

- •Contents
- •Preface
- •Contributors
- •1 Vessels
- •1.1 Aorta, Vena Cava, and Peripheral Vessels
- •Aorta, Arteries
- •Anomalies and Variant Positions
- •Dilatation
- •Stenosis
- •Wall Thickening
- •Intraluminal Mass
- •Perivascular Mass
- •Vena Cava, Veins
- •Anomalies
- •Dilatation
- •Intraluminal Mass
- •Compression, Infiltration
- •1.2 Portal Vein and Its Tributaries
- •Enlarged Lumen Diameter
- •Portal Hypertension
- •Intraluminal Mass
- •Thrombosis
- •Tumor
- •2 Liver
- •Enlarged Liver
- •Small Liver
- •Homogeneous Hypoechoic Texture
- •Homogeneous Hyperechoic Texture
- •Regionally Inhomogeneous Texture
- •Diffuse Inhomogeneous Texture
- •Anechoic Masses
- •Hypoechoic Masses
- •Isoechoic Masses
- •Hyperechoic Masses
- •Echogenic Masses
- •Irregular Masses
- •Differential Diagnosis of Focal Lesions
- •Diagnostic Methods
- •Suspected Diagnosis
- •3 Biliary Tree and Gallbladder
- •3.1 Biliary Tree
- •Thickening of the Bile Duct Wall
- •Localized and Diffuse
- •Bile Duct Rarefaction
- •Localized and Diffuse
- •Bile Duct Dilatation and Intraductal Pressure
- •Intrahepatic
- •Hilar and Prepancreatic
- •Intrapancreatic
- •Papillary
- •Abnormal Intraluminal Bile Duct Findings
- •Foreign Body
- •The Seven Most Important Questions
- •3.2 Gallbladder
- •Changes in Size
- •Large Gallbladder
- •Small/Missing Gallbladder
- •Wall Changes
- •General Hypoechogenicity
- •General Hyperechogenicity
- •General Tumor
- •Focal Tumor
- •Intraluminal Changes
- •Hyperechoic
- •Hypoechoic
- •Nonvisualized Gallbladder
- •Missing Gallbladder
- •Obscured Gallbladder
- •4 Pancreas
- •Diffuse Pancreatic Change
- •Large Pancreas
- •Small Pancreas
- •Hypoechoic Texture
- •Hyperechoic Texture
- •Focal Changes
- •Anechoic Lesion
- •Hypoechoic Lesion
- •Isoechoic Lesion
- •Hyperechoic Lesion
- •Irregular (Complex Structured) Lesion
- •Dilatation of the Pancreatic Duct
- •Marginal/Mild Dilatation
- •Marked Dilatation
- •5 Spleen
- •Nonfocal Changes of the Spleen
- •Diffuse Parenchymal Changes
- •Large Spleen
- •Small Spleen
- •Focal Changes of the Spleen
- •Anechoic Mass
- •Hypoechoic Mass
- •Hyperechoic Mass
- •Splenic Calcification
- •6 Lymph Nodes
- •Peripheral Lymph Nodes
- •Head/Neck
- •Extremities (Axilla, Groin)
- •Abdominal Lymph Nodes
- •Porta Hepatis
- •Splenic Hilum
- •Mesentery (Celiac, Upper and Lower Mesenteric Station)
- •Stomach
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •Small/Large Intestine
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •8 Peritoneal Cavity
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Wall Structures
- •Smooth Margin
- •Irregular Margin
- •Intragastric Processes
- •Intraintestinal Processes
- •9 Kidneys
- •Anomalies, Malformations
- •Aplasia, Hypoplasia
- •Cystic Malformation
- •Anomalies of Number, Position, or Rotation
- •Fusion Anomaly
- •Anomalies of the Renal Calices
- •Vascular Anomaly
- •Diffuse Changes
- •Large Kidneys
- •Small Kidneys
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Irregular Structure
