

- •Contents
- •Preface
- •Contributors
- •1 Vessels
- •1.1 Aorta, Vena Cava, and Peripheral Vessels
- •Aorta, Arteries
- •Anomalies and Variant Positions
- •Dilatation
- •Stenosis
- •Wall Thickening
- •Intraluminal Mass
- •Perivascular Mass
- •Vena Cava, Veins
- •Anomalies
- •Dilatation
- •Intraluminal Mass
- •Compression, Infiltration
- •1.2 Portal Vein and Its Tributaries
- •Enlarged Lumen Diameter
- •Portal Hypertension
- •Intraluminal Mass
- •Thrombosis
- •Tumor
- •2 Liver
- •Enlarged Liver
- •Small Liver
- •Homogeneous Hypoechoic Texture
- •Homogeneous Hyperechoic Texture
- •Regionally Inhomogeneous Texture
- •Diffuse Inhomogeneous Texture
- •Anechoic Masses
- •Hypoechoic Masses
- •Isoechoic Masses
- •Hyperechoic Masses
- •Echogenic Masses
- •Irregular Masses
- •Differential Diagnosis of Focal Lesions
- •Diagnostic Methods
- •Suspected Diagnosis
- •3 Biliary Tree and Gallbladder
- •3.1 Biliary Tree
- •Thickening of the Bile Duct Wall
- •Localized and Diffuse
- •Bile Duct Rarefaction
- •Localized and Diffuse
- •Bile Duct Dilatation and Intraductal Pressure
- •Intrahepatic
- •Hilar and Prepancreatic
- •Intrapancreatic
- •Papillary
- •Abnormal Intraluminal Bile Duct Findings
- •Foreign Body
- •The Seven Most Important Questions
- •3.2 Gallbladder
- •Changes in Size
- •Large Gallbladder
- •Small/Missing Gallbladder
- •Wall Changes
- •General Hypoechogenicity
- •General Hyperechogenicity
- •General Tumor
- •Focal Tumor
- •Intraluminal Changes
- •Hyperechoic
- •Hypoechoic
- •Nonvisualized Gallbladder
- •Missing Gallbladder
- •Obscured Gallbladder
- •4 Pancreas
- •Diffuse Pancreatic Change
- •Large Pancreas
- •Small Pancreas
- •Hypoechoic Texture
- •Hyperechoic Texture
- •Focal Changes
- •Anechoic Lesion
- •Hypoechoic Lesion
- •Isoechoic Lesion
- •Hyperechoic Lesion
- •Irregular (Complex Structured) Lesion
- •Dilatation of the Pancreatic Duct
- •Marginal/Mild Dilatation
- •Marked Dilatation
- •5 Spleen
- •Nonfocal Changes of the Spleen
- •Diffuse Parenchymal Changes
- •Large Spleen
- •Small Spleen
- •Focal Changes of the Spleen
- •Anechoic Mass
- •Hypoechoic Mass
- •Hyperechoic Mass
- •Splenic Calcification
- •6 Lymph Nodes
- •Peripheral Lymph Nodes
- •Head/Neck
- •Extremities (Axilla, Groin)
- •Abdominal Lymph Nodes
- •Porta Hepatis
- •Splenic Hilum
- •Mesentery (Celiac, Upper and Lower Mesenteric Station)
- •Stomach
