

- •Contents
- •Preface
- •Contributors
- •1 Vessels
- •1.1 Aorta, Vena Cava, and Peripheral Vessels
- •Aorta, Arteries
- •Anomalies and Variant Positions
- •Dilatation
- •Stenosis
- •Wall Thickening
- •Intraluminal Mass
- •Perivascular Mass
- •Vena Cava, Veins
- •Anomalies
- •Dilatation
- •Intraluminal Mass
- •Compression, Infiltration
- •1.2 Portal Vein and Its Tributaries
- •Enlarged Lumen Diameter
- •Portal Hypertension
- •Intraluminal Mass
- •Thrombosis
- •Tumor
- •2 Liver
- •Enlarged Liver
- •Small Liver
- •Homogeneous Hypoechoic Texture
- •Homogeneous Hyperechoic Texture
- •Regionally Inhomogeneous Texture
- •Diffuse Inhomogeneous Texture
- •Anechoic Masses
- •Hypoechoic Masses
- •Isoechoic Masses
- •Hyperechoic Masses
- •Echogenic Masses
- •Irregular Masses
- •Differential Diagnosis of Focal Lesions
- •Diagnostic Methods
- •Suspected Diagnosis
- •3 Biliary Tree and Gallbladder
- •3.1 Biliary Tree
- •Thickening of the Bile Duct Wall
- •Localized and Diffuse
- •Bile Duct Rarefaction
- •Localized and Diffuse
- •Bile Duct Dilatation and Intraductal Pressure
- •Intrahepatic
- •Hilar and Prepancreatic
- •Intrapancreatic
- •Papillary
- •Abnormal Intraluminal Bile Duct Findings
- •Foreign Body
- •The Seven Most Important Questions
- •3.2 Gallbladder
- •Changes in Size
- •Large Gallbladder
- •Small/Missing Gallbladder
- •Wall Changes
- •General Hypoechogenicity
- •General Hyperechogenicity
- •General Tumor
- •Focal Tumor
- •Intraluminal Changes
- •Hyperechoic
- •Hypoechoic
- •Nonvisualized Gallbladder
- •Missing Gallbladder
- •Obscured Gallbladder
- •4 Pancreas
- •Diffuse Pancreatic Change
- •Large Pancreas
- •Small Pancreas
- •Hypoechoic Texture
- •Hyperechoic Texture
- •Focal Changes
- •Anechoic Lesion
- •Hypoechoic Lesion
- •Isoechoic Lesion
- •Hyperechoic Lesion
- •Irregular (Complex Structured) Lesion
- •Dilatation of the Pancreatic Duct
- •Marginal/Mild Dilatation
- •Marked Dilatation
- •5 Spleen
- •Nonfocal Changes of the Spleen
- •Diffuse Parenchymal Changes
- •Large Spleen
- •Small Spleen
- •Focal Changes of the Spleen
- •Anechoic Mass
- •Hypoechoic Mass
- •Hyperechoic Mass
- •Splenic Calcification
- •6 Lymph Nodes
- •Peripheral Lymph Nodes
- •Head/Neck
- •Extremities (Axilla, Groin)
- •Abdominal Lymph Nodes
- •Porta Hepatis
- •Splenic Hilum
- •Mesentery (Celiac, Upper and Lower Mesenteric Station)
- •Stomach
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •Small/Large Intestine
- •Focal Wall Changes
- •Extended Wall Changes
- •Dilated Lumen
- •Narrowed Lumen
- •8 Peritoneal Cavity
