

- •Contents
- •Preface
- •Contributors
- •1 Vessels
- •1.1 Aorta, Vena Cava, and Peripheral Vessels
- •Aorta, Arteries
- •Anomalies and Variant Positions
- •Dilatation
- •Stenosis
- •Wall Thickening
- •Intraluminal Mass
- •Perivascular Mass
- •Vena Cava, Veins
- •Anomalies
- •Dilatation
- •Intraluminal Mass
- •Compression, Infiltration
- •1.2 Portal Vein and Its Tributaries
- •Enlarged Lumen Diameter
- •Portal Hypertension
- •Intraluminal Mass
- •Thrombosis
- •Tumor
- •2 Liver
- •Enlarged Liver
- •Small Liver
- •Homogeneous Hypoechoic Texture
- •Homogeneous Hyperechoic Texture
- •Regionally Inhomogeneous Texture
- •Diffuse Inhomogeneous Texture
- •Anechoic Masses
- •Hypoechoic Masses
- •Isoechoic Masses
- •Hyperechoic Masses
- •Echogenic Masses
- •Irregular Masses
- •Differential Diagnosis of Focal Lesions
- •Diagnostic Methods
- •Suspected Diagnosis
- •3 Biliary Tree and Gallbladder
- •3.1 Biliary Tree
- •Thickening of the Bile Duct Wall
- •Localized and Diffuse
- •Bile Duct Rarefaction
- •Localized and Diffuse
- •Bile Duct Dilatation and Intraductal Pressure
- •Intrahepatic
- •Hilar and Prepancreatic
- •Intrapancreatic
- •Papillary
- •Abnormal Intraluminal Bile Duct Findings
- •Foreign Body
- •The Seven Most Important Questions
- •3.2 Gallbladder
- •Changes in Size
- •Large Gallbladder
- •Small/Missing Gallbladder
- •Wall Changes
- •General Hypoechogenicity
- •General Hyperechogenicity
- •General Tumor
- •Focal Tumor
- •Intraluminal Changes
- •Hyperechoic
- •Hypoechoic
- •Nonvisualized Gallbladder
- •Missing Gallbladder
- •Obscured Gallbladder
- •4 Pancreas
- •Diffuse Pancreatic Change
- •Large Pancreas
- •Small Pancreas
- •Hypoechoic Texture
- •Hyperechoic Texture
- •Focal Changes
- •Anechoic Lesion
- •Hypoechoic Lesion
- •Isoechoic Lesion
- •Hyperechoic Lesion
- •Irregular (Complex Structured) Lesion
- •Dilatation of the Pancreatic Duct
- •Marginal/Mild Dilatation
- •Marked Dilatation
- •5 Spleen
- •Nonfocal Changes of the Spleen
- •Diffuse Parenchymal Changes
- •Large Spleen
- •Small Spleen
- •Focal Changes of the Spleen
- •Anechoic Mass
- •Hypoechoic Mass
- •Hyperechoic Mass
- •Splenic Calcification
- •6 Lymph Nodes
- •Peripheral Lymph Nodes
- •Head/Neck
- •Extremities (Axilla, Groin)
- •Abdominal Lymph Nodes
- •Porta Hepatis
- •Splenic Hilum
