

- •Contents
- •Preface
- •Contributors
- •1 Vessels
- •1.1 Aorta, Vena Cava, and Peripheral Vessels
- •Aorta, Arteries
- •Anomalies and Variant Positions
- •Dilatation
- •Stenosis
- •Wall Thickening
- •Intraluminal Mass
- •Perivascular Mass
- •Vena Cava, Veins
- •Anomalies
- •Dilatation
- •Intraluminal Mass
- •Compression, Infiltration
- •1.2 Portal Vein and Its Tributaries
- •Enlarged Lumen Diameter
- •Portal Hypertension
- •Intraluminal Mass
- •Thrombosis
- •Tumor
- •2 Liver
- •Enlarged Liver
- •Small Liver
- •Homogeneous Hypoechoic Texture
- •Homogeneous Hyperechoic Texture
- •Regionally Inhomogeneous Texture
- •Diffuse Inhomogeneous Texture
- •Anechoic Masses
- •Hypoechoic Masses
- •Isoechoic Masses
- •Hyperechoic Masses
- •Echogenic Masses
- •Irregular Masses
- •Differential Diagnosis of Focal Lesions
- •Diagnostic Methods
- •Suspected Diagnosis
- •3 Biliary Tree and Gallbladder
- •3.1 Biliary Tree
- •Thickening of the Bile Duct Wall
- •Localized and Diffuse
- •Bile Duct Rarefaction
- •Localized and Diffuse
- •Bile Duct Dilatation and Intraductal Pressure
- •Intrahepatic
- •Hilar and Prepancreatic
- •Intrapancreatic
- •Papillary
- •Abnormal Intraluminal Bile Duct Findings
- •Foreign Body
- •The Seven Most Important Questions
- •3.2 Gallbladder
- •Changes in Size
- •Large Gallbladder
- •Small/Missing Gallbladder
- •Wall Changes
- •General Hypoechogenicity
- •General Hyperechogenicity
- •General Tumor
- •Focal Tumor
- •Intraluminal Changes
- •Hyperechoic
- •Hypoechoic
- •Nonvisualized Gallbladder
- •Missing Gallbladder
- •Obscured Gallbladder
- •4 Pancreas
- •Diffuse Pancreatic Change
- •Large Pancreas
- •Small Pancreas
- •Hypoechoic Texture
- •Hyperechoic Texture
- •Focal Changes
- •Anechoic Lesion
- •Hypoechoic Lesion
- •Isoechoic Lesion
- •Hyperechoic Lesion
- •Irregular (Complex Structured) Lesion
- •Dilatation of the Pancreatic Duct
- •Marginal/Mild Dilatation
- •Marked Dilatation
- •5 Spleen
- •Nonfocal Changes of the Spleen
- •Diffuse Parenchymal Changes
- •Large Spleen
- •Small Spleen
- •Focal Changes of the Spleen
- •Anechoic Mass
- •Hypoechoic Mass
- •Hyperechoic Mass
- •Splenic Calcification
- •6 Lymph Nodes
- •Peripheral Lymph Nodes
- •Head/Neck
- •Extremities (Axilla, Groin)
- •Abdominal Lymph Nodes
- •Porta Hepatis
- •Splenic Hilum