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Anechoic Structure
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Wall Structures
- •Smooth Margin
- •Irregular Margin
- •Intragastric Processes
- •Intraintestinal Processes
- •9 Kidneys
- •Anomalies, Malformations
- •Aplasia, Hypoplasia
- •Cystic Malformation
- •Anomalies of Number, Position, or Rotation
- •Fusion Anomaly
- •Anomalies of the Renal Calices
- •Vascular Anomaly
- •Diffuse Changes
- •Large Kidneys
- •Small Kidneys
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Irregular Structure
- •Circumscribed Changes
- •Anechoic Structure
- •Hypoechoic or Isoechoic Structure
- •Complex Structure
- •Hyperechoic Structure
- •10 Adrenal Glands
- •Enlargement
- •Anechoic Structure
- •Hypoechoic Structure
- •Complex Echo Structure
- •Hyperechoic Structure
- •11 Urinary Tract
- •Malformations
- •Duplication Anomalies
- •Dilatations and Stenoses
- •Dilated Renal Pelvis and Ureter
- •Anechoic
- •Hypoechoic
- •Hypoechoic
- •Hyperechoic
- •Large Bladder
- •Small Bladder
- •Altered Bladder Shape
- •Intracavitary Mass
- •Hypoechoic
- •Hyperechoic
- •Echogenic
- •Wall Changes
- •Diffuse Wall Thickening
- •Circumscribed Wall Thickening
- •Concavities and Convexities
- •12.1 The Prostate
- •Enlarged Prostate
- •Regular
- •Irregular
- •Small Prostate
- •Regular
- •Echogenic
- •Circumscribed Lesion
- •Anechoic
- •Hypoechoic
- •Echogenic
- •12.2 Seminal Vesicles
- •Diffuse Change
- •Hypoechoic
- •Circumscribed Change
- •Anechoic
- •Echogenic
- •Irregular
- •12.3 Testis, Epididymis
- •Diffuse Change
- •Enlargement
- •Decreased Size
- •Circumscribed Lesion
- •Anechoic or Hypoechoic
- •Irregular/Echogenic
- •Epididymal Lesion
- •Anechoic
- •Hypoechoic
- •Intrascrotal Mass
- •Anechoic or Hypoechoic
- •Echogenic
- •13 Female Genital Tract
- •Masses
- •Abnormalities of Size or Shape
- •Uterus
- •Abnormalities of Size or Shape
- •Myometrial Changes
- •Intracavitary Changes
- •Endometrial Changes
- •Fallopian Tubes
- •Hypoechoic Mass
- •Anechoic Cystic Mass
- •Solid Echogenic or Nonhomogeneous Mass
- •14 Thyroid Gland
- •Diffuse Changes
- •Enlarged Thyroid Gland
- •Small Thyroid Gland
- •Hypoechoic Structure
- •Hyperechoic Structure
- •Circumscribed Changes
- •Anechoic
- •Hypoechoic
- •Isoechoic
- •Hyperechoic
- •Irregular
- •Differential Diagnosis of Hyperthyroidism
- •Types of Autonomy
- •15 Pleura and Chest Wall
- •Chest Wall
- •Masses
- •Parietal Pleura
- •Nodular Masses
- •Diffuse Pleural Thickening
- •Pleural Effusion
- •Anechoic Effusion
- •Echogenic Effusion
- •Complex Effusion