- •Circumscribed Changes
- •Anechoic Structure
- •Hypoechoic or Isoechoic Structure
- •Complex Structure
- •Hyperechoic Structure
- •10 Adrenal Glands
- •Enlargement
- •Anechoic Structure
- •Hypoechoic Structure
- •Complex Echo Structure
- •Hyperechoic Structure
- •11 Urinary Tract
- •Malformations
- •Duplication Anomalies
- •Dilatations and Stenoses
- •Dilated Renal Pelvis and Ureter
- •Anechoic
- •Hypoechoic
- •Hypoechoic
- •Hyperechoic
- •Large Bladder
- •Small Bladder
- •Altered Bladder Shape
- •Intracavitary Mass
- •Hypoechoic
- •Hyperechoic
- •Echogenic
- •Wall Changes
- •Diffuse Wall Thickening
- •Circumscribed Wall Thickening
- •Concavities and Convexities
- •12.1 The Prostate
- •Enlarged Prostate
- •Regular
- •Irregular
- •Small Prostate
- •Regular
- •Echogenic
- •Circumscribed Lesion
- •Anechoic
- •Hypoechoic
- •Echogenic
- •12.2 Seminal Vesicles
- •Diffuse Change
- •Hypoechoic
- •Circumscribed Change
- •Anechoic
- •Echogenic
- •Irregular
- •12.3 Testis, Epididymis
- •Diffuse Change
- •Enlargement
- •Decreased Size
- •Circumscribed Lesion
- •Anechoic or Hypoechoic
- •Irregular/Echogenic
- •Epididymal Lesion
- •Anechoic
- •Hypoechoic
- •Intrascrotal Mass
- •Anechoic or Hypoechoic
- •Echogenic
- •13 Female Genital Tract
- •Masses
- •Abnormalities of Size or Shape
- •Uterus
- •Abnormalities of Size or Shape
- •Myometrial Changes
- •Intracavitary Changes
- •Endometrial Changes
- •Fallopian Tubes
- •Hypoechoic Mass
- •Anechoic Cystic Mass
- •Solid Echogenic or Nonhomogeneous Mass
- •14 Thyroid Gland
- •Diffuse Changes
- •Enlarged Thyroid Gland
- •Small Thyroid Gland
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Circumscribed Changes
- •Anechoic
- •Hypoechoic
- •Isoechoic
- •Hyperechoic
- •Irregular
- •Differential Diagnosis of Hyperthyroidism
- •Types of Autonomy
- •15 Pleura and Chest Wall
- •Chest Wall
- •Masses
- •Parietal Pleura
- •Nodular Masses
- •Diffuse Pleural Thickening
- •Pleural Effusion
- •Anechoic Effusion
- •Echogenic Effusion
- •Complex Effusion
- •16 Lung
- •Masses
- •Anechoic Masses
- •Hypoechoic Masses
- •Complex Masses
- •Index
Pseudomyxoma Peritonei
Peritonei














































Pseudomyxoma peritonei is considered a rare, mainly low-grade, malignant diffuse tumor of the peritoneum. It is characterized by large amounts of mucin in the abdominal cavity, often seen during operations.
A differentiation can be made between diffuse peritoneal adenomucinosis (DPAM) with a more favorable outcome and a more aggressive peritoneal mucinous carcinomatosis (PMCA).4 Sonographically a septated or a structured ascites is visible, which concurs mainly with
DPAM (Fig. 8.33a,b).
Fig. 8.33
a Honeycomb-like ascites in a peritoneal pseudomyxoma. Longitudinal scan caudally of the right liver lobe with tangential section of the small bowel.
b Transversal scan in the right lower abdomen, same female patient. The puncture demonstrated a typic mucinous substrate.