- •Mesentery (Celiac, Upper and Lower Mesenteric Station)
- •Stomach
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •Small/Large Intestine
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •8 Peritoneal Cavity
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Wall Structures
- •Smooth Margin
- •Irregular Margin
- •Intragastric Processes
- •Intraintestinal Processes
- •9 Kidneys
- •Anomalies, Malformations
- •Aplasia, Hypoplasia
- •Cystic Malformation
- •Anomalies of Number, Position, or Rotation
- •Fusion Anomaly
- •Anomalies of the Renal Calices
- •Vascular Anomaly
- •Diffuse Changes
- •Large Kidneys
- •Small Kidneys
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Irregular Structure
- •Circumscribed Changes
- •Anechoic Structure
- •Hypoechoic or Isoechoic Structure
- •Complex Structure
- •Hyperechoic Structure
- •10 Adrenal Glands
- •Enlargement
- •Anechoic Structure
- •Hypoechoic Structure
- •Complex Echo Structure
- •Hyperechoic Structure
- •11 Urinary Tract
- •Malformations
- •Duplication Anomalies
- •Dilatations and Stenoses
- •Dilated Renal Pelvis and Ureter
- •Anechoic
- •Hypoechoic
- •Hypoechoic
- •Hyperechoic
- •Large Bladder
- •Small Bladder
- •Altered Bladder Shape
- •Intracavitary Mass
- •Hypoechoic
- •Hyperechoic
- •Echogenic
- •Wall Changes
- •Diffuse Wall Thickening
- •Circumscribed Wall Thickening
- •Concavities and Convexities
- •12.1 The Prostate
- •Enlarged Prostate
- •Regular
- •Irregular
- •Small Prostate
- •Regular
- •Echogenic
- •Circumscribed Lesion
- •Anechoic
- •Hypoechoic
- •Echogenic
- •12.2 Seminal Vesicles
- •Diffuse Change
- •Hypoechoic
- •Circumscribed Change
- •Anechoic
- •Echogenic
- •Irregular
- •12.3 Testis, Epididymis
- •Diffuse Change
- •Enlargement
- •Decreased Size
- •Circumscribed Lesion
- •Anechoic or Hypoechoic
- •Irregular/Echogenic
- •Epididymal Lesion
- •Anechoic
- •Hypoechoic
- •Intrascrotal Mass
- •Anechoic or Hypoechoic
- •Echogenic
- •13 Female Genital Tract
- •Masses
- •Abnormalities of Size or Shape
- •Uterus
- •Abnormalities of Size or Shape
- •Myometrial Changes
- •Intracavitary Changes
- •Endometrial Changes
- •Fallopian Tubes
- •Hypoechoic Mass
- •Anechoic Cystic Mass
- •Solid Echogenic or Nonhomogeneous Mass
- •14 Thyroid Gland
- •Diffuse Changes
- •Enlarged Thyroid Gland
- •Small Thyroid Gland
