

- •Contents
- •Preface
- •Contributors
- •1 Vessels
- •1.1 Aorta, Vena Cava, and Peripheral Vessels
- •Aorta, Arteries
- •Anomalies and Variant Positions
- •Dilatation
- •Stenosis
- •Wall Thickening
- •Intraluminal Mass
- •Perivascular Mass
- •Vena Cava, Veins
- •Anomalies
- •Dilatation
- •Intraluminal Mass
- •Compression, Infiltration
- •1.2 Portal Vein and Its Tributaries
- •Enlarged Lumen Diameter
- •Portal Hypertension
- •Intraluminal Mass
- •Thrombosis
- •Tumor
- •2 Liver
- •Enlarged Liver
- •Small Liver
- •Homogeneous Hypoechoic Texture
- •Homogeneous Hyperechoic Texture
- •Regionally Inhomogeneous Texture
- •Diffuse Inhomogeneous Texture
- •Anechoic Masses
- •Hypoechoic Masses
- •Isoechoic Masses
- •Hyperechoic Masses
- •Echogenic Masses
- •Irregular Masses
- •Differential Diagnosis of Focal Lesions
- •Diagnostic Methods
- •Suspected Diagnosis
- •3 Biliary Tree and Gallbladder
- •3.1 Biliary Tree
- •Thickening of the Bile Duct Wall
- •Localized and Diffuse
- •Bile Duct Rarefaction
- •Localized and Diffuse
- •Bile Duct Dilatation and Intraductal Pressure
- •Intrahepatic
- •Hilar and Prepancreatic
- •Intrapancreatic
- •Papillary
- •Abnormal Intraluminal Bile Duct Findings
- •Foreign Body
- •The Seven Most Important Questions
- •3.2 Gallbladder
- •Changes in Size
- •Large Gallbladder
- •Small/Missing Gallbladder
- •Wall Changes
- •General Hypoechogenicity
- •General Hyperechogenicity
- •General Tumor
- •Focal Tumor
- •Intraluminal Changes
- •Hyperechoic
- •Hypoechoic
- •Nonvisualized Gallbladder
- •Missing Gallbladder
- •Obscured Gallbladder
- •4 Pancreas
- •Diffuse Pancreatic Change
- •Large Pancreas
- •Small Pancreas
- •Hypoechoic Texture
- •Hyperechoic Texture
- •Focal Changes
- •Anechoic Lesion
- •Hypoechoic Lesion
- •Isoechoic Lesion
- •Hyperechoic Lesion
- •Irregular (Complex Structured) Lesion
- •Dilatation of the Pancreatic Duct
- •Marginal/Mild Dilatation
- •Marked Dilatation
- •5 Spleen
- •Nonfocal Changes of the Spleen
- •Diffuse Parenchymal Changes
- •Large Spleen
- •Small Spleen
- •Focal Changes of the Spleen
- •Anechoic Mass
- •Hypoechoic Mass
- •Hyperechoic Mass
- •Splenic Calcification
- •6 Lymph Nodes
- •Peripheral Lymph Nodes
- •Head/Neck
- •Extremities (Axilla, Groin)
- •Abdominal Lymph Nodes
- •Porta Hepatis
- •Splenic Hilum
- •Mesentery (Celiac, Upper and Lower Mesenteric Station)
- •Stomach
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •Small/Large Intestine
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •8 Peritoneal Cavity
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Wall Structures