Hyperechoic Structure
Cavity |
Diffuse Changes |
|||
|
|
|
||
|
|
|
|
Anechoic Structure |
Peritoneal |
|
Hypoechoic Structure |
||
|
Hyperechoic Structure |
|||
|
|
|
|
|
|
|
|
Localized Changes |
|
|
|
|
||
|
|
|
Wall Structures |
|
|
|
|
||
|
|
|
Differentiating Intraand Extraluminal |
|
|
|
|
||
|
|
|
GI Tract Fluid |
|
Pneumoperitoneum
Pneumoperitoneum

















































A collection of free intra-abdominal gas (pneumoperitoneum) is visualized as a hyperechoic structure with characteristic reverberation echoes and appears, for example, in free perforations of the GI tract. However, in general a frank perforation is a rare event (frequency only 1–2%).
Cause. The most common causes are:
●Duodenal/gastric ulcer
●Inflammatory bowel disease (appendicitis, diverticulitis, etc.)
●Postoperative, anastomotic/suture line leakage
●Iatrogenic (endoscopy, excision biopsy and polypectomy, contrast enema)
●Trauma, foreign body
●Tumor (stomach, colon)
The most common cause of a free perforation is mainly a postoperative or postendoscopic condition, a tumor complication, or a postinflammatory condition, rather than a gastric or duodenal ulcer. In complicated diverticulitis of the colon, which is not very uncommon, the leading symptom tends to be localized peritonitis of the left lower quadrant.
Sonographic morphology. In expert hands the signs of a free collection of intra-abdominal gas are easy to recognize (sensitivity 80–90%), and even a less experienced sonographer can reproduce these findings in postoperative patients after laparoscopic surgery and with vestiges of pneumoperitoneum. Follow-up studies of these patients provides excellent training. The most important signs of free intra-abdomi- nal gas are discussed below ( 8.4).5,6
8.4).5,6
●The characteristic localizations have already been mentioned above. If the echoes (gas) rise on patient repositioning, this is pathognomonic.
●The reverberation echoes at the preferred localizations already mentioned are characteristic of perforation.
●The additional leakage of fluid, quite often with internal echoes, is another sign of GI tract injury.
●Compared with intraluminal gas collections in the GI tract, marked breathing movement will not result in positional changes (constant respiratory position).