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Circumscribed Changes
- •Anechoic
- •Hypoechoic
- •Isoechoic
- •Hyperechoic
- •Irregular
- •Differential Diagnosis of Hyperthyroidism
- •Types of Autonomy
- •15 Pleura and Chest Wall
- •Chest Wall
- •Masses
- •Parietal Pleura
- •Nodular Masses
- •Diffuse Pleural Thickening
- •Pleural Effusion
- •Anechoic Effusion
- •Echogenic Effusion
- •Complex Effusion
- •16 Lung
- •Masses
- •Anechoic Masses
- •Hypoechoic Masses
- •Complex Masses
- •Index
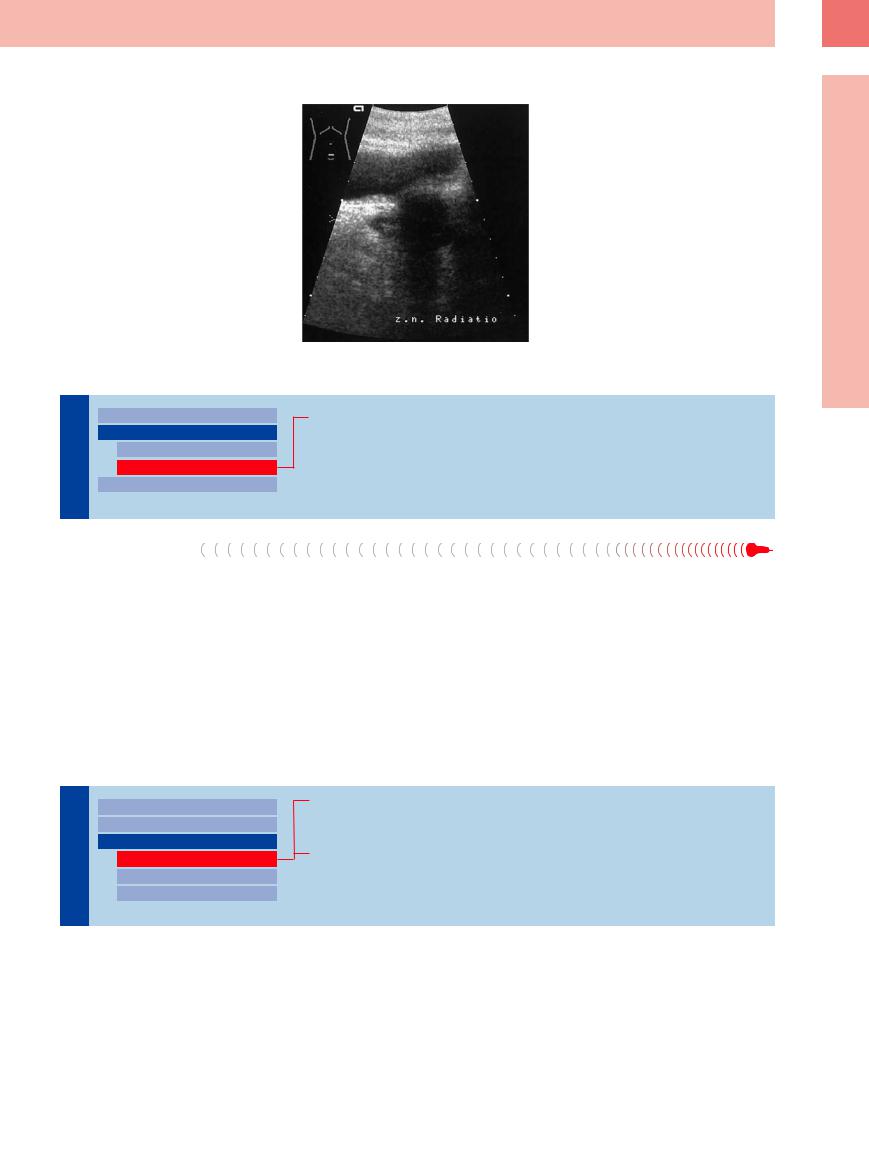
Radiation Therapy


















































The goal of radiation therapy is complete tu- |
Fig. 12.13 State after radiotherapy of the prostate as a |
mor destruction. The irradiation also leads to |
consequence of cancer: echo with bright shadow in the |
atrophy and size reduction of the remaining |
site of the prostate. |
|
|
gland. A tissue increase discovered at ultra- |
|
sound suggests a recurrence or, more likely, |
|
the local regrowth of residual tumor |
|
(Fig.12.13). |
|
12
Circumscribed Lesion
Echogenic
Prostate |
|
|
|
Enlarged Prostate |
|
|
|
|
|
||
|
|
|
|
Small Prostate |
|
|
|
|
|
||
|
|
|
|
|
Regular |
The |
|
|
|
|
Echogenic |
|
|
|
|
||
|
|
|
Circumscribed Lesion |
||
|
|
|
|
||
Chronic Prostatitis
Chronic Prostatitis
The prostate in the end stage of chronic prostatitis is small (Fig.12.11), consisting only of glandular remnants and dense lesions such as fibrosis or calcifications. Such changes are also commonly seen in prostatic hyperplasia—at times incidentally—with no prior clinical manifestations of chronic prostatitis.
■ Circumscribed Lesion
Anechoic
Prostate |
|
|
|
Enlarged Prostate |
|
|
|
|
|
||
|
|
|
|
Small Prostate |
|
|
|
||||
|
|
|
|
Circumscribed Lesion |
|
|
|
|
|
||
The |
|
|
|
|
Anechoic |
|
|
|
|
||
|
|
|
|
Hypoechoic |
|
|
|
|
|
|
|
|
|
|
|
|
Echogenic |
Abscess, Cavity
Utricular Cyst, Ectopic Ureter
After Transurethral Resection
Abscess, Cavity 



















































Anechoic lesions in the prostate may be abscesses when corresponding clinical signs are present, or they may represent cavities in rare instances of urogenital tuberculosis (Fig.12.7). The diagnosis is established by biopsy with culture or histological analysis.
