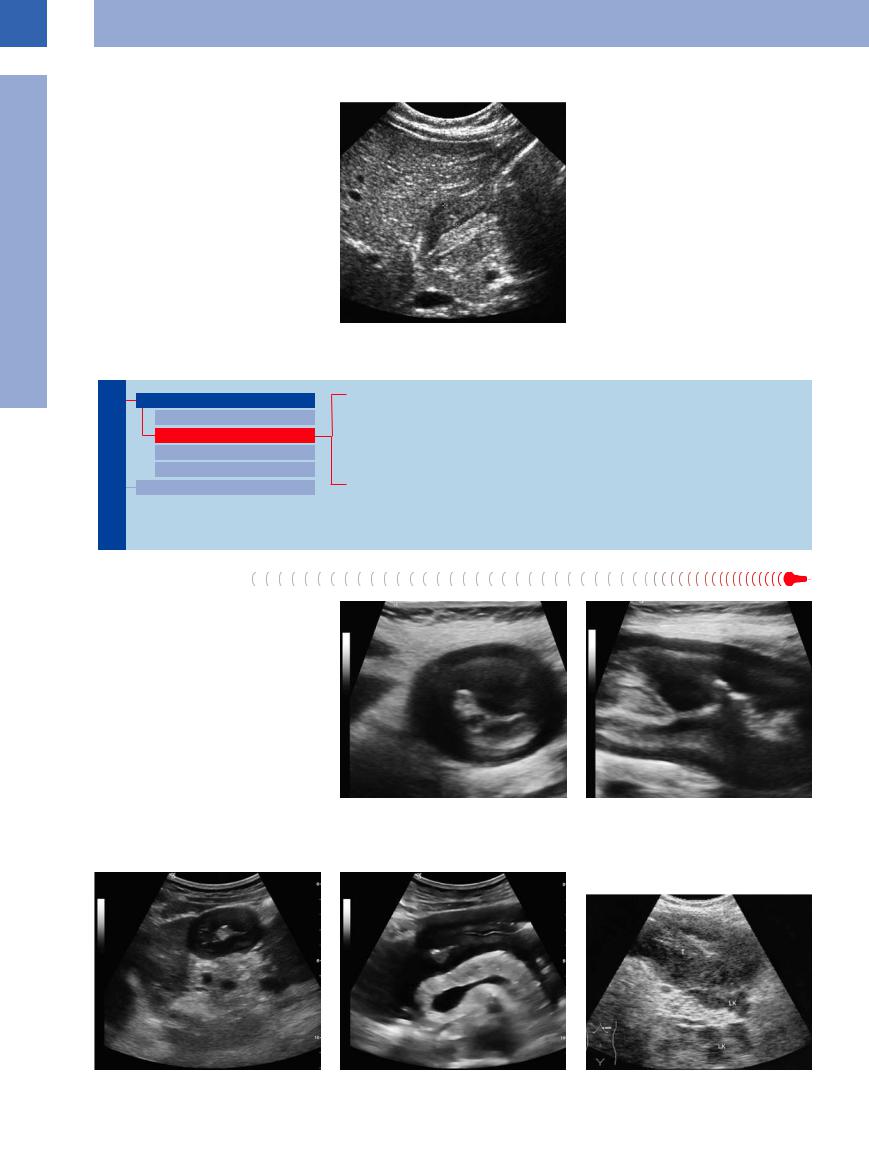
Adenocarcinoma of the stomach, especially scirrhous carcinoma, is characterized by diffuse extensive invasion of the gastric wall by the tumor, resulting in a narrowed lumen and loss of the layered wall architecture. Owing to the intramural spread of the carcinoma, the inner and outer margins of the gastric wall are still smoothly defined irrespective of a possible wall thickness of several centimeters. The region of the tumor will be devoid of any peristaltic movement, and the pathological gut signature will demonstrate a coarse texture and lack any pliability (Figs. 7.14, 7.15, 7.16).
Fig. 7.14 Scirrhous carcinoma. Oblong abnormal target |
b Transverse section. |
sign produced by a scirrhous signet-ring cell carcinoma of |
|
the stomach. |
|
a Longitudinal section. |
|
Fig. 7.15a and b Adenocarcinoma of the gastric antrum. |
b Transverse scan. |
Fig. 7.16 Gastric lymphoma: diffuse tumor invasion of the |
a Longitudinal scan. |
|
gastric wall (T) with lymph node metastasis (LK). |
270