●Furthermore, in the left lateral position there is a discontinuity between the gas in the distal segments of the lungs and the free gas anterior to the liver.
●In the superior compartment, however (e. g., below the diaphragm with the patient upright or below the abdominal wall with the patient supine), the echoes there will shift when repositioning the patient.
8
Diffuse Changes
307
8
Peritoneal Cavity
 8.4 Ultrasound Signs of Free Intra-abdominal Gas
8.4 Ultrasound Signs of Free Intra-abdominal Gas
●Multiple reverberation echoes
●Characteristic localizations (see above)
●Additional fluid with internal echoes
●No change in position with breathing movements
●Pleuroperitoneal discontinuity
●Hyperechoic echoes in the superior recesses
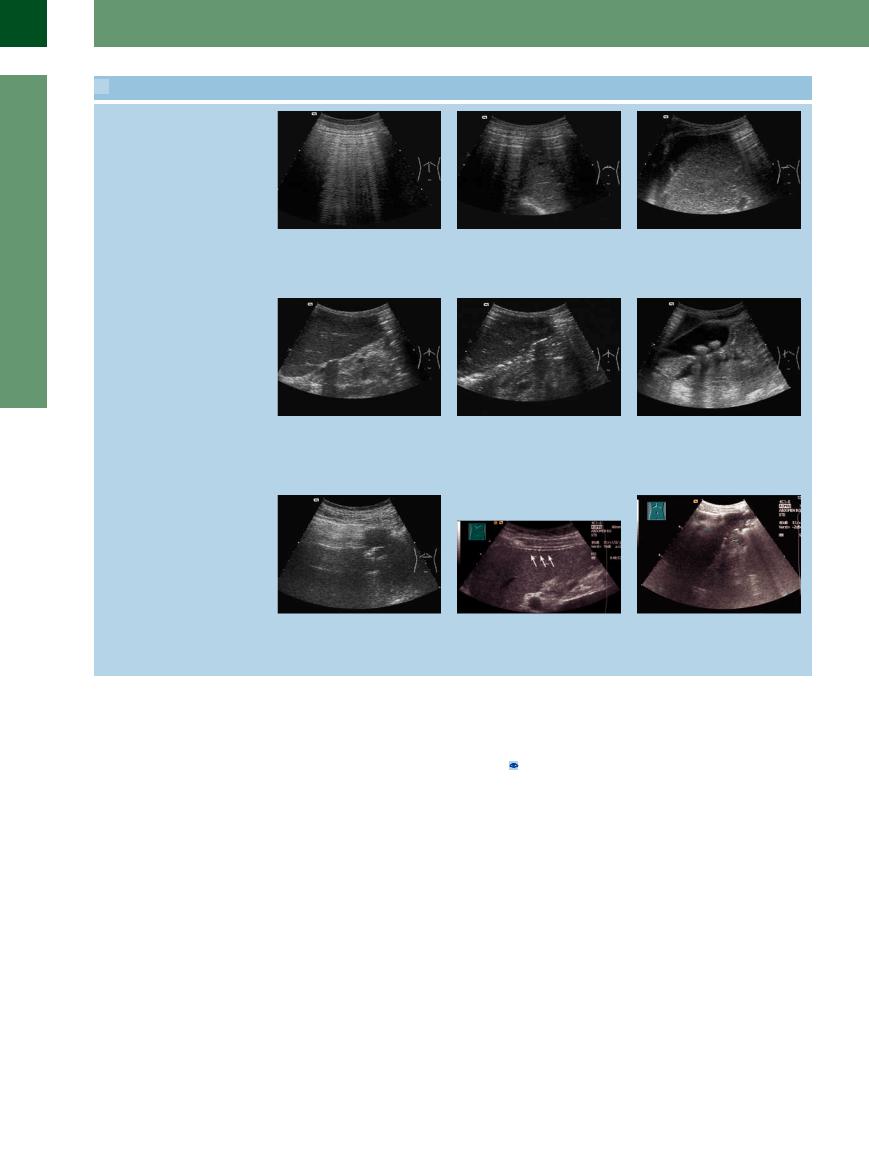
a Hyperechoic intra-abdominal collection of gas. No organs can be visualized behind the curtain of free gas, characteristic reverberation echoes.
d At the lower margin of the left hepatic lobe: hyperechoic structure (free gas). Posterior to the left hepatic lobe: intense echo complex with posterior shadowing marking the site of the perforation (duodenal ulcer).
g In the transverse plane of the epigastric region: a small section of the left hepatic lobe. The rest of the organ is masked by the free gas. Status post perforation of the colon in cancer of the hepatic flexure.
b Hyperechoic collection of gas anterior to the left and right hepatic lobe; parts of the liver are masked. Status post perforation of a duodenal ulcer.
e Anterior to and at the lower margin of the left hepatic lobe: free gas (hyperechoic). Posterior to the left hepatic lobe: a string of small hyperechoic gas bubbles.
h Very small amounts of gas in the intraabdominal cavity can be particularly well seen sonographically between the right liver lobe and the lateral abdominal wall.
c Apart from the free perihepatic gas on the right of the liver, there is also echogenic free fluid. Free gas + fluid is indicative of a perforated GI tract (here, perforated duodenal ulcer).
f In the longitudinal plane: some free gas anterior to and to the right of the calculous gallbladder.
i Hyperechoic gas collection at the posterior margin of the left liver lobe caused by dislocated PEG. Free gas with reverberations between the left liver lobe and the ventral abdominal wall.
