

- •Contents
- •Preface
- •Contributors
- •1 Vessels
- •1.1 Aorta, Vena Cava, and Peripheral Vessels
- •Aorta, Arteries
- •Anomalies and Variant Positions
- •Dilatation
- •Stenosis
- •Wall Thickening
- •Intraluminal Mass
- •Perivascular Mass
- •Vena Cava, Veins
- •Anomalies
- •Dilatation
- •Intraluminal Mass
- •Compression, Infiltration
- •1.2 Portal Vein and Its Tributaries
- •Enlarged Lumen Diameter
- •Portal Hypertension
- •Intraluminal Mass
- •Thrombosis
- •Tumor
- •2 Liver
- •Enlarged Liver
- •Small Liver
- •Homogeneous Hypoechoic Texture
- •Homogeneous Hyperechoic Texture
- •Regionally Inhomogeneous Texture
- •Diffuse Inhomogeneous Texture
- •Anechoic Masses
- •Hypoechoic Masses
- •Isoechoic Masses
- •Hyperechoic Masses
- •Echogenic Masses
- •Irregular Masses
- •Differential Diagnosis of Focal Lesions
- •Diagnostic Methods
- •Suspected Diagnosis
- •3 Biliary Tree and Gallbladder
- •3.1 Biliary Tree
- •Thickening of the Bile Duct Wall
- •Localized and Diffuse
- •Bile Duct Rarefaction
- •Localized and Diffuse
- •Bile Duct Dilatation and Intraductal Pressure
- •Intrahepatic
- •Hilar and Prepancreatic
- •Intrapancreatic
- •Papillary
- •Abnormal Intraluminal Bile Duct Findings
- •Foreign Body
- •The Seven Most Important Questions
- •3.2 Gallbladder
- •Changes in Size
- •Large Gallbladder
- •Small/Missing Gallbladder
- •Wall Changes
- •General Hypoechogenicity
- •General Hyperechogenicity
- •General Tumor
- •Focal Tumor
- •Intraluminal Changes
- •Hyperechoic
- •Hypoechoic
- •Nonvisualized Gallbladder
- •Missing Gallbladder
- •Obscured Gallbladder
- •4 Pancreas
- •Diffuse Pancreatic Change
- •Large Pancreas
- •Small Pancreas
- •Hypoechoic Texture
- •Hyperechoic Texture
- •Focal Changes
- •Anechoic Lesion
- •Hypoechoic Lesion
- •Isoechoic Lesion
- •Hyperechoic Lesion
- •Irregular (Complex Structured) Lesion
- •Dilatation of the Pancreatic Duct
- •Marginal/Mild Dilatation
- •Marked Dilatation
- •5 Spleen
- •Nonfocal Changes of the Spleen
- •Diffuse Parenchymal Changes
- •Large Spleen
- •Small Spleen
- •Focal Changes of the Spleen
- •Anechoic Mass
- •Hypoechoic Mass
- •Hyperechoic Mass
- •Splenic Calcification
- •6 Lymph Nodes
- •Peripheral Lymph Nodes
- •Head/Neck
- •Extremities (Axilla, Groin)
- •Abdominal Lymph Nodes
- •Porta Hepatis
- •Splenic Hilum
- •Mesentery (Celiac, Upper and Lower Mesenteric Station)
- •Stomach
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •Small/Large Intestine
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •8 Peritoneal Cavity