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •Small/Large Intestine
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •8 Peritoneal Cavity
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Wall Structures
- •Smooth Margin
- •Irregular Margin
- •Intragastric Processes
- •Intraintestinal Processes
- •9 Kidneys
- •Anomalies, Malformations
- •Aplasia, Hypoplasia
- •Cystic Malformation
- •Anomalies of Number, Position, or Rotation
- •Fusion Anomaly
- •Anomalies of the Renal Calices
- •Vascular Anomaly
- •Diffuse Changes
- •Large Kidneys
- •Small Kidneys
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Irregular Structure
- •Circumscribed Changes
- •Anechoic Structure
- •Hypoechoic or Isoechoic Structure
- •Complex Structure
- •Hyperechoic Structure
- •10 Adrenal Glands
- •Enlargement
- •Anechoic Structure
- •Hypoechoic Structure
- •Complex Echo Structure
- •Hyperechoic Structure
- •11 Urinary Tract
- •Malformations
- •Duplication Anomalies
- •Dilatations and Stenoses
- •Dilated Renal Pelvis and Ureter
- •Anechoic
- •Hypoechoic
- •Hypoechoic
- •Hyperechoic
- •Large Bladder
- •Small Bladder
- •Altered Bladder Shape
- •Intracavitary Mass
- •Hypoechoic
- •Hyperechoic
- •Echogenic
- •Wall Changes
- •Diffuse Wall Thickening
- •Circumscribed Wall Thickening
- •Concavities and Convexities
- •12.1 The Prostate
- •Enlarged Prostate
- •Regular
- •Irregular
- •Small Prostate
- •Regular
- •Echogenic
- •Circumscribed Lesion
- •Anechoic
- •Hypoechoic
- •Echogenic
- •12.2 Seminal Vesicles
- •Diffuse Change
- •Hypoechoic
- •Circumscribed Change
- •Anechoic
- •Echogenic
- •Irregular
- •12.3 Testis, Epididymis
- •Diffuse Change
- •Enlargement
- •Decreased Size
- •Circumscribed Lesion
- •Anechoic or Hypoechoic
- •Irregular/Echogenic
- •Epididymal Lesion
- •Anechoic
- •Hypoechoic
- •Intrascrotal Mass
- •Anechoic or Hypoechoic
- •Echogenic
- •13 Female Genital Tract
- •Masses
- •Abnormalities of Size or Shape
- •Uterus
- •Abnormalities of Size or Shape
- •Myometrial Changes
- •Intracavitary Changes
- •Endometrial Changes
- •Fallopian Tubes
- •Hypoechoic Mass
- •Anechoic Cystic Mass
- •Solid Echogenic or Nonhomogeneous Mass
- •14 Thyroid Gland
- •Diffuse Changes
- •Enlarged Thyroid Gland
- •Small Thyroid Gland
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Circumscribed Changes
- •Anechoic
- •Hypoechoic
- •Isoechoic
- •Hyperechoic
- •Irregular
- •Differential Diagnosis of Hyperthyroidism
