

- •Contents
- •Preface
- •Contributors
- •1 Vessels
- •1.1 Aorta, Vena Cava, and Peripheral Vessels
- •Aorta, Arteries
- •Anomalies and Variant Positions
- •Dilatation
- •Stenosis
- •Wall Thickening
- •Intraluminal Mass
- •Perivascular Mass
- •Vena Cava, Veins
- •Anomalies
- •Dilatation
- •Intraluminal Mass
- •Compression, Infiltration
- •1.2 Portal Vein and Its Tributaries
- •Enlarged Lumen Diameter
- •Portal Hypertension
- •Intraluminal Mass
- •Thrombosis
- •Tumor
- •2 Liver
- •Enlarged Liver
- •Small Liver
- •Homogeneous Hypoechoic Texture
- •Homogeneous Hyperechoic Texture
- •Regionally Inhomogeneous Texture
- •Diffuse Inhomogeneous Texture
- •Anechoic Masses
- •Hypoechoic Masses
- •Isoechoic Masses
- •Hyperechoic Masses
- •Echogenic Masses
- •Irregular Masses
- •Differential Diagnosis of Focal Lesions
- •Diagnostic Methods
- •Suspected Diagnosis
- •3 Biliary Tree and Gallbladder
- •3.1 Biliary Tree
- •Thickening of the Bile Duct Wall
- •Localized and Diffuse
- •Bile Duct Rarefaction
- •Localized and Diffuse
- •Bile Duct Dilatation and Intraductal Pressure
- •Intrahepatic
- •Hilar and Prepancreatic
- •Intrapancreatic
- •Papillary
- •Abnormal Intraluminal Bile Duct Findings
- •Foreign Body
- •The Seven Most Important Questions
- •3.2 Gallbladder
- •Changes in Size
- •Large Gallbladder
- •Small/Missing Gallbladder
- •Wall Changes
- •General Hypoechogenicity
- •General Hyperechogenicity
- •General Tumor
- •Focal Tumor
- •Intraluminal Changes
- •Hyperechoic
- •Hypoechoic
- •Nonvisualized Gallbladder
- •Missing Gallbladder
- •Obscured Gallbladder
- •4 Pancreas
- •Diffuse Pancreatic Change
- •Large Pancreas
- •Small Pancreas
- •Hypoechoic Texture
- •Hyperechoic Texture
- •Focal Changes
- •Anechoic Lesion
- •Hypoechoic Lesion
- •Isoechoic Lesion
- •Hyperechoic Lesion
- •Irregular (Complex Structured) Lesion
- •Dilatation of the Pancreatic Duct
- •Marginal/Mild Dilatation
- •Marked Dilatation
- •5 Spleen
- •Nonfocal Changes of the Spleen
- •Diffuse Parenchymal Changes
- •Large Spleen
- •Small Spleen
- •Focal Changes of the Spleen
- •Anechoic Mass
- •Hypoechoic Mass
- •Hyperechoic Mass
- •Splenic Calcification
- •6 Lymph Nodes
- •Peripheral Lymph Nodes
- •Head/Neck
- •Extremities (Axilla, Groin)
- •Abdominal Lymph Nodes
- •Porta Hepatis
- •Splenic Hilum
- •Mesentery (Celiac, Upper and Lower Mesenteric Station)
- •Stomach
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •Small/Large Intestine
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •8 Peritoneal Cavity
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Wall Structures
- •Smooth Margin
- •Irregular Margin
- •Intragastric Processes
- •Intraintestinal Processes
- •9 Kidneys
- •Anomalies, Malformations
- •Aplasia, Hypoplasia
- •Cystic Malformation
- •Anomalies of Number, Position, or Rotation