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Wall Structures
- •Smooth Margin
- •Irregular Margin
- •Intragastric Processes
- •Intraintestinal Processes
- •9 Kidneys
- •Anomalies, Malformations
- •Aplasia, Hypoplasia
- •Cystic Malformation
- •Anomalies of Number, Position, or Rotation
- •Fusion Anomaly
- •Anomalies of the Renal Calices
- •Vascular Anomaly
- •Diffuse Changes
- •Large Kidneys
- •Small Kidneys
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Irregular Structure
- •Circumscribed Changes
- •Anechoic Structure
- •Hypoechoic or Isoechoic Structure
- •Complex Structure
- •Hyperechoic Structure
- •10 Adrenal Glands
- •Enlargement
- •Anechoic Structure
- •Hypoechoic Structure
- •Complex Echo Structure
- •Hyperechoic Structure
- •11 Urinary Tract
- •Malformations
- •Duplication Anomalies
- •Dilatations and Stenoses
- •Dilated Renal Pelvis and Ureter
- •Anechoic
- •Hypoechoic
- •Hypoechoic
- •Hyperechoic
- •Large Bladder
- •Small Bladder
- •Altered Bladder Shape
- •Intracavitary Mass
- •Hypoechoic
- •Hyperechoic
- •Echogenic
- •Wall Changes
- •Diffuse Wall Thickening
- •Circumscribed Wall Thickening
- •Concavities and Convexities
- •12.1 The Prostate
- •Enlarged Prostate
- •Regular
- •Irregular
- •Small Prostate
- •Regular
- •Echogenic
- •Circumscribed Lesion
- •Anechoic
- •Hypoechoic
- •Echogenic
- •12.2 Seminal Vesicles
- •Diffuse Change
- •Hypoechoic
- •Circumscribed Change
- •Anechoic
- •Echogenic
- •Irregular
- •12.3 Testis, Epididymis
- •Diffuse Change
- •Enlargement
- •Decreased Size
- •Circumscribed Lesion
- •Anechoic or Hypoechoic
- •Irregular/Echogenic
- •Epididymal Lesion
- •Anechoic
- •Hypoechoic
- •Intrascrotal Mass
- •Anechoic or Hypoechoic
- •Echogenic
- •13 Female Genital Tract
- •Masses
- •Abnormalities of Size or Shape
- •Uterus
- •Abnormalities of Size or Shape
- •Myometrial Changes
- •Intracavitary Changes
- •Endometrial Changes
- •Fallopian Tubes
- •Hypoechoic Mass
- •Anechoic Cystic Mass
- •Solid Echogenic or Nonhomogeneous Mass
- •14 Thyroid Gland
- •Diffuse Changes
- •Enlarged Thyroid Gland
- •Small Thyroid Gland
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Circumscribed Changes
- •Anechoic
- •Hypoechoic
- •Isoechoic
- •Hyperechoic
- •Irregular
- •Differential Diagnosis of Hyperthyroidism
- •Types of Autonomy
- •15 Pleura and Chest Wall
- •Chest Wall
- •Masses
- •Parietal Pleura
- •Nodular Masses
- •Diffuse Pleural Thickening
- •Pleural Effusion
- •Anechoic Effusion
- •Echogenic Effusion