■ Localized Changes
“Pseudoascites.” Diagnosis of anechoic and |
number of fluid collections discussed else- |
● Preformed hollow viscera filled with liquid |
hypoechoic intra-abdominal structures has to |
where, the most important being ( 8.5): |
(urinary bladder, gallbladder hydrops) |
differentiate them from fluid collections with- |
● Abscess |
● Aortic aneurysm |
out connection to the abdominal cavity. The |
● Hematoma |
● Hydronephrosis |
latter are also called “pseudoascites.” This |
● Cysts (liver, kidney, pancreas pseudocysts, |
● Ileus and gastric outlet obstruction |
term is something of a misnomer since the |
ovaries) |
● Hypoechoic masses (e. g., lymphoma) |
fluid is not actually ascites but rather structures |
● Ovarian cystoma and other cystic masses |
● Fluid processes within the abdominal wall |
outside the abdominal cavity that are not in- |
(cystadenoma, cystadenocarcinoma) |
|
terconnected with it. This includes quite a |
● Mesothelioma, lymphangioma |
|
308
 8.5 Differentiating Fluid Masses from Ascites
8.5 Differentiating Fluid Masses from Ascites
●Liver
●Abdominal wall
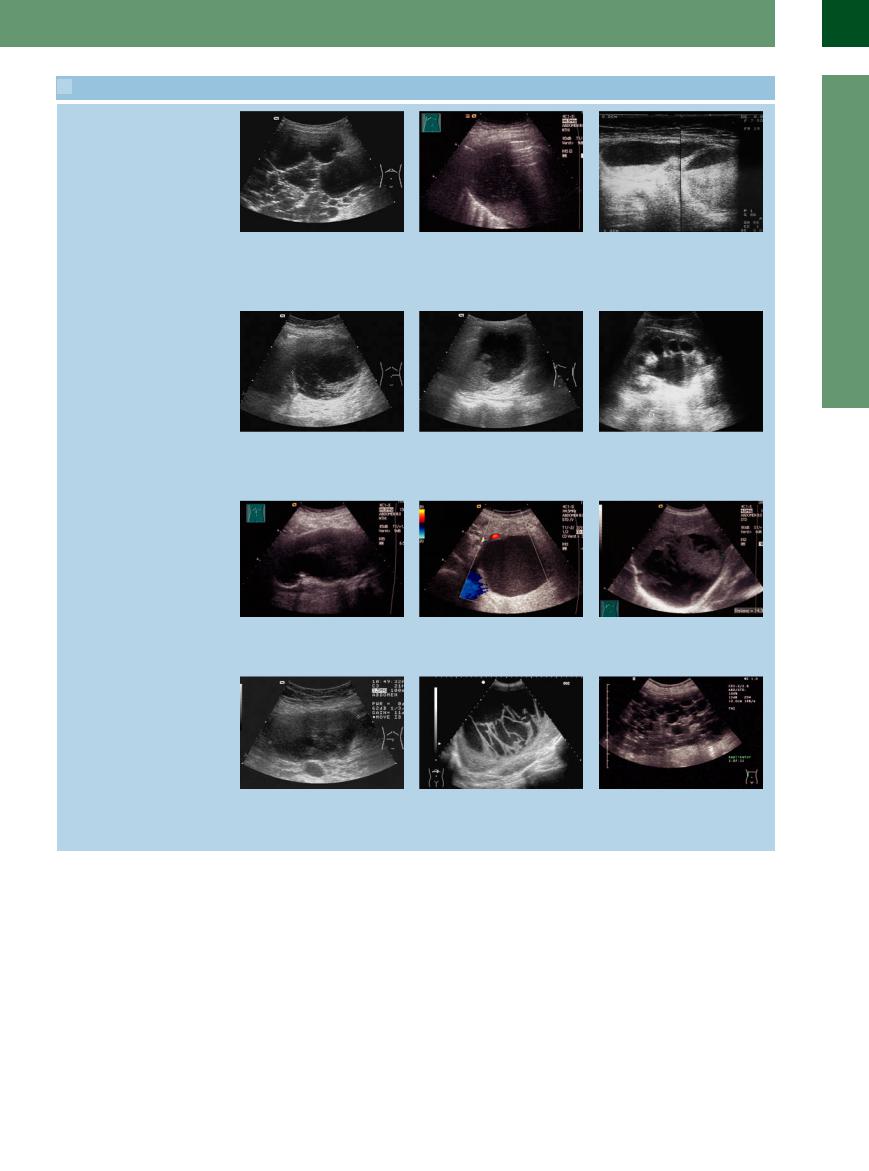
a Polycystic liver: to be differentiated from |
b A new large hypoechoic liquid formation |
c Septated collection of fluid with some |
septated ascites in the upper quadrants. |
is allocated to the liver and constitutes a |
sedimentation of the contents: massive |
|
cholangitic liver abscess. |
hematoma after heparin-induced throm- |
|
|
bocytopenia, totally within the abdominal |
|
|
wall and therefore extraperitoneal in lo- |
|
|
cation. |
●Pancreas
●Spleen
●Kidney
d Localized cystic mass in the left upper quadrant, permeated by septum-like structures; no walled-off pancreatogenous ascites but cystic malignancy of the pancreas (cystadenocarcinoma).