- •Smooth Margin
- •Irregular Margin
- •Intragastric Processes
- •Intraintestinal Processes
- •9 Kidneys
- •Anomalies, Malformations
- •Aplasia, Hypoplasia
- •Cystic Malformation
- •Anomalies of Number, Position, or Rotation
- •Fusion Anomaly
- •Anomalies of the Renal Calices
- •Vascular Anomaly
- •Diffuse Changes
- •Large Kidneys
- •Small Kidneys
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Irregular Structure
- •Circumscribed Changes
- •Anechoic Structure
- •Hypoechoic or Isoechoic Structure
- •Complex Structure
- •Hyperechoic Structure
- •10 Adrenal Glands
- •Enlargement
- •Anechoic Structure
- •Hypoechoic Structure
- •Complex Echo Structure
- •Hyperechoic Structure
- •11 Urinary Tract
- •Malformations
- •Duplication Anomalies
- •Dilatations and Stenoses
- •Dilated Renal Pelvis and Ureter
- •Anechoic
- •Hypoechoic
- •Hypoechoic
- •Hyperechoic
- •Large Bladder
- •Small Bladder
- •Altered Bladder Shape
- •Intracavitary Mass
- •Hypoechoic
- •Hyperechoic
- •Echogenic
- •Wall Changes
- •Diffuse Wall Thickening
- •Circumscribed Wall Thickening
- •Concavities and Convexities
- •12.1 The Prostate
- •Enlarged Prostate
- •Regular
- •Irregular
- •Small Prostate
- •Regular
- •Echogenic
- •Circumscribed Lesion
- •Anechoic
- •Hypoechoic
- •Echogenic
- •12.2 Seminal Vesicles
- •Diffuse Change
- •Hypoechoic
- •Circumscribed Change
- •Anechoic
- •Echogenic
- •Irregular
- •12.3 Testis, Epididymis
- •Diffuse Change
- •Enlargement
- •Decreased Size
- •Circumscribed Lesion
- •Anechoic or Hypoechoic
- •Irregular/Echogenic
- •Epididymal Lesion
- •Anechoic
- •Hypoechoic
- •Intrascrotal Mass
- •Anechoic or Hypoechoic
- •Echogenic
- •13 Female Genital Tract
- •Masses
- •Abnormalities of Size or Shape
- •Uterus
- •Abnormalities of Size or Shape
- •Myometrial Changes
- •Intracavitary Changes
- •Endometrial Changes
- •Fallopian Tubes
- •Hypoechoic Mass
- •Anechoic Cystic Mass
- •Solid Echogenic or Nonhomogeneous Mass
- •14 Thyroid Gland
- •Diffuse Changes
- •Enlarged Thyroid Gland
- •Small Thyroid Gland
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Circumscribed Changes
- •Anechoic
- •Hypoechoic
- •Isoechoic
- •Hyperechoic
- •Irregular
- •Differential Diagnosis of Hyperthyroidism
- •Types of Autonomy
- •15 Pleura and Chest Wall
- •Chest Wall
- •Masses
- •Parietal Pleura
- •Nodular Masses
- •Diffuse Pleural Thickening
- •Pleural Effusion
- •Anechoic Effusion
- •Echogenic Effusion
- •Complex Effusion
- •16 Lung
- •Masses
- •Anechoic Masses
- •Hypoechoic Masses
- •Complex Masses
- •Index
3
Biliary Tree and Gallbladder