- •Fusion Anomaly
- •Anomalies of the Renal Calices
- •Vascular Anomaly
- •Diffuse Changes
- •Large Kidneys
- •Small Kidneys
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Irregular Structure
- •Circumscribed Changes
- •Anechoic Structure
- •Hypoechoic or Isoechoic Structure
- •Complex Structure
- •Hyperechoic Structure
- •10 Adrenal Glands
- •Enlargement
- •Anechoic Structure
- •Hypoechoic Structure
- •Complex Echo Structure
- •Hyperechoic Structure
- •11 Urinary Tract
- •Malformations
- •Duplication Anomalies
- •Dilatations and Stenoses
- •Dilated Renal Pelvis and Ureter
- •Anechoic
- •Hypoechoic
- •Hypoechoic
- •Hyperechoic
- •Large Bladder
- •Small Bladder
- •Altered Bladder Shape
- •Intracavitary Mass
- •Hypoechoic
- •Hyperechoic
- •Echogenic
- •Wall Changes
- •Diffuse Wall Thickening
- •Circumscribed Wall Thickening
- •Concavities and Convexities
- •12.1 The Prostate
- •Enlarged Prostate
- •Regular
- •Irregular
- •Small Prostate
- •Regular
- •Echogenic
- •Circumscribed Lesion
- •Anechoic
- •Hypoechoic
- •Echogenic
- •12.2 Seminal Vesicles
- •Diffuse Change
- •Hypoechoic
- •Circumscribed Change
- •Anechoic
- •Echogenic
- •Irregular
- •12.3 Testis, Epididymis
- •Diffuse Change
- •Enlargement
- •Decreased Size
- •Circumscribed Lesion
- •Anechoic or Hypoechoic
- •Irregular/Echogenic
- •Epididymal Lesion
- •Anechoic
- •Hypoechoic
- •Intrascrotal Mass
- •Anechoic or Hypoechoic
- •Echogenic
- •13 Female Genital Tract
- •Masses
- •Abnormalities of Size or Shape
- •Uterus
- •Abnormalities of Size or Shape
- •Myometrial Changes
- •Intracavitary Changes
- •Endometrial Changes
- •Fallopian Tubes
- •Hypoechoic Mass
- •Anechoic Cystic Mass
- •Solid Echogenic or Nonhomogeneous Mass
- •14 Thyroid Gland
- •Diffuse Changes
- •Enlarged Thyroid Gland
- •Small Thyroid Gland
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Circumscribed Changes
- •Anechoic
- •Hypoechoic
- •Isoechoic
- •Hyperechoic
- •Irregular
- •Differential Diagnosis of Hyperthyroidism
- •Types of Autonomy
- •15 Pleura and Chest Wall
- •Chest Wall
- •Masses
- •Parietal Pleura
- •Nodular Masses
- •Diffuse Pleural Thickening
- •Pleural Effusion
- •Anechoic Effusion
- •Echogenic Effusion
- •Complex Effusion
- •16 Lung
- •Masses
- •Anechoic Masses
- •Hypoechoic Masses
- •Complex Masses
- •Index
16Lung
C. Goerg
Transcutaneous ultrasound is limited in its ability to define the thoracic organs. Although sonography quickly became an established tool for pleural examination, it was not until the late 1980s that systematic studies of the lung by Mathis et al.1 led to a greater acceptance of pulmonary ultrasound.
There are several physical and acoustic phenomena that chiefly limit the intrathoracic use of ultrasound. The ribs, sternum, spinal column, and scapula create diagnostic “dead spaces” by reflecting virtually all incident sound. Also, very large differences in acoustic impedance exist at interfaces between lung tissue and aerated alveoli, causing almost