- •Complex Effusion
- •16 Lung
- •Masses
- •Anechoic Masses
- •Hypoechoic Masses
- •Complex Masses
- •Index
2
Liver
Small Liver
|
|
|
Diffuse Changes in Hepatic |
|
|
Atrophy |
|
|
|
|
|
|
|||||
|
|
|
Parenchyma |
|
|
Cirrhosis |
|
|
Liver |
|
Enlarged Liver |
|
|
|
|||
|
|
|
Resection |
|
||||
|
|
|
|
|
|
|
||
|
|
|
|
Small Liver |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Homogeneous Hypoechoic Texture |
|
|
|
|
|
|
|
|
Homogeneous Hyperechoic Texture |
|
|
|
|
|
|
|
|
Regionally Inhomogeneous |
|
|
|
|
|
|
|
|
Texture |
|
|
|
|
|
|
|
|
Diffuse Inhomogeneous Texture |
|
|
|
|
|
|
|
Localized Changes in Hepatic |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
Parenchyma |
|
|
|
|
|
|
|
|
Differential Diagnosis of Focal Lesions |
|
|
|
|
|
|
|
|
|
|
|
|
||
A small liver is a rather infrequent finding and |
|
|
|
|
||||
becomes evident only if the decrease in size is |
|
|
|
|
||||
substantial. Owing to the small probe contact |
|
|
|
|
||||
area and the hidden position below the ribs, |
|
|
|
|
||||
the conditions for ultrasound studies of the |
|
|
|
|
||||
liver are less than ideal. |
|
|
|
|
||||
Atrophy |
|
|
|
|
||||
Hepatic atrophy is a rather rare finding and |
|
|
|
|
||||
may pertain to the entire organ or just individ- |
|
|
|
|
||||
ual segments. Its possible causes include vas- |
|
|
|
|
||||
cular disorders or chronic inflammatory dis- |
|
|
|
|
||||
ease, the most common being chronic atrophic |
|
|
|
|
||||
cirrhosis. |
|
|
|
|
|
|
||
Cirrhosis |
|
|
|
|
||||
Apart from the decrease in size, the cirrhotic |
and thus can still be insonated well despite its |
gal flow (Fig. 2.29). The hepatic artery proper |
||||||
liver is characterized by certain typical criteria |
lack of size (Fig. 2.27, Fig. 2.28). Also, there are |
correspondingly shows an increased flow in |
||||||
(Table 2.9). Quite often there is a substantial |
clear-cut signs of portal hypertension, with a |
these situations. |
||||||
amount of ascites, in which the small organ |
drop in flow velocity within the portal vein, or |
|
||||||
seems to float like a wooden block in water |
even no flow at all, and sometimes a hepatofu- |
|
||||||
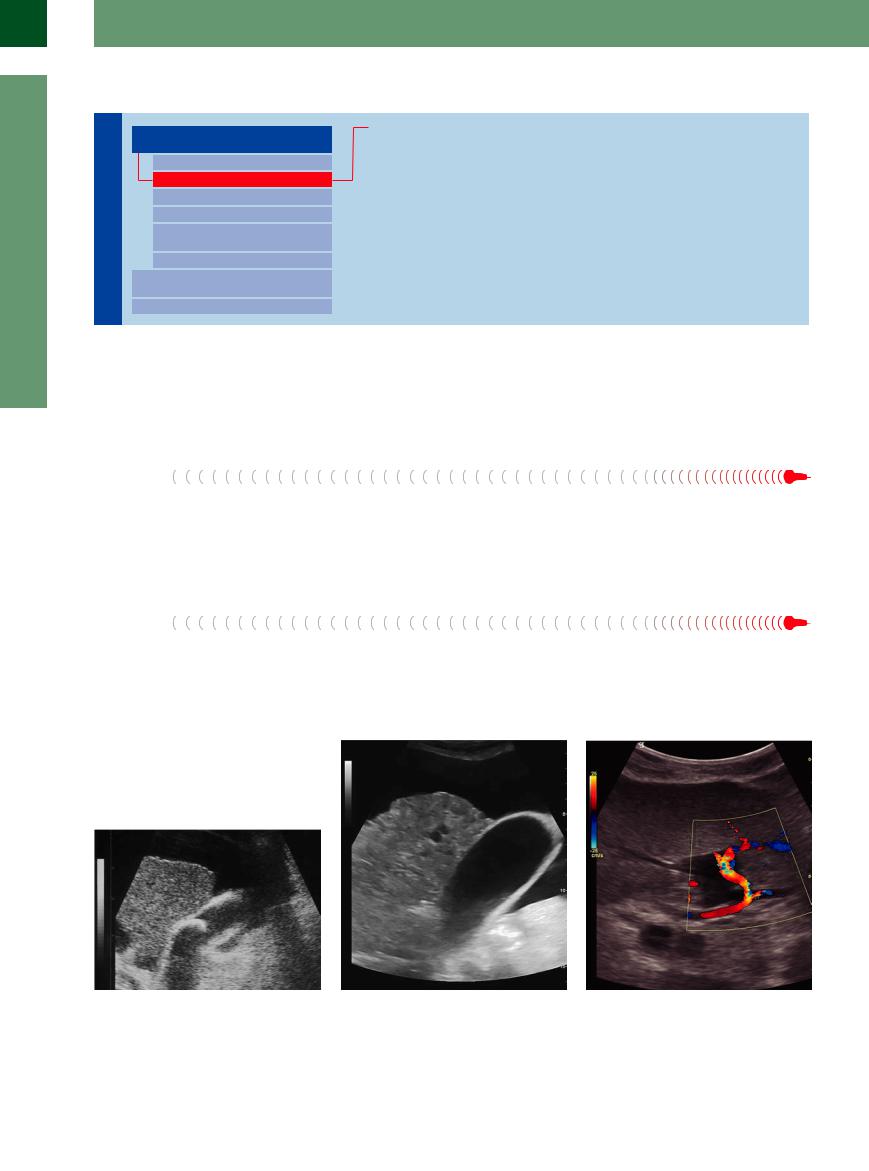
Fig. 2.27 Atrophic cirrhosis. Grainy, slightly inhomogeneous hepatic parenchyma, irregular surface, rarefied vasculature; the liver floats like a wooden block in the ascites. Ancillary finding: thickened gallbladder wall, gallstone evident within the lumen of the gallbladder.