423
12
Prostate, Seminal Vesicles, Testis, Epididymis
Utricular Cyst,
Cyst, Ectopic Ureter
Ectopic Ureter












































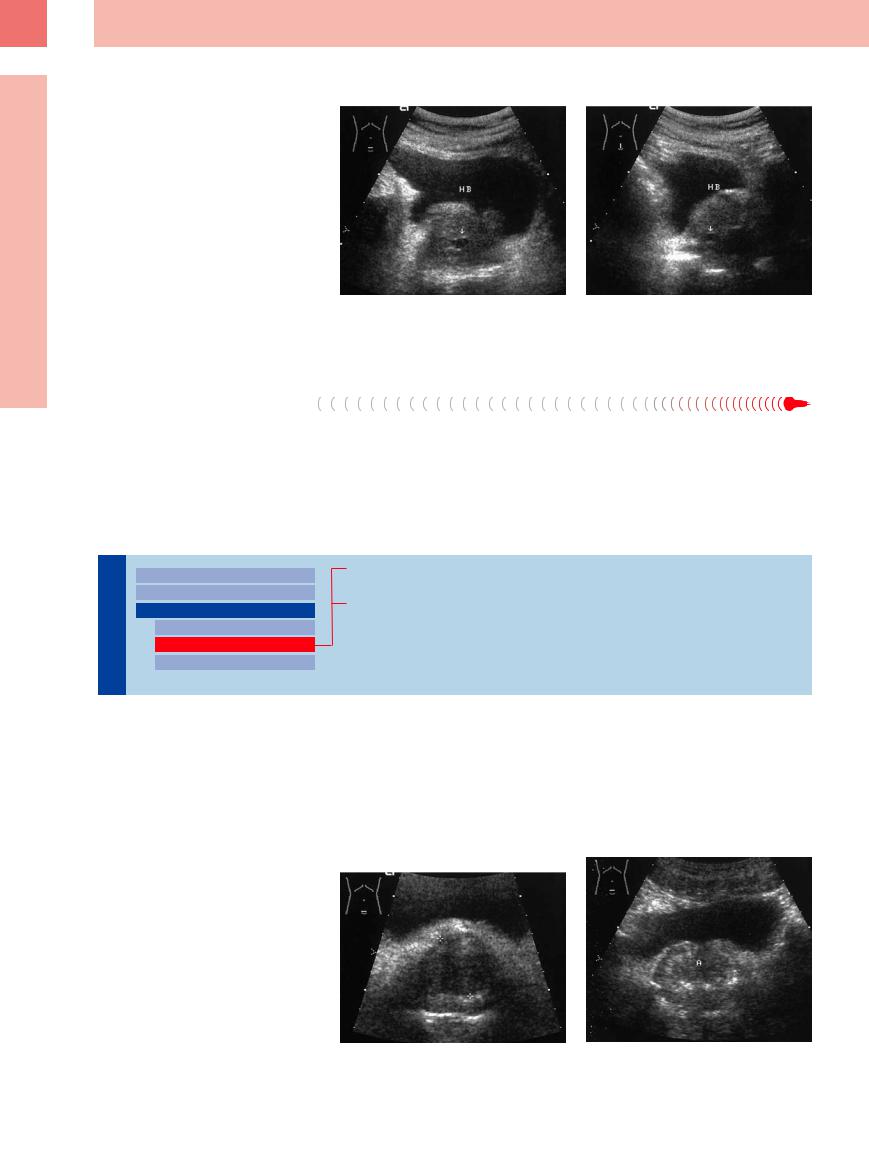
Anechoic areas located in the posteromedian and cranial portion of the prostate (dorsally to the zone of the possible prostatic hyperplasia, the periurethral or transition zone) represent harmless utricular cysts (Fig.12.14). They are considered remnants of the embryonic müllerian duct. Differentiation is required from an ectopic ureter with an anomalous insertion into the wolffian duct.