100% reflection of sound waves. Central lung regions cannot be scanned through normally aerated peripheral lung tissue.
As a result, thoracic ultrasound is currently used as an adjunctive, complementary procedure for investigating diffuse radiographic opacities located near the pleura.2,3
Topography and Ultrasound Morphology
Ultrasound Morphology 





































Relations of the lungs
●Intrathoracic
●Bounded by the ribs, sternum, and diaphragm
Sonographic landmarks
●Sharp, mobile, high-amplitude echo at the lung–pleura interface
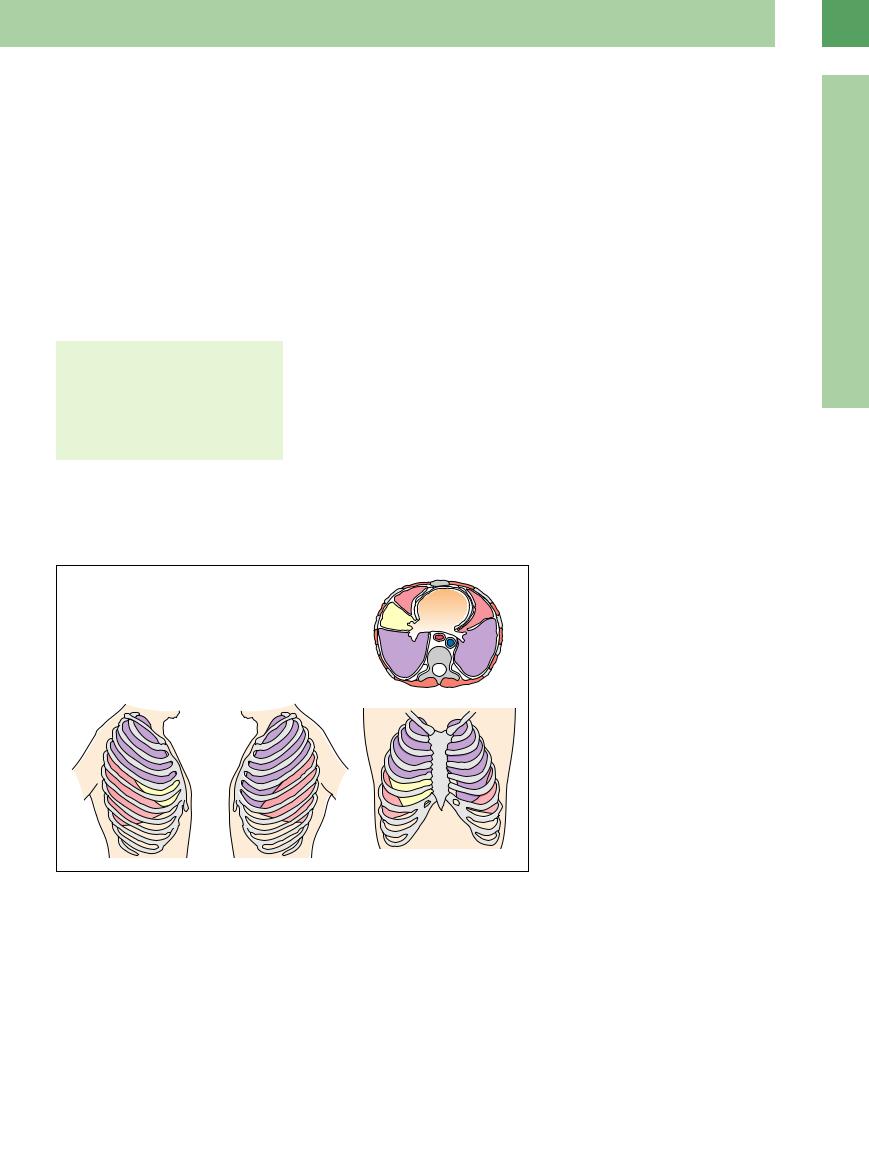
The lungs are intrathoracic and are bounded by the thoracic skeleton. The chest cavity is bounded inferiorly by the diaphragm. The upper lobes are covered posteriorly by the scapulae. The lower lobes can be visualized by scanning through the intercostal spaces, which are directed obliquely downward. The anterior rib segments are more horizontal, and the upper lobes can be scanned at that level through the intercostal spaces on both sides. The middle lobe can be scanned from a parasternal probe position on the right side (Fig.16.1). The lower lung fields can be eval-
uated with a subcostal scan through the liver (right lung) or through the spleen (left lung), the transhepatic scan providing the better view. The trans-splenic window is frequently obscured by gas in the stomach or colon. The apical lung regions are best demonstrated by a supraclavicular scan angled toward the feet. The range of intercostal sound transmission normally extends to the visceral pleura and ends at the aerated alveoli, which reflect all incident sound. The typical echogenic pleural line is produced by total sound reflection at the pleura–lung interface (the “entry echo”).
Fig. 16.1 Anatomic relations of the pulmonary lobes.
16
Masses
■ Masses
Because mass lesions of the chest wall and pleura as well as peripheral lung diseases promote sound transmission, they can be imaged with transcutaneous ultrasound. Chest-wall and pleural lesions can exert extrinsic pressure on the lung, displacing air from the tissue and enabling it to transmit sound (e. g., compression atelectasis due to pleural effusion). These lesions are distinguished from actual intrapul-
monary masses that cause absent or decreased aeration of the lung parenchyma. Only the latter type of lesion is discussed here.
Criteria for ultrasound evaluation. The sonographic evaluation of peripheral lung masses is based on their number, location, size, shape, margins, echogenicity, and homogeneity. The behavior of the focal lesion during respiratory
excursions has proved to be an important criterion.