- •Types of Autonomy
- •15 Pleura and Chest Wall
- •Chest Wall
- •Masses
- •Parietal Pleura
- •Nodular Masses
- •Diffuse Pleural Thickening
- •Pleural Effusion
- •Anechoic Effusion
- •Echogenic Effusion
- •Complex Effusion
- •16 Lung
- •Masses
- •Anechoic Masses
- •Hypoechoic Masses
- •Complex Masses
- •Index
15 Pleura and Chest Wall
Pleura and Chest Wall 511
|
Chest Wall |
513 |
|||||
|
|||||||
|
|
|
|
Masses |
513 |
||
|
|
|
|
||||
|
|
|
|
|
|
Rib and Sternal Fractures |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Rib and Sternal Metastases |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cutaneous Metastases |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Carcinoma of the Chest Wall |
|
|
Parietal Pleura |
518 |
|||||
|
|||||||
|
|
|
Nodular Masses |
518 |
|||
|
|
|
|||||
|
|
|
|
|
|
Metastases |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pleural Plaque |
|
|
|
|
Diffuse Pleural Thickening |
520 |
|||
Pleural Carcinomatosis
Pleural Fibrosis
Diffuse Malignant Mesothelioma
Pleural Effusion |
523 |
||||||
|
|
|
Anechoic Effusion |
525 |
|||
|
|
||||||
|
|
|
|
|
|
Transudative Effusion |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Exudative Effusion |
|
|
|
|
Echogenic Effusion |
526 |
|||
|
|
|
|||||
|
|
|
|
|
|
Benign Effusion |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
Malignant Effusion |
|
|
|
|
Complex Effusion |
528 |
|||
Inflammatory or Malignant Effusion
Fibrothorax
Seropneumothorax,
Pneumothorax

15
Pleura and Chest Wall
the lung parenchyma. Histologically, it consists |
pleural cavity. |
of a single layer of epithelium. The visceral |
At the level of the chest wall, the pleura is |
pleura, which covers the surface of the lung, |
bounded externally by the ribs, sternum, and |
is distinguished from the parietal pleura, which |
intercostal muscles. Overlying these structures |
lines the inner chest wall (thoracic part) and |
is a layer of chest-wall muscle and subcutane- |
covers much of the diaphragm (diaphragmatic |
ous fat (Fig.15.1). |
part). Normally the two pleural layers are ap- |
|
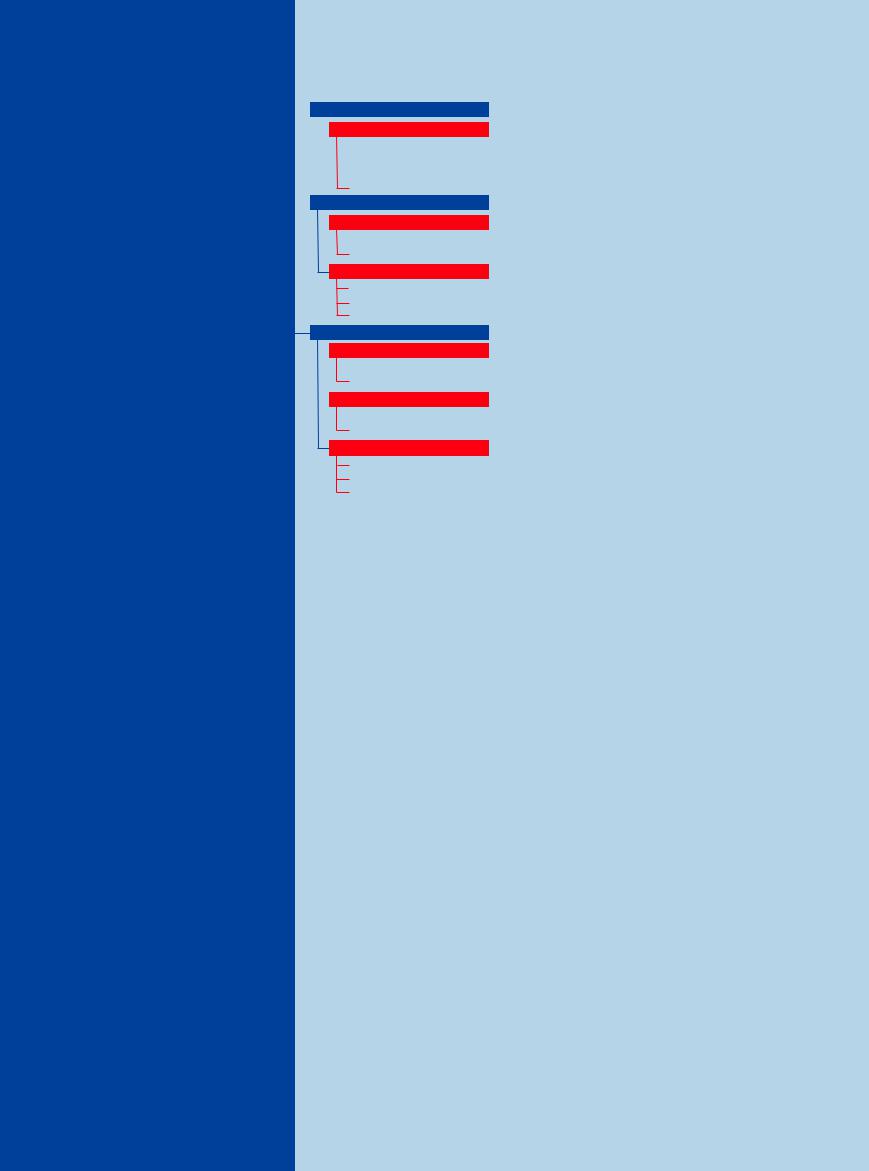
Fig. 15.1 Anatomical relations of the parietal pleura in the lateral chest wall.
a Schematic diagram: (1) skin; (2) subcutaneous fat; (3) chest-wall muscle; (4) intercostal muscles; (5) ribs; (6) parietal pleura; (7) visceral pleura; (8) lung.