Fig. 2.28 Completely atrophic cirrhosis of the liver with irregular surface, rarefied intrahepatic vasculature, and marked ascites. Ancillary finding: thickened gallbladder wall.
Fig. 2.29 Normally, the blood supply is 70–75% by the portal vein, and 25–30% by the liver artery.4 In cirrhotic liver, the artery compensates for the reduced blood flow caused by portal hypertension and increases in diameter (color Doppler). The reduction of the portal flow results in a zero blood flow or flow reversal.
76
Table 2.9 Diagnostic criteria in cirrhosis of the liver |
|
|
|
Criterion |
Fatty cirrhosis |
Posthepatitic cirrhosis |
Cardiac cirrhosis |
Size |
+++ |
Normal–smaller |
Normal |
Shape |
Rounded |
Beak-like |
– |
Surface |
Comparatively smooth |
Irregular |
Smooth |
Contour of margin |
Blunt/rounded |
Sharply angulated |
Sharply angulated/blunt |
Parenchymal structure |
Dense, homogeneous |
Coarse, inhomogeneous |
Coarse, inhomogeneous |
Conduction |
Attenuated |
Normal |
Increased |
Hepatic veins |
Narrow, blurred, beginning rarefaction |
Marked rarefaction |
Engorged |
Portal veins |
Center: engorged; periphery: caliber change |
Center: engorged; periphery: caliber change |
Engorged |
Hepatic artery |
No characteristic change |
Prominent due to compensation |
No characteristic change |
Respiratory motion |
Normal |
Normal |
Normal |
Consistency |
Firm |
Hard |
Hard |
Tenderness |
Possible |
No |
In acute decompensation |
Resection 






















































Usually, the status of any parts of the liver after |
the change in vascular architecture, but one has |
the remaining liver with tilting, rotation, and |
resection is hard to recognize just by looking at |
to remember that the numerous normal var- |
twisting around the portal axis. Apart from the |
the size of the organ since the liver has an |
iants of the vascular system and the congeni- |
usual small contact area at the right thoracic |
enormous capacity for regeneration, and any |
tally different sizes of the various liver seg- |
wall, these factors will hamper orientation in |
surgical reduction in volume will be compen- |
ments (smaller left lobe) may make this an |
the right upper abdomen. |
sated for by hypertrophy of the remaining tis- |
impossibility. Quite often, right hemihepatec- |
|
sue. A postresection liver is best assessed by |
tomy will produce an anomalous position of |
|
Homogeneous Hypoechoic Texture
Liver

Diffuse Changes in Hepatic
Parenchyma
Enlarged Liver
Small Liver
Homogeneous Hypoechoic Texture
Homogeneous Hyperechoic Texture
Regionally Inhomogeneous
Texture
Diffuse Inhomogeneous Texture
Localized Changes in Hepatic
Parenchyma
Differential Diagnosis of Focal Lesions
Acute Liver Congestion
Amyloidosis
Acute Hepatitis
A hypoechoic homogeneous echotexture within the liver is due to a decrease in the number of echoes per unit area because of fluid accumulation on the intracellular level (edema), or the extracellular/intracellular/sinusoidal level (hypervolemia, congestion), or both (right-sided heart failure, renal failure, hemodialysis).