Color Doppler ultrasound can supply additional information that is useful in characterizing lesions. It can provide qualitative information on the display of color-flow signals that is useful for classifying lesions as avascular, hypovascular, or hypervascular. These signals are dependent on the quality of the equipment
533
16
Lung
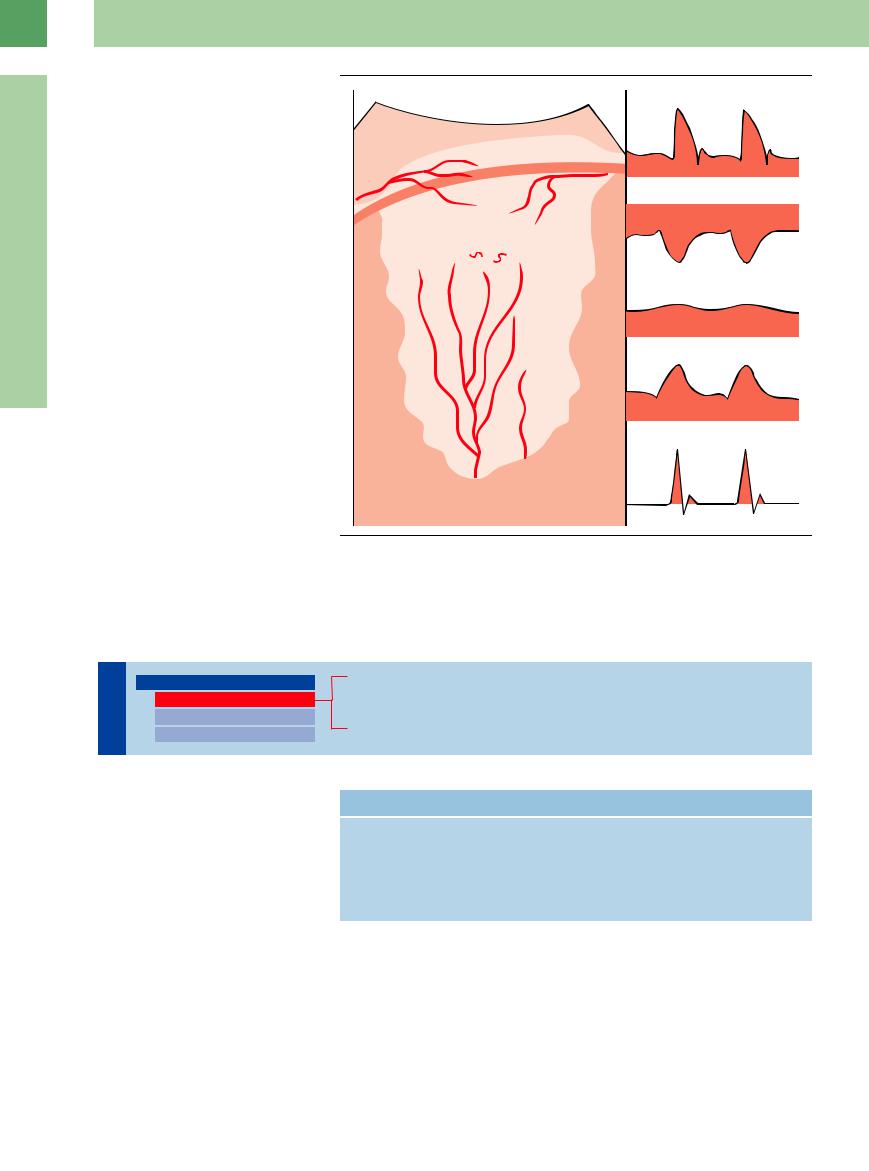
for contrast medium perfusion makes it possible to distinguish between the pulmonary and bronchial arteries. CEUS is valuable even in identifying areas of consolidated lung tissue without perfusion.
The interpretation of ultrasound findings also depends on the history, the clinical presentation, and the results of follow-up scans. In some cases a definitive interpretation may require ultrasound-guided fine-needle aspiration (FNA).5
Fig. 16.2 Schematic illustration of lung vascularization with corresponding presentation of spectral curves. ICA = intercostal arteries; pBA = peripheral bronchial artery; TN = cancer neoangiogenesis, cBA = central bronchial artery; PA = pulmonary artery.
Anechoic Masses
Lung |
Masses |
|||
|
|
|
||
|
|
|
|
Anechoic Masses |
|
|
|
|
|
|
|
|
|
Hypoechoic Masses |
|
|
|
|
Complex Masses |
Loculated Pleural Effusion
Pulmonary Cyst, Liquefaction, Abscess
Aortic Aneurysm, Cardiac Cavity
A loculated pleural effusion is the most frequent cause of an anechoic mass between the lung and chest wall. Differentiation is required from rare anechoic lung masses, which can be defined with ultrasound if they reach the parenchymal surface (Table 16.1,  16.1).
16.1).