Ultrasound Morphology
Morphology
Normal appearance. The bony structures of the chest wall (ribs and sternum) are characterized by a high-level surface echo with almost complete posterior acoustic shadowing ( 15.1a,b). By contrast, the uncalcified costal cartilages allow the complete through-transmission of sound waves (
15.1a,b). By contrast, the uncalcified costal cartilages allow the complete through-transmission of sound waves ( 15.1c). The parietal pleura lines the inner chest wall, while the visceral pleura invests the lung parenchyma.
15.1c). The parietal pleura lines the inner chest wall, while the visceral pleura invests the lung parenchyma.
The pleura normally appears as a bright, well-defined linear echo called the pleural line. The potential space between the pleural layers cannot be visualized with ultrasound. In dynamic real-time sonography during respiration, the visceral part of the pleural echo can be seen gliding in relation to the stationary parietal part ( 15.1 d).
15.1 d).
Positions for scanning. The patient should be examined in a sitting position whenever possible. Generally the ultrasound probe is placed
b Sonographic appearance of the structures. 1 = Subcutaneous fat; 2 = chest-wall muscle; 3 = intercostal muscle; 4 = pleural echo.
intercostally. A subcostal transhepatic and intercostal approach is recommended for subpulmonary and diaphragmatic scanning (Fig.15.2,  15.1e,f). The posterior insertion of the muscular diaphragm (crus) can be defined in the paravertebral region in an upper abdominal transverse scan (
15.1e,f). The posterior insertion of the muscular diaphragm (crus) can be defined in the paravertebral region in an upper abdominal transverse scan ( 15.1 g–i). When fluid accumulates in the pleural cavity and abdomen, ultrasound can clearly define the contractions of the diaphragm that occur with respiration (
15.1 g–i). When fluid accumulates in the pleural cavity and abdomen, ultrasound can clearly define the contractions of the diaphragm that occur with respiration ( 15.1j–l). On deep inspiration, a subcostal scan angled toward the head can show variable degrees of hepatic impression by the diaphragmatic crura, which appear as hyperechoic “pseudotumors” in the liver (
15.1j–l). On deep inspiration, a subcostal scan angled toward the head can show variable degrees of hepatic impression by the diaphragmatic crura, which appear as hyperechoic “pseudotumors” in the liver ( 15.1 m–o).
15.1 m–o).
A complete ultrasound examination of the pleura is not possible because the mediastinal and paravertebral pleura cannot be visualized. Additional blind spots exist in the regions of the scapula and left hemidiaphragm.