Fig. 12.14 Cystic mass (arrow) in the lower midline of |
b Lower abdominal longitudinal scan. |
slightly enlarged prostate (P) in a 43-year-old man with |
|
no symptoms. Most likely a utricular cyst. HB = bladder. |
|
a Lower abdominal transverse scan. |
|
After Transurethral Resection
Anechoic areas are also seen following TUR. |
bladder neck with the proximal urethra. A prior |
Irregular, anechoic areas are found at the site |
history of TUR suggests the correct interpreta- |
of the resection cavity, or a funnel-shaped an- |
tion for both of these findings (Fig.12.12). |
echoic area may be found at the junction of the |
|
Hypoechoic
Prostate |
|
|
Enlarged Prostate |
|
|
|
|
||
|
|
|
Small Prostate |
|
|
|
|||
|
|
|
Circumscribed Lesion |
|
|
|
|
||
The |
|
|
|
Anechoic |
|
|
|
Hypoechoic |
|
|
|
|
|
|
|
|
|
|
Echogenic |
Benign Prostatic Hyperplasia
Prostatic Carcinoma
Prostatic hyperplasia and prostatic carcinoma |
investigation. The location of the lesion (see |
typically appear sonographically as circum- |
above) is the only helpful sonographic sign |
scribed hypoechoic lesions that are difficult to |
for benign/malignant differentiation. Clinical |
distinguish from each other by their ultrasound |
findings (DRE, PSA) and transrectal/transure- |
features. Every hypoechoic lesion is therefore |
thral sonography can advance the diagnosis. |
suspicious for carcinoma and warrants further |
|
Benign Prostatic Hyperplasia
Hyperplasia












































A hypoechoic area in the median lobe of the prostate is suggestive of hyperplasia (Fig. 12.15). Hypoechoic areas can also appear as a peripheral rim that contrasts with the more echogenic compressed tissues, forming a “surgical capsule” (Fig.12.16).
Fig. 12.15 Hypoechoic median lobe adenoma (hyperplasia; cursors), clearly demarcated from the rest of the prostate. HB = bladder.
Fig. 12.16 Hyperplastic median lobe (A), delineated by high-level echoes from the hypoechoic displaced prostatic tissue. HB = bladder.
424
Prostatic Carcinoma
Carcinoma







Prostate cancer is a disease of older men with a rapidly increasing incidence at over 50 years of age and with each decade thereafter. Prostate cancer is rarely seen in men less than 50 years of age. A screening program before this age therefore does not seem useful. The age group between 55 and 69 years may profit from a reduced mortality through a screening program with DRE and PSA.
Other conditions present as familiar (genetic) carcinoma. The relative risk is 4.43-fold higher in sons whose father got sick by prostatic carcinoma before the age of 65. This group should be checked from the age of 45.
The early stage of prostatic carcinoma usually appears sonographically as a focal hypoechoic mass (Figs. 12.17, 12.18, 12.19).7 Irregular isoechoic structures can also occur, depending on the tumor histology and extent and any preexisting changes that are incorporated into the tumor. Tumors smaller than 5 mm are not detected by transabdominal or transrectal sonography. Differentiation from BPH with hypoechoic fibromuscular nodules and from focal lesions in prostatitis is almost impossible, with the result that carcinoma usually cannot be detected by ultrasound screening. Generally, then, the role of ultrasonography is limited
to defining tumor extent and detecting lymph node involvement in the lesser pelvis and along the iliac chain (Fig.12.18, Fig.12.19).3
The results of TRUS as a diagnostic procedure are limited because of its inadequate sensitivity and specificity (60–92% and 49–79% respectively).8 Therefore, TRUS is relegated to a role in the diagnostic work-up of an abnormal screening test like a biopsy procedure (10–12 biopsies) and staging. MRI seems to be the best imaging procedure. It can depict the prostate with its zonal anatomy, the surrounding tissue, and lymphatic vessel drainage.