g Large liquid formation with thrombotic parts situated in the median line; extensive typically located aneurysm of the aorta.
j A large hypoechoic solid form located in the middle of the abdomen is a large lymphoma; color Doppler or contrast-en- hanced ultrasound can delineate the lymphoma clearly from liquid structures.
e Irregularly defined collection of fluid within the spleen: invasion of a pancreatic pseudocyst.
h Post-acute pancreatic pseudocyst with homogeneous content situated posterior to the stomach.
k Large echogenic form well delineated from the surrounding splenic tissue is a large partly organized splenic hematoma.
f Massively dilated renal calices and pelvis. No parenchymal margin to be visualized; hydronephrotic nephrectasia; no interconnection with the abdominal cavity.
i Crowding liquid formation with solid parts in the lumen is located in the right liver lobe; large partially hemorrhagic liver cyst.
l Large honeycomb-like structured fluid collection in the right upper and middle abdomen caused by a polycystic kidney disease.
8
Localized Changes
309
8
Peritoneal Cavity
Anechoic Structure
Cavity |
Diffuse Changes |
|||
|
|
|
||
|
|
|
Localized Changes |
|
Peritoneal |
|
Anechoic Structure |
||
|
||||
|
Hypoechoic Structure |
|||
|
|
|
|
|
|
|
|
|
Hyperechoic Structure |
|
|
|
Wall Structures |
|
|
|
|
||
|
|
|
Differentiating Intraand Extraluminal |
|
|
|
|
||
|
|
|
GI Tract Fluid |
|
Septated Ascites
Intra-abdominal Abscess
Septated Ascites
Ascites




























If there is no unrestricted intercompartmental connection, e. g., as may be the case in the presence of adhesions, the collection of intraabdominal fluid will be localized. Classic examples are the septated ascites in peritoneal carcinomatosis with adhesions (Fig. 8.34) and in pancreatitis (Fig. 8.35). The example of an isolated septated exudation into the omental bursa has already been mentioned ( 8.2e).