Location of the pleura
●Along the inner chest wall (parietal)
●Along the inner surface of the diaphragm (parietal)
●Over the surface of the lung parenchyma (visceral)
Pleural thickness
●Visceral, parietal, and diaphragmatic: 1 mm or less
Histology
●Single layer of epithelial cells lining the thoracic cavity
Ultrasound appearance
●Sharp, bright, linear “entry echo” produced as the sound enters the lung
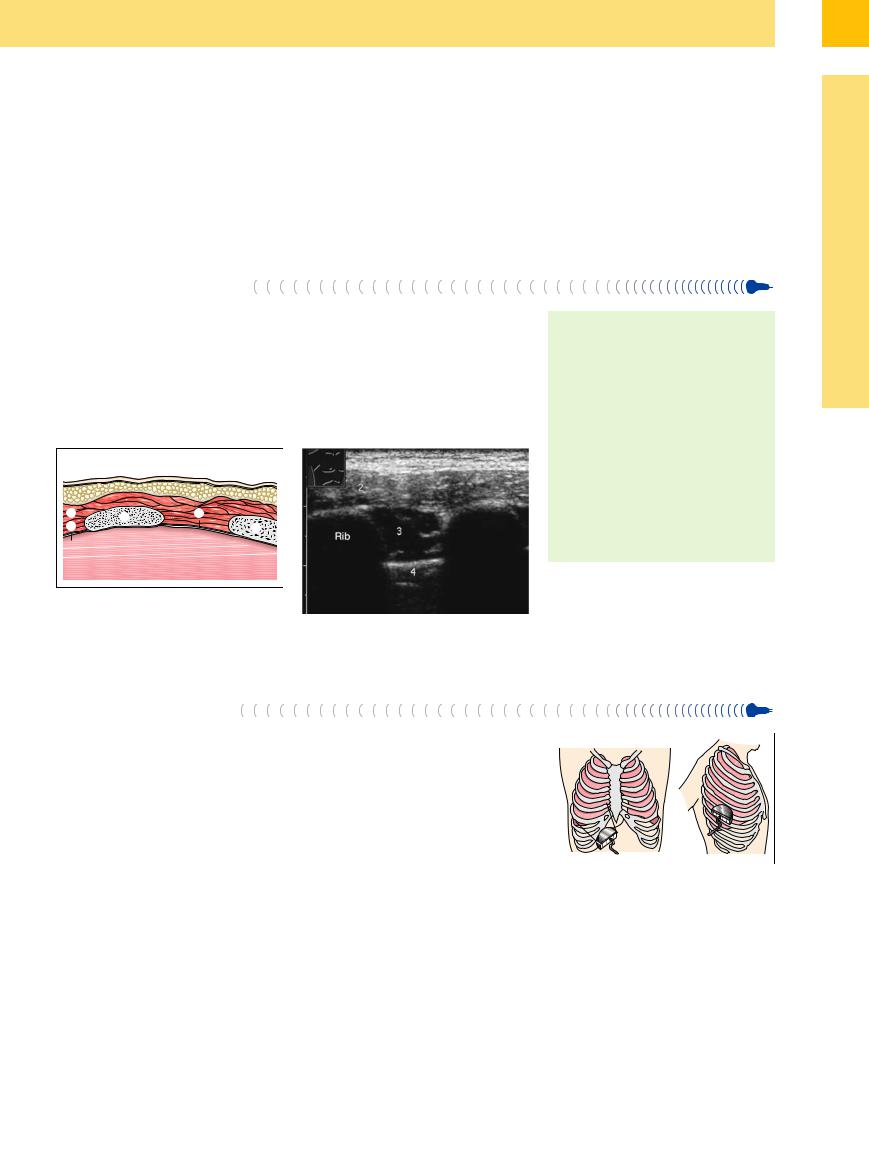
Fig. 15.2 Diagram of transducer placements for thoracic ultrasound. Left: subcostal transhepatic scan for evaluating the lower lung field. Right: intercostal scan parallel to the ribs.