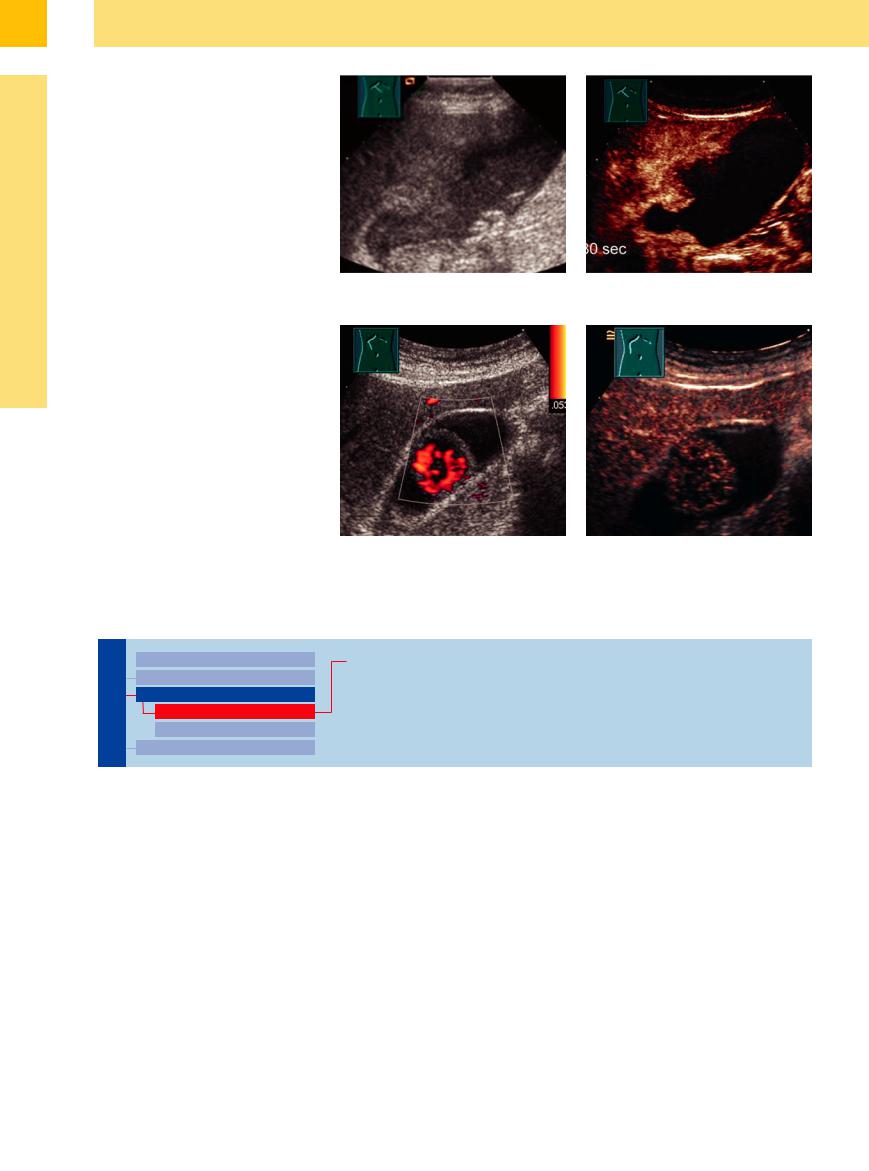
Fig. 3.64 Continued.
d Echoic gallbladder, ill-defined margins to the liver. Calculi on the bottom, probably sludge.
e Contrast-enhanced US (30 s): unequivocally infiltrating carcinoma into the liver with enhancing. The remaining gallbladder is without vessels delimiting the tumor from the gallbladder.
Metastasis






















































Metastases in the wall of the gallbladder and hepatic metastases infiltrating the gallbladder from the liver may mimic primary carcinoma of the gallbladder wall and do not display any characteristic ultrasound morphology (Fig. 3.65). Metastasis in the gallbladder wall is a rare finding and cannot be clearly differentiated by sonography from true gallbladder carcinoma.
Fig. 3.65 Metastasis in the gallbladder wall of malignant melanoma (FNB, histology).
a Vascularized mass, CDS.
b CEUS with intratumoral enhancement.
■ Intraluminal Changes
Hyperechoic
Gallbladder |
|
Changes in Size |
Gallstones |
|
|||
|
|
|
Wall Changes
Intraluminal Changes
Hyperechoic
Hypoechoic
Nonvisualized Gallbladder
Gallstones 






















































Gallstones are the classic example of mobile changes within the gallbladder. The wellknown mnemonic of “the five Fs”—fat, female, fertile, forty, fair—characterizes the segment of the population most at risk for cholecystolithiasis.
Typically, gallbladder stones are mobile and differ in their extent of posterior shadowing (depending on the size of the calculus) as well as in their intrinsic pattern ( 3.7). The sonographic morphology of the stones depends on their size, shape, and composition. Usually, the gallstones are a mixture of cholesterol, calcium, and bilirubin and are located at the most dependent part of the gallbladder. When looking for calculi it should be remembered that with the patient supine the stones are more likely to
3.7). The sonographic morphology of the stones depends on their size, shape, and composition. Usually, the gallstones are a mixture of cholesterol, calcium, and bilirubin and are located at the most dependent part of the gallbladder. When looking for calculi it should be remembered that with the patient supine the stones are more likely to
be found in the neck of the gallbladder, while in the left lateral decubitus position they tend to collect in the region of the fundus/body ( 3.7a–c). Fairly large pure cholesterol stones (up to 60 mm) may float in the liquid bile.
3.7a–c). Fairly large pure cholesterol stones (up to 60 mm) may float in the liquid bile.