2
Diffuse Changes in Hepatic Parenchyma
77
2
Liver
Acute Liver Congestion





Congestion of the inferior vena cava will increase the volume load of the liver (edema) and explains the lessened echogenicity but heightened conduction of the organ; on the other hand, such typical criteria as the significant capsular tension with its concomitant pain and the tightly elastic/firm consistency of the
liver on palpation with marked tenderness will be hard to miss. The hypoechoic coarse parenchyma may be quite discreet and become masked by previous chronic congestion of the liver aggravated by acute right ventricular failure; however, sonographic findings of improved ultrasound conduction of the organ,
engorged hepatic veins easily followed far into the periphery, and a dilated junction of the hepatic veins remain the characteristic sonographic signs of an acutely congested liver (Figs. 2.17, 2.18, 2.19).
Amyloidosis 





















































Amyloidosis is characterized by a homogeneous increase in the size of the liver, with regular architecture and a homogeneous hypoechoic parenchyma of coarse consistency.
Acute Hepatitis 



















































Since acute hepatitis is accompanied by edema and the infiltration of inflammatory cells, one would expect a hypoechoic organ that is easy to insonate; unfortunately, a liver such as this is rarely encountered in acute viral hepatitis. Ultrasonography is therefore not the modality of choice in the work-up of acute hepatitis, especially since there are far more characteristic findings suggesting the diagnosis of acute viral
hepatitis: even if shape, size, and echotexture of the liver appear absolutely normal, quite often an increasing resemblance of the parenchymal splenic and hepatic echotextures (possibly with homogeneous enlargement) becomes evident (Fig. 2.30, Fig. 2.31). A thickened striated gallbladder wall of up to 20 mm (no tenderness!) and hypoechoic, pathologically enlarged hilar lymph nodes can also frequently
be demonstrated (Fig. 2.32, Fig. 2.33). Parenchymal hypoechogenicity in acute viral hepatitis is an incidental finding in fulminating necrosis of the liver; in this case, the organ is surprisingly small, displays a markedly soft consistency, and is characterized by a hypoechoic to splotchy/inhomogeneous parenchymal echotexture.
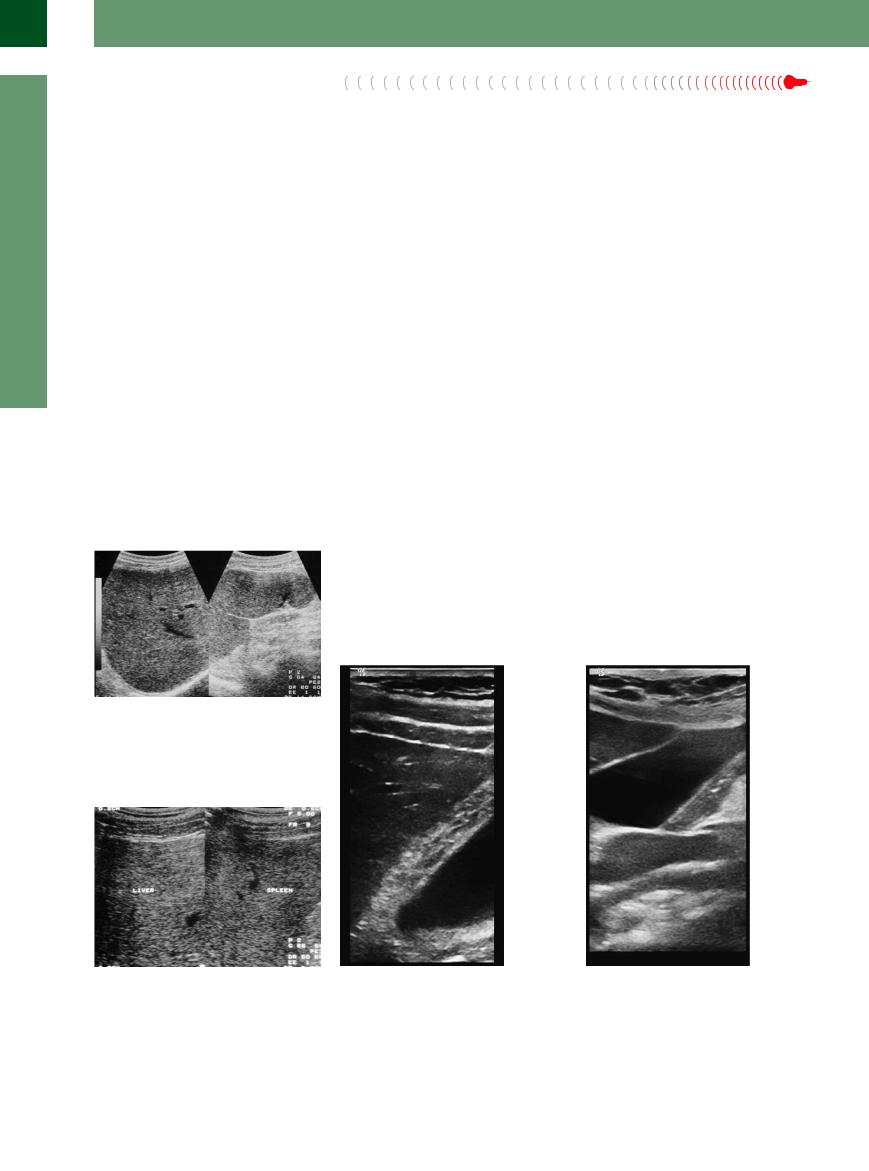