- •Mesentery (Celiac, Upper and Lower Mesenteric Station)
- •Stomach
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •Small/Large Intestine
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •8 Peritoneal Cavity
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Wall Structures
- •Smooth Margin
- •Irregular Margin
- •Intragastric Processes
- •Intraintestinal Processes
- •9 Kidneys
- •Anomalies, Malformations
- •Aplasia, Hypoplasia
- •Cystic Malformation
- •Anomalies of Number, Position, or Rotation
- •Fusion Anomaly
- •Anomalies of the Renal Calices
- •Vascular Anomaly
- •Diffuse Changes
- •Large Kidneys
- •Small Kidneys
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Irregular Structure
- •Circumscribed Changes
- •Anechoic Structure
- •Hypoechoic or Isoechoic Structure
- •Complex Structure
- •Hyperechoic Structure
- •10 Adrenal Glands
- •Enlargement
- •Anechoic Structure
- •Hypoechoic Structure
- •Complex Echo Structure
- •Hyperechoic Structure
- •11 Urinary Tract
- •Malformations
- •Duplication Anomalies
- •Dilatations and Stenoses
- •Dilated Renal Pelvis and Ureter
- •Anechoic
- •Hypoechoic
- •Hypoechoic
- •Hyperechoic
- •Large Bladder
- •Small Bladder
- •Altered Bladder Shape
- •Intracavitary Mass
- •Hypoechoic
- •Hyperechoic
- •Echogenic
- •Wall Changes
- •Diffuse Wall Thickening
- •Circumscribed Wall Thickening
- •Concavities and Convexities
- •12.1 The Prostate
- •Enlarged Prostate
- •Regular
- •Irregular
- •Small Prostate
- •Regular
- •Echogenic
- •Circumscribed Lesion
- •Anechoic
- •Hypoechoic
- •Echogenic
- •12.2 Seminal Vesicles
- •Diffuse Change
- •Hypoechoic
- •Circumscribed Change
- •Anechoic
- •Echogenic
- •Irregular
- •12.3 Testis, Epididymis
- •Diffuse Change
- •Enlargement
- •Decreased Size
- •Circumscribed Lesion
- •Anechoic or Hypoechoic
- •Irregular/Echogenic
- •Epididymal Lesion
- •Anechoic
- •Hypoechoic
- •Intrascrotal Mass
- •Anechoic or Hypoechoic
- •Echogenic
- •13 Female Genital Tract
- •Masses
- •Abnormalities of Size or Shape
- •Uterus
- •Abnormalities of Size or Shape
- •Myometrial Changes
- •Intracavitary Changes
- •Endometrial Changes
- •Fallopian Tubes
- •Hypoechoic Mass
- •Anechoic Cystic Mass
- •Solid Echogenic or Nonhomogeneous Mass
- •14 Thyroid Gland
- •Diffuse Changes
- •Enlarged Thyroid Gland
- •Small Thyroid Gland