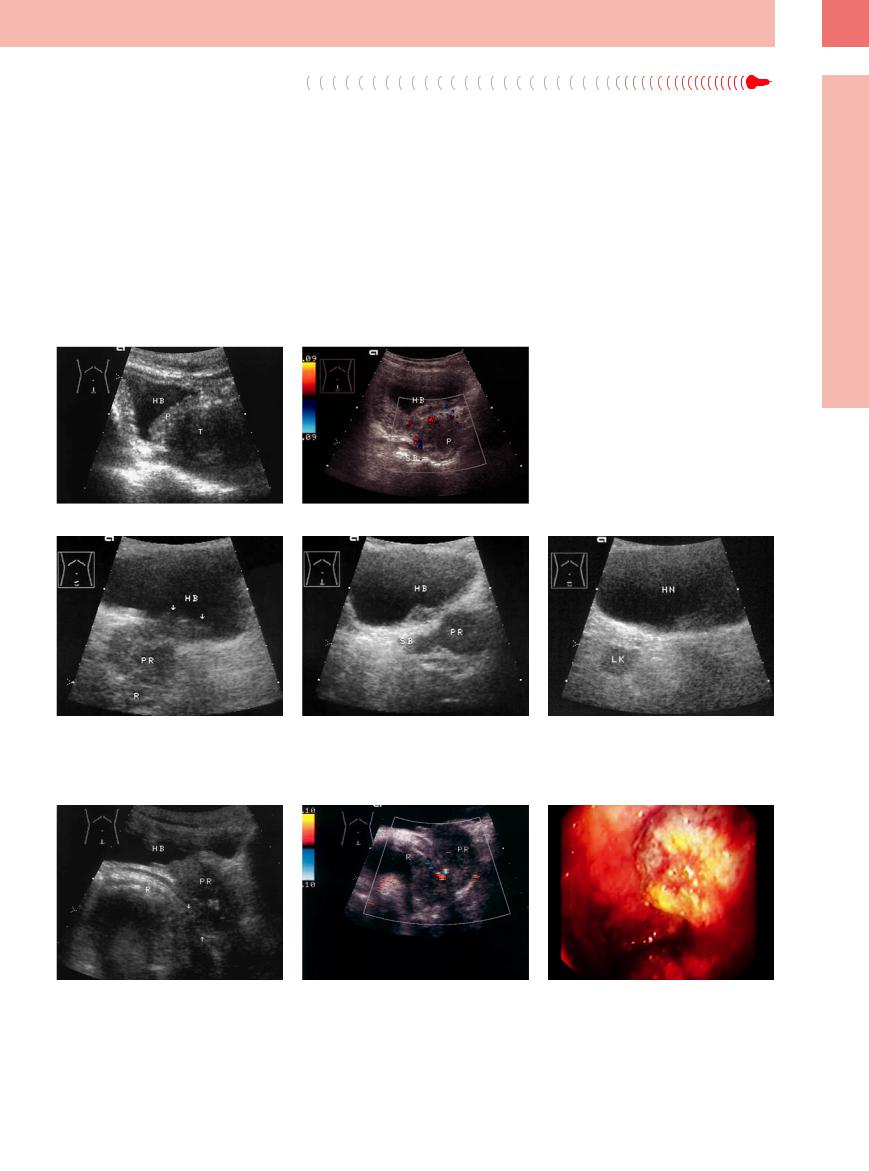
Fig. 12.17 Prostatic carcinoma.
a Ill-defined hypoechoic mass (T) inferior to the normal prostate (P). Sonographically, probably infiltrated into the seminal vesicle.
b Color Doppler view. Hypoechoic mass (P); sedimentation on the floor of the bladder (HB). SB= seminal vesicle.
Fig. 12.18 Hypoechoic prostatic carcinoma (PR), locally |
b Infiltration of the seminal vesicles (SB). |
c Locoregional lymph node (LK). All the changes re- |
advanced. |
|
gressed in response to treatment. HN = bladder. |
a Infiltration of the bladder floor (HB, arrows) and rec- |
|
|
tum (R). |
|
|
Fig. 12.19 Prostatic carcinoma infiltrating the rectum. HB |
b Color duplex image of a: scattered aberrant tumor |
c Endoscopy: intestinal bleeding. |
= bladder; PR = prostate; R = rectum. |
vessels. |
|
a Sonography: ill-defined posteroinferior margin and a |
|
|
thickened, infiltrated rectal wall (R; arrows). |
|
|
12
Circumscribed Lesion
425