511
15
Pleura and Chest Wall
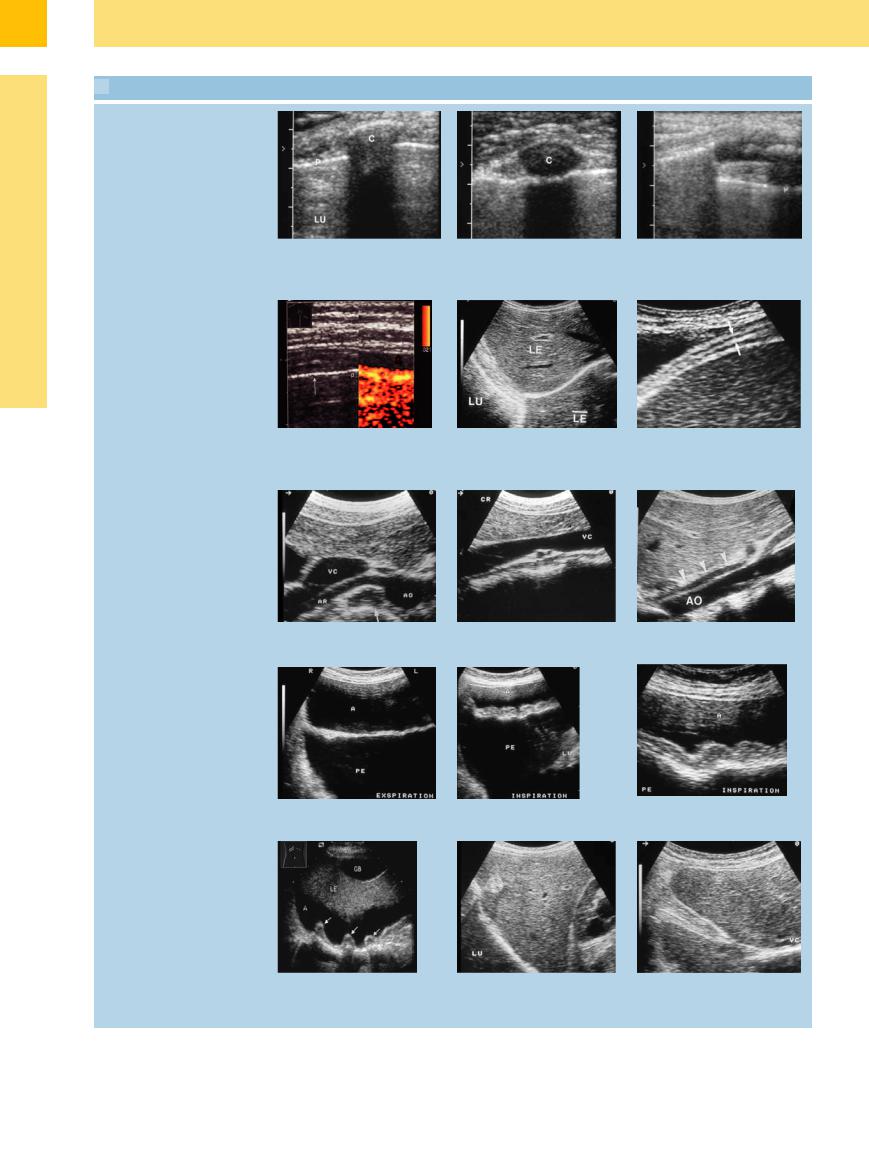
 15.1 Ultrasound Appearance of the Ribs, Pleura, and Diaphragm
15.1 Ultrasound Appearance of the Ribs, Pleura, and Diaphragm
Ribs
a and b Appearance of a bony rib (a) and a cartilaginous rib (b) in transverse section. c Longitudinal section, central cartilage C = rib, LU = lung. shadow. Total shadowing in the bony
part of the rib (left image margin). P = pleura–lung boundary echo.
Pleura–lung boundary line
d Power Doppler scan color-encodes the respiratory movements of the lung (right). P = pleura.
Muscular diaphragm
e The pleural lines in subcostal scans through the liver (L). Reflections from the pleura produce a mirror image artifact (LE). LU = lung.
f E usion outlines the diaphragm (arrows) in an intercostal scan on the right side.
g–i Posterior insertion of the muscular diaphragm (arrows) in upper abdominal transverse scans (g) and upper abdominal longitudinal scans (h and l). AO = aorta; VC = vena cava; AR = renal artery; SC = spinal column.
Diaphragm, respiratory position changes
j–l Subcostal scans in the presence of ascites (A) and pleural e usion (PE). The survey scans (j and k) show relaxation of the diaphragm with expiration and contraction with inspiration. LU = lung.
Diaphragmatic crura
m When ascites is present (A), the diaphragmatic crura are clearly visualized along the anterior chest wall. GB = gallbladder; LE = liver.
n The diaphragmatic crura occasionally appear as pseudotumors. LU = lung.
o The diaphragmatic crura may deeply indent the liver tissue in the subcostal scan.
512