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Circumscribed Changes
- •Anechoic
- •Hypoechoic
- •Isoechoic
- •Hyperechoic
- •Irregular
- •Differential Diagnosis of Hyperthyroidism
- •Types of Autonomy
- •15 Pleura and Chest Wall
- •Chest Wall
- •Masses
- •Parietal Pleura
- •Nodular Masses
- •Diffuse Pleural Thickening
- •Pleural Effusion
- •Anechoic Effusion
- •Echogenic Effusion
- •Complex Effusion
- •16 Lung
- •Masses
- •Anechoic Masses
- •Hypoechoic Masses
- •Complex Masses
- •Index
15
Pleura and Chest Wall
Complex Effusion
Wall |
|
|
|
Chest Wall |
|
|
|
|
|
||
|
|
|
|
Parietal Pleura |
|
|
|
|
|||
|
|
|
|
Pleural Effusion |
|
Chest |
|
|
|
||
|
|
|
|
Anechoic Effusion |
|
|
|
|
|
|
|
andPleura |
|
|
|
|
Echogenic Effusion |
|
|
|
|
Complex Effusion |
|
|
|
|
|
|
|
Inflammatory or Malignant Effusion Fibrothorax
Seropneumothorax, Pneumothorax
Inflammatory or Malignant
Malignant Effusion
Effusion








































Ultrasound examination of a complex pleural effusion will show varying degrees of fibrin stranding and septation, ranging to a honey- comb-like permeation of the pleural cavity in extreme cases. These structures are defined less clearly by CT than by ultrasound. The ultra- sound-guided aspiration of septated effusions can be rewarding in clinically symptomatic patients, consistently yielding an exudative fluid. Various degrees of pleural thickening are seen. These findings are characteristic of an inflammatory or malignant effusion.
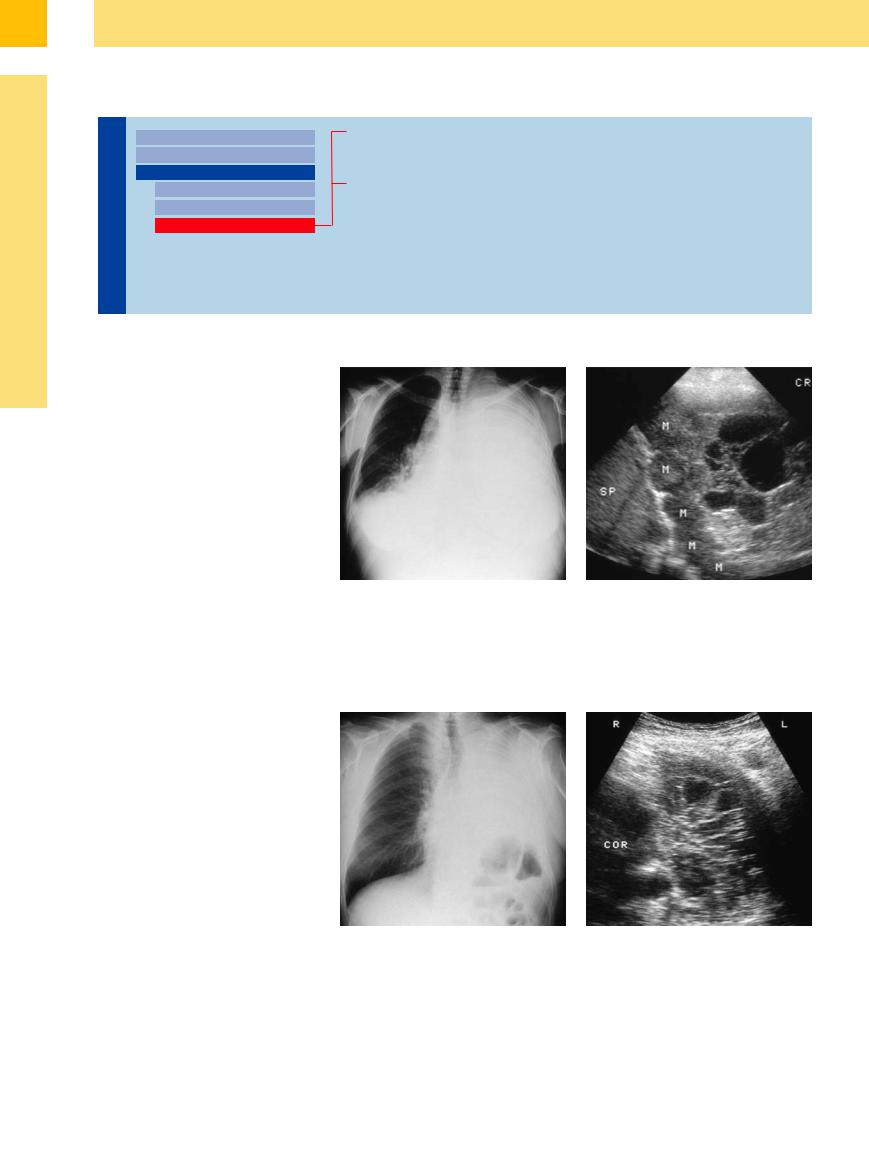
In the latter case, it is not uncommon to find nodular tumor masses in the effusion when disease is advanced (Fig.15.20). Ultrasoundguided percutaneous drainage is no longer beneficial in these cases.
Fig. 15.20 Low-grade non-Hodgkin lymphoma in a 21- year-old woman.
a Chest radiograph shows complete opacification of the left lung.
b Left lateral intercostal scan shows an extensive, loculated pleural effusion with a string-of-beads arrangement of nodular masses (M) along the diaphragmatic pleura. Cytology confirmed lymphomatous involvement of the pleura. SP = spleen.
Fibrothorax 





















































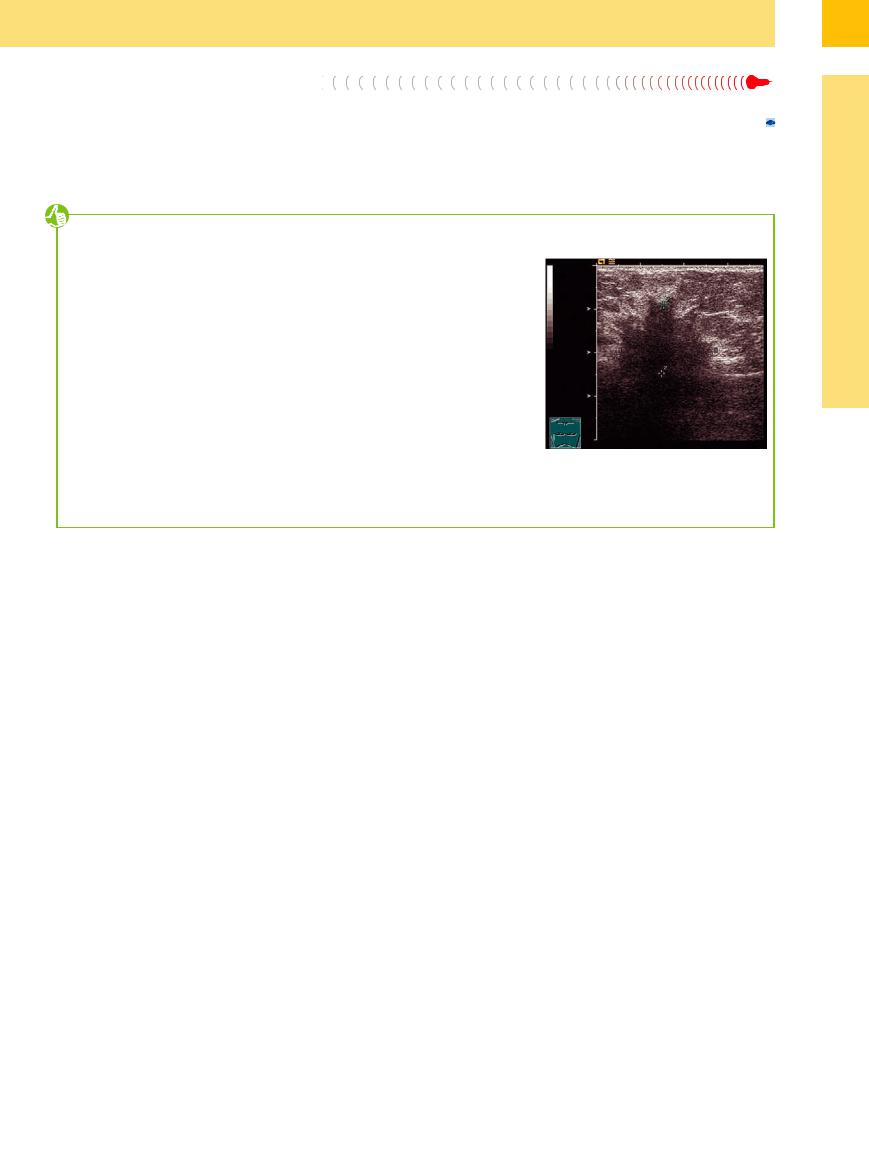
Fibrothorax is a special type of complex effusion that develops following unilateral pneumonectomy (Fig.15.21).