8.2e).
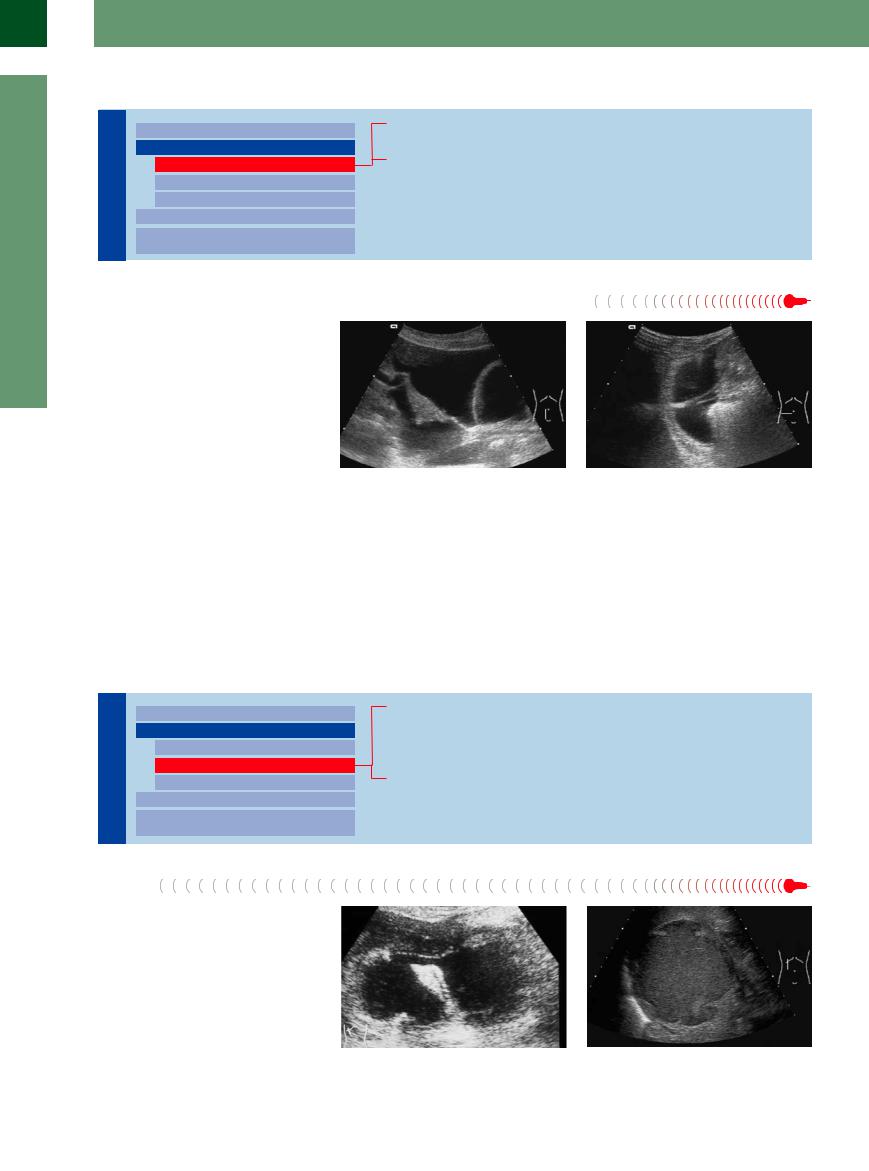
Fig. 8.34 Septated ascites in peritoneal carcinomatosis (ovarian malignancy). The septa may compartmentalize the fluid, which then will not shift freely on repositioning of the patient.
Fig. 8.35 In necrotizing pancreatitis, septation may also result in compartmentalization, thus “trapping” the ascites. Here, too, the fluid cannot shift freely on repositioning of the patient.
Intra-abdominal Abscess
Abscess 














































Inflammatory adhesions may also wall off in- |
rarely anechoic but more commonly tend to |
tra-abdominal collections of fluid, for instance |
be hypoechoic. |
in abscesses. However, these structures are |
|
Hypoechoic Structure
Cavity |
Diffuse Changes |
|||
|
|
|
||
|
|
|
Localized Changes |
|
|
|
|
||
Peritoneal |
|
Anechoic Structure |
||
|
Hypoechoic Structure |
|||
|
|
|
|
|
|
|
|
|
Hyperechoic Structure |
|
|
|
Wall Structures |
|
|
|
|
||
|
|
|
Differentiating Intraand Extraluminal |
|
|
|
|
||
|
|
|
GI Tract Fluid |
|
Abscess
Bilioma
Hematoma
Necrosis After Pancreatitis
Abscess
Intra-abdominal abscess (e. g., between the bowel loops, subphrenic, or subhepatic) is mainly hypoechoic and displays an inhomogeneous structure. In most cases the margin is irregular (Fig. 8.36, Fig. 8.37). Less frequently the abscess may be anechoic or hyperechoic; this is particularly true in gas abscess due to bacterial colonization. The diagnosis is facilitated by the presence of the appropriate clinical symptoms with markedly elevated blood markers, fever, and pain.
Fig. 8.36 Two large, irregularly defined hypoechoic abscesses below the liver after cholecystectomy. The narrow interconnection between the abscesses permits the fluid to communicate; successful interventional treatment with two drains.
Fig. 8.37 Localized, irregularly defined echogenic process around the right liver after pancreatitis: abscess.
310