Fig. 2.30 Acute hepatitis in mononucleosis. Compare spleen/liver: in acute hepatitis the parenchymal texture of the liver and spleen may start to resemble each other.
Fig. 2.31 Acute hepatitis. Compare spleen/liver: in this case of acute viral hepatitis the hepatic and splenic parenchyma begin to resemble each other. This is a case of acute hepatitis A infection.
Fig. 2.32 Gallbladder in a case of acute hepatitis B. Marked thickening and striation of the wall > 20 mm without any tenderness. The parenchyma itself and the ultrasound conductivity of the liver are normal.
Fig. 2.33 Lymph node in acute hepatitis in the liver hilum. Normal gallbladder wall. Hypoechoic enlarged lymph node in the hepatoduodenal ligament as a sign for viral or autoimmune hepatitis. Normal parenchyma and US properties.
78
Homogeneous Hyperechoic Texture
Liver

Diffuse Changes in Hepatic
Parenchyma
Enlarged Liver
Small Liver
Homogeneous Hypoechoic Texture
Homogeneous Hyperechoic Texture
Regionally Inhomogeneous
Texture
Diffuse Inhomogeneous Texture
Localized Changes in Hepatic
Parenchyma
Differential Diagnosis of Focal Lesions
Fatty Liver
Hemochromatosis
Fibrosis
A hyperechoic homogeneous texture of the liver may be the result of an increased number of echoes/boundaries per unit area, which in turn may be traced back to intracellular or interstitial deposits of foreign substances (e. g., fat or iron, and fibrosis, respectively).
Fatty Liver












In principle, fatty tissue lends itself quite well to insonation: it is characterized by a low density and impedance and conducts ultrasound better than water or hepatic parenchyma. It is the increase in the number of boundaries that is responsible for the typical hyperechogenicity and attenuation encountered in fatty liver. The
severity of the steatosis, the type of fatty deposits within the hepatocytes (large vesicles = few additional boundaries; small vesicles = numerous additional boundaries), the type of fat, and other factors (severity of any concomitant inflammation or fibrosis) predetermine the change in the echotexture, i. e., the number,
size, and density of the individual echoes and the degree of attenuation. But one aspect remains constant: even if the overall echotexture varies between segments or regions, within any such affected area the individual echoes still exhibit the homogeneous appearance (
2.6).