Lymphoma






















































Diffuse invasion of the gastric wall by lymphoma may lead to clearly recognizable irregular and noncompliant hypoechoic thickening of the wall, with easily visualized hypervascularity and loss of its layered architecture.
Gastritis 























































The different types of gastritis (Helicobacter pylori infection, long-term therapy with proton pump inhibitors), as well as Ménétrier disease, display a markedly pronounced emphasis of the layering and rugal coarsening (Fig. 7.17).
Fig. 7.17 Hypertrophic gastric corpus giant-fold gastritis in Ménétrier disease.
a Longitudinal section.
b Transverse section.
Congestion, Edema 







Congestion. In cardiac congestion, the outer layers of the gastric wall will undergo a marked hypoechoic thickening; other signs of the cardiac congestion will always be present as well (distended hepatic veins, engorged vena cava, possibly ascites, and pleural effusion).
Edema. Concomitant inflammatory reaction of the gastric wall as part of pancreatitis could result in a more pronounced appearance of the layering as well as discrete extended thickening of the gastric wall. Owing to the concurrent paralytic ileus, there is no peristalsis and the pliability of the wall is diminished by the inflammatory invasion.
Peritoneal Carcinomatosis 













































As part of diffuse peritoneal carcinomatosis the gastric wall may undergo appositional thickening from the outside, and it is quite typical of these cases that marked ascites can frequently be demonstrated.
7
Stomach
271
7
Gastrointestinal Tract
Dilated Lumen
Tract |
|
|
Stomach |
|
Physiological Dilatation |
|
|
||||||
|
|
|
Focal Wall Changes |
|
Inflammation |
|
Gastrointestinal |
|
|
|
Extended Wall Changes |
|
Gastric Outlet Obstruction |
|
|
|
Dilated Lumen |
|
Functional Disorder |
|
|
|
|
|
|
||
|
|
|
|
|||
|
|
|
|
Narrowed Lumen |
|
|
|
|
|
Small/Large Intestine |
|
|
|
|
|
|
|
|||
Being a storage organ, the stomach may hold |
the fasting state (6 hours, at most 12 hours, |
up to 2000 mL of food even under physiological |
after the last ingestion) under physiological |
conditions. Conditioning and disease/disorders |
conditions the stomach will empty com- |
can increase this volume beyond 3000 mL. In |
pletely; with the patient in the supine position |
Physiological Dilatation
























The postprandial chyme can be visualized at the gastric fundus with the patient in the supine position (Fig. 7.18). Peristaltic activity will mix it and then transport it to the gastric outlet, where it is portioned through the pylorus into the duodenum. Here, the chyme becomes visible only because of the peristalsis and can then be demonstrated within the lumen along its brief passage through the duodenum.
the small residual secretion of about 50 mL can be demonstrated at the gastric fundus. The echogenicity of the gastric contents depends on the type of food ingested.
Fig. 7.18 Postprandial lumen of the stomach, markedly dilated by ingesta; thinned out, dilated gastric wall.
Inflammation 




















































When dealing with inflammation near the du- |
logical and diminished peristalsis with sloshing |
neath the fluid and gas and can be churned by |
odenal arch (pancreatitis, cholecystitis, compli- |
of the fluid. At the same time, the gastric lumen |
deliberate palpation or by repositioning the |
cated ulcer, ileus) one can always demonstrate |
will contain an increased quantity of food par- |
patient. |
fluid within the duodenal lumen (indirect |
ticles and fluid. Because of the lack of peristal- |
|
sign), the latter displaying a markedly patho- |
sis, the solid particles will settle in layers be- |
|
Gastric Outlet Obstruction 













































Gastric outlet stenosis or obstruction by the duodenum will result in a markedly ectatic stomach, retaining the food and fluid previously ingested as well as the increased amount of gastric juice produced.
Functional  Disorder
Disorder

















































Functional disorders of gastric emptying are |
Fig. 7.19 Pathological dilatation of the stomach in dia- |
encountered in ileus and diabetic gastroparesis |
betic gastroparesis (in this case > 3000 mL of hematinic |
(Fig. 7.19); here, it is primarily the retention of |
fasting secretion was drained). |
fluid characterized by fine echoes. |
|
272
Narrowed Lumen
Tract |
|
|
Stomach |
|
|
|
|
||
|
|
|
|
Focal Wall Changes |
Gastrointestinal |
|
|
|
Extended Wall Changes |
|
|
|
Dilated Lumen |
|
|
|
|
|
|
|
|
|
|
Narrowed Lumen |
|
|
|
|
|
|
|
|
Small/Large Intestine |
|
|
|
|||
In fasting, peristaltic movement of the antrum will result in concentric contraction of the gastric wall with complete loss of the lumen; depending on the degree of prefilling, this narrowing of the lumen may be incomplete.
Impression
Compression
Tumor
Postoperative Status
Impression






















