Shadowing can be observed in gallstones with a diameter down to about 2–3 mm, depending on the quality of the stone as well as the equipment used and the frequency employed. Calculi with a diameter of less than 5 mm are called microliths. From a diameter of 8 mm and upward, subtle differentiation of the gallstones into cholesterol, calcium, and pigmented calculi usually does not present any problem.12 In microliths with a diameter of less than 5 mm, assessment of the intrinsic echo pattern may become difficult. Here, addi-
tional data such as tabular structure and comet-tail artifacts as well as any flotation of the stones (rich in cholesterol) and their size and shape (usually hyperechoic microliths dependent in the gallbladder are of mixed calcium composition) have to be taken into account (Table 3.4). Ultrasound morphology is essential when planning possible lysis or shock-wave lithotripsy.
Differentiating gallstones. The criteria for differentiating gallstones are their intrinsic echo pattern, surface echo, and posterior shadowing ( 3.7 d–i). Although gallstones are best visualized at the focus of the transducer, the quality and settings of the platform used are extremely important as well. Optimized differentiation of
3.7 d–i). Although gallstones are best visualized at the focus of the transducer, the quality and settings of the platform used are extremely important as well. Optimized differentiation of
160
the calculi is possible only if the transmission |
detected by rolling the patient by 360 ° once or |
between microliths (cholesterol crystals) and |
power matches the situation at hand. Occasion- |
more on the examination table (the so-called |
sludge is difficult. Clinical relevance (lysis, op- |
ally, very small hidden microliths can only be |
“Jacobeit rolling maneuver”). Differentiating |
eration) is determined by clinical data. |
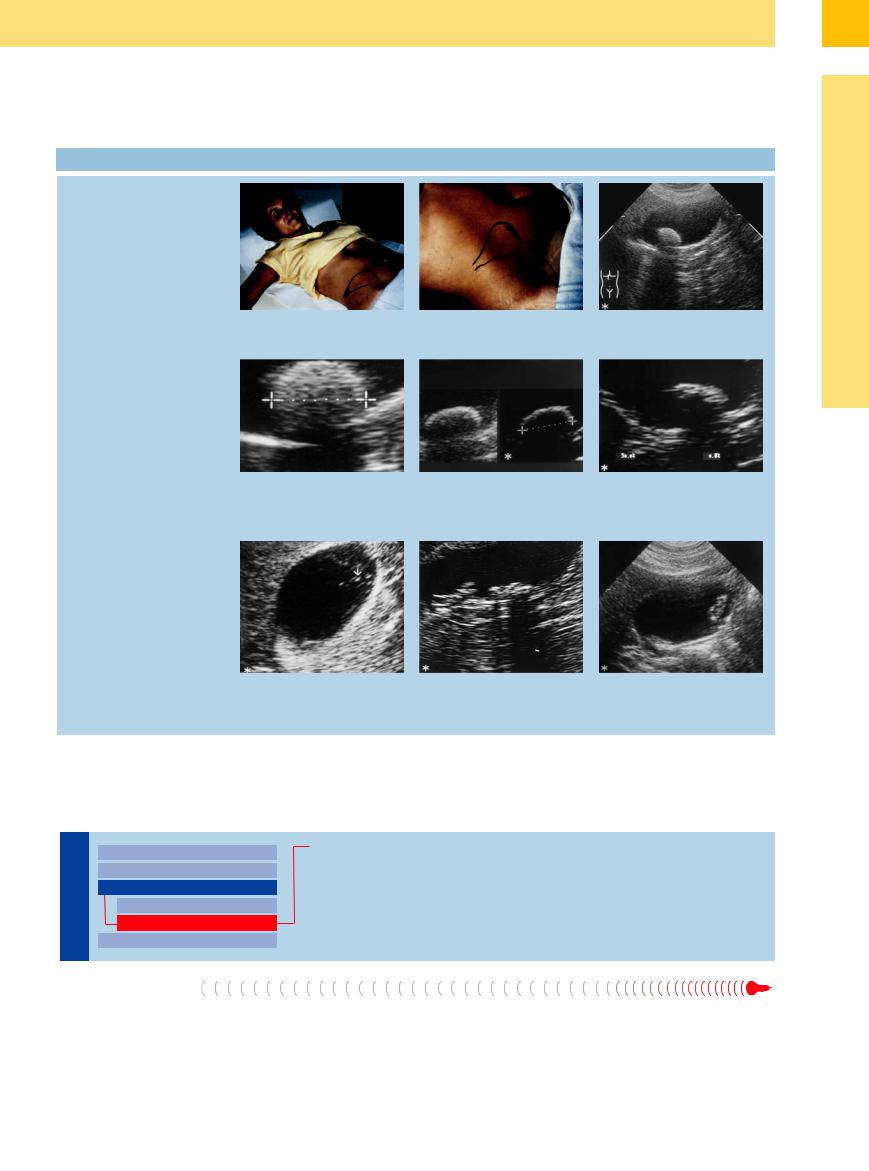
 3.7 Differentiating Gallstones by Ultrasound
3.7 Differentiating Gallstones by Ultrasound
Differentiating calculi in the supine and left lateral decubitus position
Differentiating calculi with a diameter > 8 mm
Differentiating calculi with a diameter < 8 mm
a Supine—the stones are more likely to collect in the neck of the gallbladder.