Hemochromatosis


















































Although iron deposits in the hepatocytes re- |
nonspecific, making ultrasonography an un- |
tion of the hepatic parenchyma will then char- |
sult in a homogeneous increase in the echoge- |
suitable modality in early diagnosis. Only in- |
acterize the disease (Fig. 2.26). |
nicity as well as attenuation, this finding is |
flammatory changes and cirrhotic transforma- |
|
Fibrosis
Fibrosis of the liver may be a primary hepatic |
ity of the liver, demonstration of a slightly un- |
disorder, a sequela to a previously overcome |
dulating surface, firm consistency, and quite |
bout of hepatitis, or a chronic vascular disease. |
often a still evident vascular and hepatic archi- |
Typical ultrasound findings are the homogene- |
tecture (Fig. 2.34). |
ous, if somewhat coarsely grained, echogenic- |
|
2
Diffuse Changes in Hepatic Parenchyma
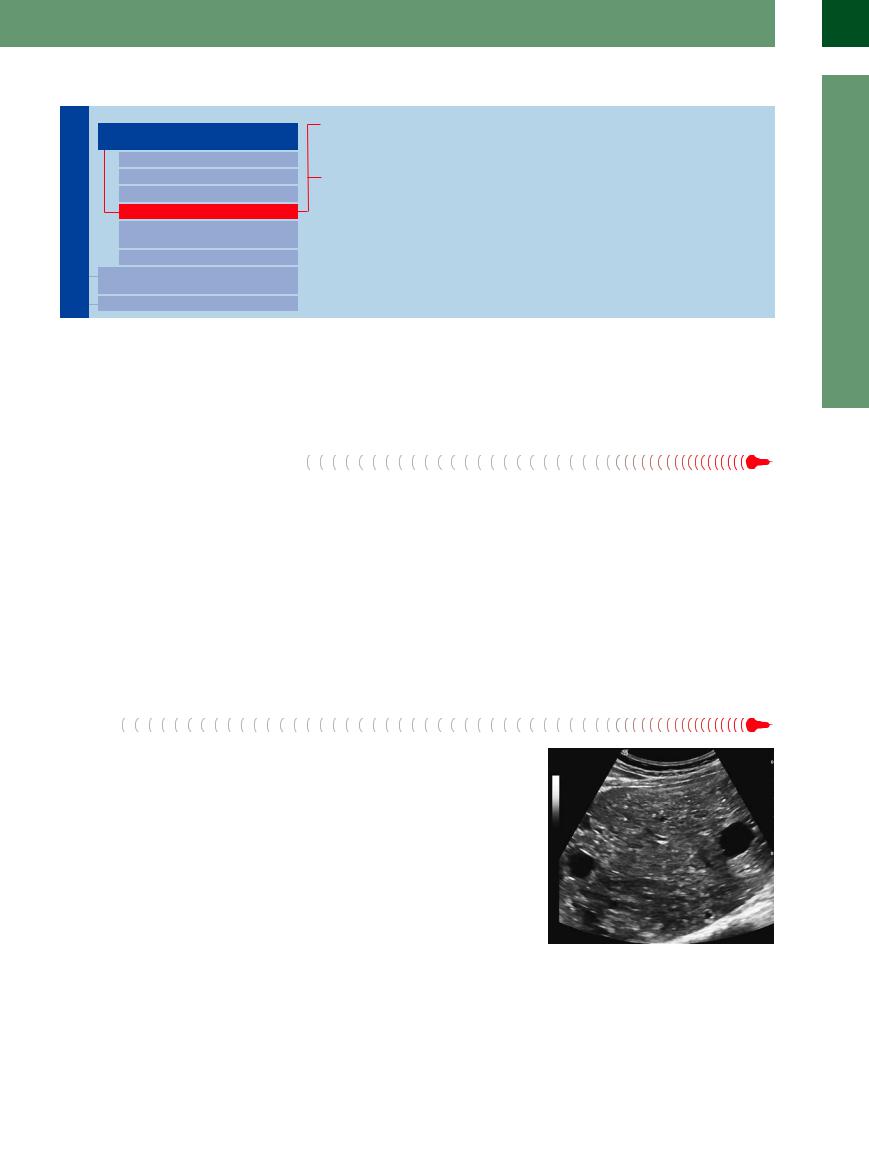
Fig. 2.34 Fibrosis; in this case, Caroli syndrome with slightly inhomogeneous, coarsely grained, hyperechoic hepatic parenchyma; demonstration of a small cyst, still present hepatic vein taking a mildly arced course.
79