Fig. 15.21 A 65-year-old man who had previously under- |
b Left anterior intercostal scan shows a nonhomogene- |
gone pneumonectomy for bronchial carcinoma. |
ous, solid/cystic-appearing mass consistent with a fibro- |
a Chest radiograph shows complete opacification of the |
thorax. COR = heart. |
left hemithorax. |
|
528
15
Pleural Effusion
Tips, tricks, and pitfalls
In females, a thoracic wall mass may be indicative of a mammary carcinoma, even in cancer of unknown primary site (CUP) syndrome (Fig. 15.22).10
For tumors of the breast, mammography has a general sensitivity of 75–90%; it is even higher (93–99%) in MRI, with better specificity.
In women less than 40 years of age, ultrasonography is the primary method of choice, as it is considered to be better than mammography in dense tissues.
Criteria in real-time ultrasonography are:
●echogenicity and attenuation
●movability with palpation
●compression, local retraction and “crow’s feet”
●microcalcifications (inside and aside the lesion), macrocalcifications (> 5 mm)
References
[1]Mathis G. Thoraxsonography—Part I: Chest wall and pleura. Ultrasound Med Biol 1997;23(8):1131–1139
[2]Reuß J. Sonographic imaging of the pleura: nearly 30 years experience. Eur J Ultrasound 1996;3:125–139
[3]Wernecke K. Sonographic features of pleural disease. AJR Am J Roentgenol 1997;168(4): 1061–1066
[4]Bitschnau R, Gehmacher O, Kopf A, Scheier M, Mathis G. Ultraschalldiagnostik von Rippenund Sternumfrakturen [Ultrasound in the di-
●demonstration of complicated cysts (grapelike or irregularly shaped) with infiltrated and or distended milk canaliculi
●vascularization:
–no vessels
–number of vessels
–contrast pattern
–contrast enhancement and augmented vascularization (as a differential diagnostic sign to fibroadenoma)
●changes in surrounding tissue
agnosis of rib and sternal fractures]. Ultraschall Med 1997;18(4):158–161
[5]Yang PC, Lee LN, Luh KT, Kuo SH, Yang SP. Ultrasonography of Pancoast tumor. Chest 1988;94(1):124–128
[6]Görg C, Görg K, Schwerk WB, Kleinsorge F. Sonographie der Pleura diaphragmatica bei Tumorpatienten [Sonography of the diaphragmatic pleura in tumor patients]. Ultraschall Med 1988;9(6):274–278
[7]Goerg C, Schwerk WB, Goerg K, Walters E. Pleural effusion: an “acoustic window” for sonography of pleural metastases. J Clin Ultrasound 1991;19(2):93–97
Fig. 15.22 Ill-defined hypoechoic breast mass in a 69- year-old woman: clinically, hard, fixed and painless nodule of the right breast.10
[8]Gehmacher O, Kopf A, Scheier M, Bitschnau R, Wertgen T, Mathis G. Ist eine Pleuritis sonographisch darstellbar?[ Can pleurisy be detected with ultrasound?] Ultraschall Med 1997;18(5):214–219
[9]Goecke W, Schwerk WB. Die Real-Time Sonographie in der Diagnostik von Pleuraergüs-
sen. In: Gebhardt J et al. (eds.). Ultraschalldiagnostik 89. Berlin: Springer, 1990;
pp. 385–387
[10]Schmidt G, Ed. Ultrasound Thieme Clinical Companions. Stuttgart· New York: Thieme, 2007
529