d Cholesterol gallstone: fine crystalline homogeneous intrinsic echo pattern (“through transmission”) with comet-tail artifacts, weak surface echo, soft posterior shadowing.
b Left lateral decubitus—the calculi will be located at the fundus/body of the gallbladder.
e Calcium stone: shell-like surface echo, pronounced posterior shadowing, inhomogeneous intrinsic echo pattern.
c Typical gallstone with the patient supine: bright echo of the stone, classic posterior shadowing.
f Mixed pigment gallstone: inhomogeneous intrinsic echo pattern with black voids (pigment), soft surface echo, weak posterior shadowing.
g Cholesterol gallstone: intrinsic echo pat- |
h Mixed calcium stones: rather hyper- |
i Mixed pigment gallstone: mixed intrinsic |
tern with tabular structure (with some- |
echoic gallstone dependent in the gall- |
echo pattern (inhomogeneous); stones |
what comet-tail–like artifacts); calculi |
bladder. |
mostly dependent in the gallbladder. |
floating within the lumen of the gallblad- |
|
|
der. |
|
|
Hypoechoic
|
|
|
|
|
Changes in Size |
|
Gallbladder Sludge |
||
Gallbladder |
|||||||||
Wall Changes |
|
Hemobilia |
|||||||
|
|
|
|
|
|
||||
|
|
|
|
|
|
Intraluminal Changes |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
Hyperechoic |
|
|
|
|
|
|
|
|
|
Hypoechoic |
|
|
|
|
|
|
|
|
Nonvisualized Gallbladder |
|
|
||
|
|
|
|
|
|
|
|||
Gallbladder Sludge |
|
|
|||||||
Sludge formation in the gallbladder depends |
der (no posterior shadowing), or the gallblad- |
||||||||
on bile concentration, changes in crystalliza- |
der is filled solid with sluggish floating mate- |
||||||||
tion, and desquamation. The presence of sludge |
rial. Gallbladder sludge is characterized by its |
||||||||
is marked by a hypoechoic layer, or one of |
motility upon repositioning of the patient. De- |
||||||||
mixed echogenicity, at the floor of the gallblad- |
pending on make-up and amount, the types of |
||||||||
sludge in the gallbladder may be differentiated as shown in Table 3.6 and  3.8. Dysfunctional motility or ejection is a precondition.