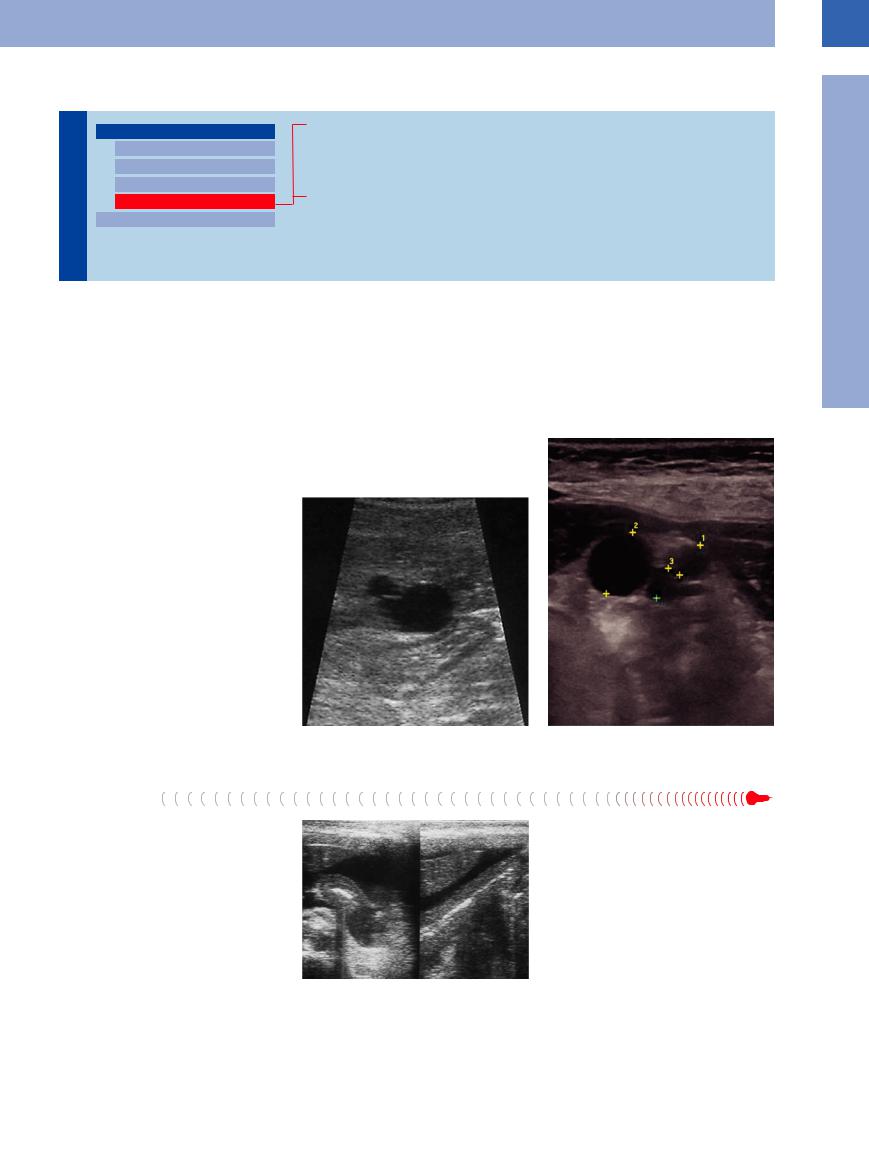
Impression of the stomach from the outside may result in eccentric narrowing of the gastric lumen, the primary such cause being masses in adjacent organs, e. g., hepatic (Fig. 7.20, Fig. 7.21) or pancreatic cysts, but also the gallbladder.
7
Stomach
Compression
Compression of the gastric lumen from the outside is seen in massive ascites (e. g., in peritoneal carcinomatosis; Fig. 7.22) and severe pancreatitis with retroperitoneal edema and ascites.
Fig. 7.20 Anterior impression of the stomach by a liver |
Fig. 7.21 Posterior impression of the stomach by a cyst- |
cyst. |
adenoma of the pancreas. |
Fig. 7.22 Gastric compression by ascites in a gynecologic tumor with peritoneal carcinomatosis, the stomach lacking any dilatability.
273