Table 16.1 Differential diagnosis of echo-free masses
Common |
Less common |
Loculated e usion in a lobar fissure |
Lung abscess |
|
Primary lung cyst |
|
Liquefying tumor |
|
Liquefying atelectasis |
|
Aortic aneurysm on the chest wall |
|
Cardiac cavity abutting the chest wall |
534

Loculated Pleural Effusion 













































Localized anechoic masses between the lung and chest wall most likely represent a loculated pleural effusion (Fig.16.3). An exudative type of effusion is usually present. The underlying disease may be an infection or malignant process.
Pulmonary Cyst,
Cyst, Liquefaction, Abscess
Liquefaction, Abscess
Fig. 16.3 Bronchial carcinoma in a 45-year-old man. Left lateral intercostal scan shows the bright entry echo at the interface of the pleura and lung (LU) cranial to the spleen (SP). A rounded, echo-free mass rimmed by solid echogenic material is visible in the costophrenic angle. It is consistent with a loculated effusion in pleural carcinomatosis.
Pulmonary cysts are rare and are subdivided |
Liquefying processes (pneumonic infiltrates, |
They have an echogenic wall and produce char- |
into primary and secondary forms ( |
tumors, metastases) can occasionally appear |
acteristic clinical symptoms. Abscessation can |
16.1a,d–f). |
anechoic ( 16.1j–k). |
be confirmed by ultrasound-guided percutane- |
|
Lung abscesses usually have a complex echo |
ous aspiration. |
|
texture but may also appear anechoic ( 16.1 l). |
|
 16.1 Pulmonary Cysts, Liquefaction, and Abscesses
16.1 Pulmonary Cysts, Liquefaction, and Abscesses
Cyst, aspergilloma
16
Masses
a A 67-year-old woman with a 12-year |
b and c A 49-year-old man with leukemia |
history of a constant peripheral lung |
and fever. |
mass. Parasternal scan demonstrates an |
b Chest radiograph shows multiple pul- |
echo-free mass with irregular margins in |
monary nodules. |
the right parasternal region, consistent |
|
with a pulmonary cyst (Cy). c = secondary |
|
cysts. |
|
Peripheral pulmonary nodule
d–f Peripheral lung nodule in a 74-year-old |
e Over the next 2 months the mass |
man. |
resolves into a cystic focus, presumably |
d Initially complex lung mass. |
the result of pneumonia or infarction. |
c Right lateral intercostal scan shows an almost echo-free mass in the lung (LU), identified histologically as an aspergilloma.
f CT: peripheral lung nodule.
535

16
Lung
 16.1 Pulmonary Cysts, Liquefaction, and Abscesses (Continued)
16.1 Pulmonary Cysts, Liquefaction, and Abscesses (Continued)
Liquefaction, cystic tumor, abscess
g A 38-year-old man with fever. Right anterior intercostal scan shows di use hypoechoic transformation of the lung with central liquefaction (A) consistent with cavitating pneumonia. INF = infarction; LU = lung.
j and k A 33-year-old woman with known sarcoma and a large right thoracic metastasis.
j Color duplex demonstrates a cystic-solid mass with color-flow signals in the solid components.
h and i Bronchial carcinoma.
h Chest radiograph shows complete opacification of the left hemithorax.
k Sampled waveforms display a highresistance “extremity” pattern in pulmonary arterial vessels and a low-resistance “parenchymal” pattern in tumor vessels.
i Left lateral intercostal scan shows pleural e usion (PE) with upper (UL) and lower lobar atelectasis. The lower lobe contains a central hypoechoic area (arrows) consistent with liquefaction.
l A 79-year-old man with fever and dyspnea. Left lateral intercostal scan shows a large, echo-free mass with irregular margins and central air echoes (arrow) cranial to the spleen (SP). Percutaneous aspiration of the mass yielded pus. A = abscess; SP = spleen.
Aortic Aneurysm,  Cardiac
Cardiac Cavity
Cavity










































An aortic aneurysm bordering the chest wall and a cardiac cavity abutting the chest wall due to cardiomegaly are rare differential diagnoses for a hypoechoic mass; they illustrate the im-
portance of seeing the chest radiograph before making a definitive interpretation of the ultrasound findings. An easy distinction can be made by color Doppler (Fig.16.4).
Fig. 16.4 A 67-year-old man with mediastinal widening in |
b Color Doppler shows arterial turbulence within the |
c MRI confirms the diagnosis of a dissecting thoracic |
the chest radiograph. |
mass. |
aortic aneurysm. |
a Ultrasound shows a rounded, hypoechoic mass with a |
|
|
septum (arrows) in the left paravertebral region. SC = |
|
|
spinal column; LU = lung. |
|
|
536