3.8. Dysfunctional motility or ejection is a precondition.
3
Intraluminal Changes
161
3
Biliary Tree and Gallbladder
Table 3.6 Types of gallbladder sludge |
|
|
|
|
|
Sludge-filled gallbladder |
Polypoid sludge |
Sludge sedimentation |
Floating cholesterol crystals |
Size |
Gallbladder filled, solid |
Varying |
Varying |
Crystalline |
Shape |
Gallbladder filled, solid |
Polypoid, dependent on |
Rather dependent on posi- |
Tabular |
|
|
position |
tion, often layered |
|
Echogenicity |
Varying, sometimes hepatized |
Varying |
Mixed, varying |
Hyperechoic, comet-tail artifacts |
Wall |
Normal |
Normal |
Normal |
Normal |
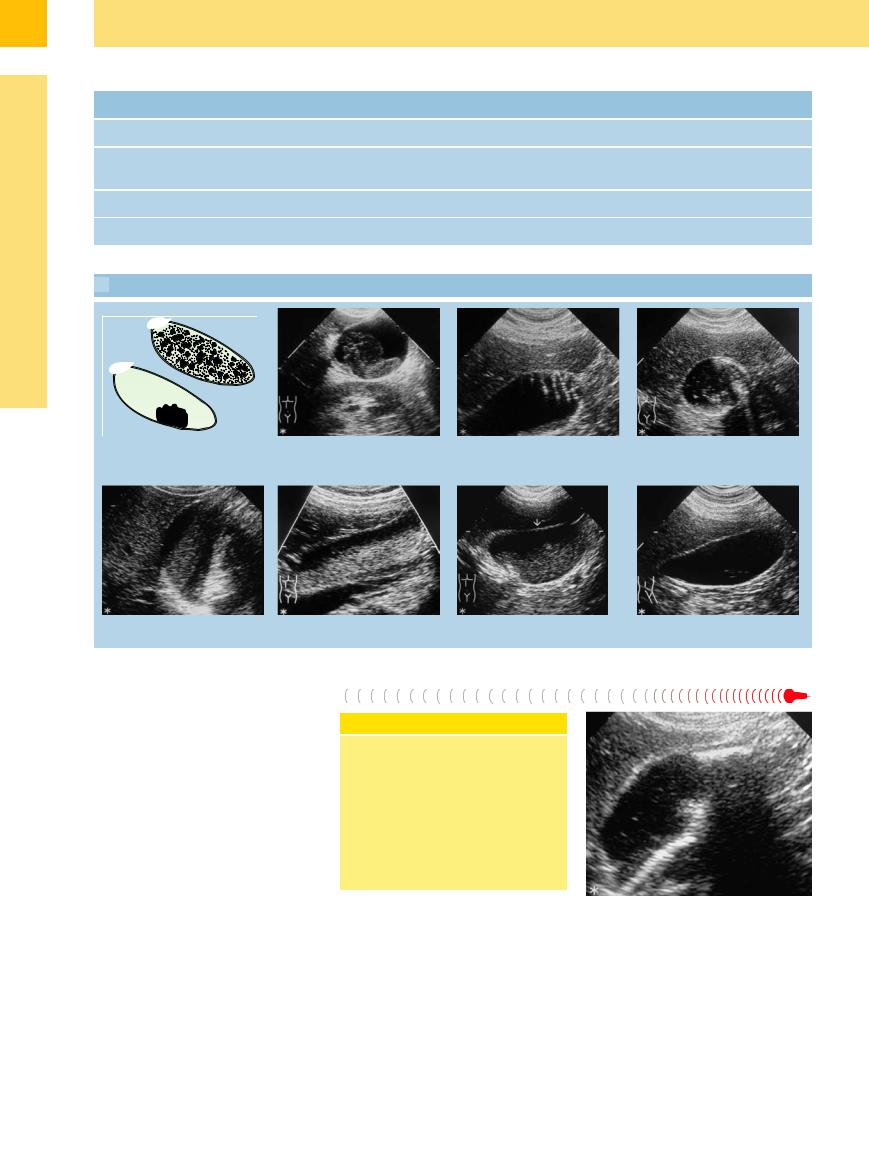
 3.8 Types of Sludge
3.8 Types of Sludge
Floating
a Sludge may float freely or appear as a |
b Polypoid sludge within the gallbladder. |
c Floating sludge: cholesterol tables at the |
d Di use floating sludge: multiple echoes |
“pseudotumor” (modified from Retten- |
|
fundus arranged in rouleau fashion. |
of di erent size and echogenicity. |
Meier and Seitz14). |
|
|
|
e Pseudotumorous sludge in the center of f and g Nearly completely sludge-filled gallbladder: homogeneous hyperechoic sludge. h Floating cholesterol crystals. the gallbladder.
Hemobilia 












Hemobilia is a well-known complication of tumor or, less commonly, inflammatory and traumatic gallbladder lesions. A fresh clot within the gallbladder may mimic hypoechoic sludge. Older traumatic clots adherent to the wall will display as hyperechoic mass (Fig. 3.66). During anticoagulation and known gallbladder disease hemobilia must be considered in the case of an obscure anemia.
Conclusion
These findings demonstrate the enormous capabilities offered by a subtle ultrasound study in the differential diagnosis of gallbladder disease. Ultrasound is the diagnostic modality of choice in all disorders of the gallbladder, since its resolution is much better than that of all the other modalities. Therefore, sonography is the linchpin in the diagnostic work-up of the gallbladder.
Fig. 3.66 Hemobilia in the fundus of the gallbladder, trau- matic-related hemorrhage, spontaneous resolution within 4 weeks.
162