- •16 Lung
- •Masses
- •Anechoic Masses
- •Hypoechoic Masses
- •Complex Masses
- •Index
11
Urinary Tract
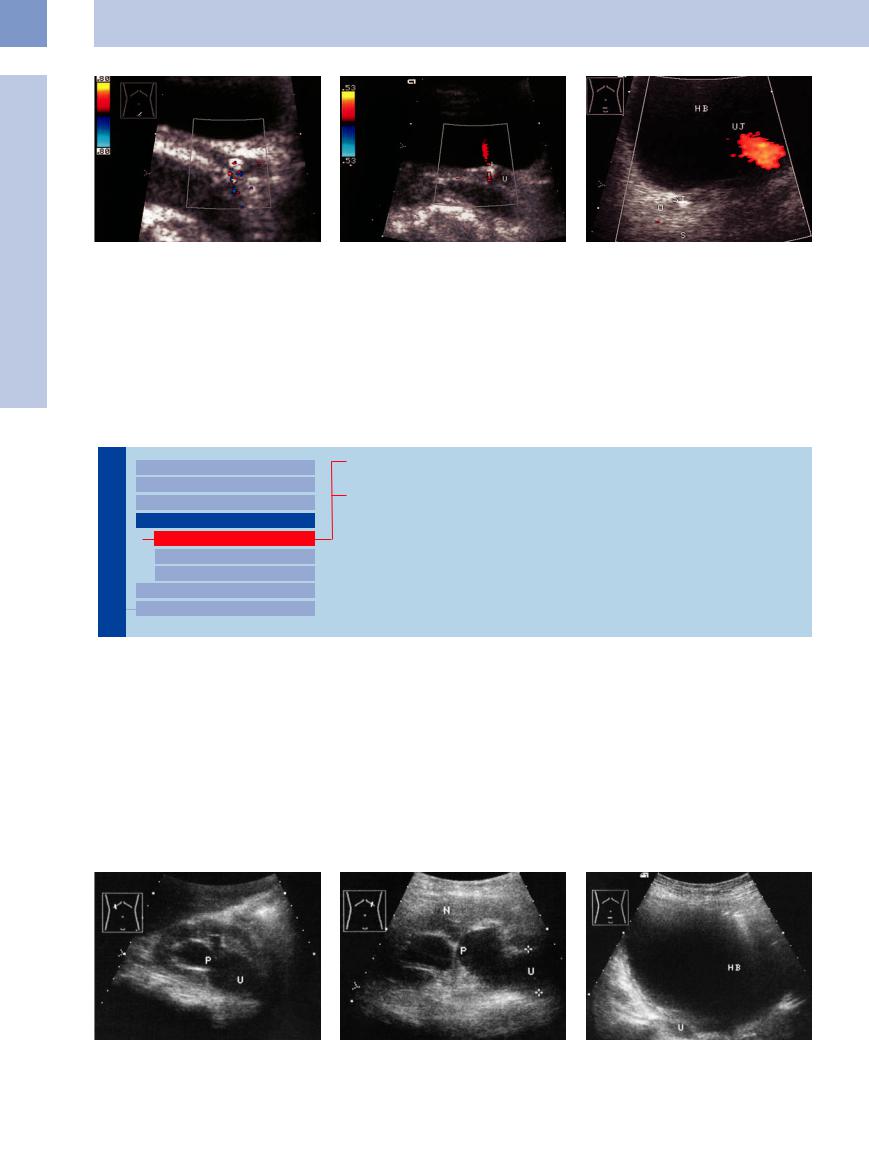
Fig. 11.50 Colic caused by an urinary calculus in the distally slightly dilated ureter; twinkling artifact.
Fig. 11.51 Prevesical stone in the ureteral orifice (U; 4 days later; see Fig. 11.50). Color Doppler: twinkling artifact in the acoustic shadow. Ureteral jet shows a maintained flow into the bladder. The stone was passed spontaneously 1 day later.
Fig. 11.52 Prevesical stone in the right ureter (ST, partial acoustic shadow S), color Doppler view: no ureteral jet on the right side with fluid diuresis, but a conspicuous colorflow jet (UJ) is visible on the left side. HB = bladder.
■ Changes in Bladder Size or Shape
Large Bladder
Urinary Tract

Malformations
Dilated Renal Pelvis and Ureter Renal Pelvic Mass, Ureteral Mass Changes in Bladder Size or Shape
Large Bladder
Small Bladder
Altered Bladder Shape Intracavitary Mass
Wall Changes
Urinary Retention
Overflow Bladder, Neurogenic Bladder
Urinary Retention


















































Urinary retention refers to an inability to empty the bladder. All gradations can occur, from mildly impaired outflow with or without residual urine to total retention. The causes are diverse and include functional and neurogenic causes (detrusor paralysis, as in Parkinson disease) as well as morphological changes (stones, tumors, foreign bodies, infravesical obstructions). Most causes can be detected and iden-
tified on ultrasound (Table 11.3). Idiopathic urinary retention is rare.
Volume estimation. Ultrasound in urinary retention demonstrates an overdistended bladder. The degree of enlargement can be measured by estimating the bladder volume. Normally a bladder volume of 350–450 mL triggers the urge to urinate. The maximum anatomical bladder capacity is 400–600 mL, and patholog-
ical bladder volumes may reach 2 liters or more. The sonographic estimation of bladder volume and residual urine is simple: take the product of the largest longitudinal, transverse, and anteroposterior diameters and divide by 2 (the formula for a rotational ellipsoid). The range of error is relatively large (small volumes are overestimated, large volumes are underestimated), but the formula is quite satisfactory for clinical purposes (Fig.11.53, Fig.11.54).
Fig. 11.53a–c Maximal bladder distension behind a clogged urethral catheter, with secondary reflux into the ureter (U) and renal pelvis (P). N = kidney; HB = bladder.
398
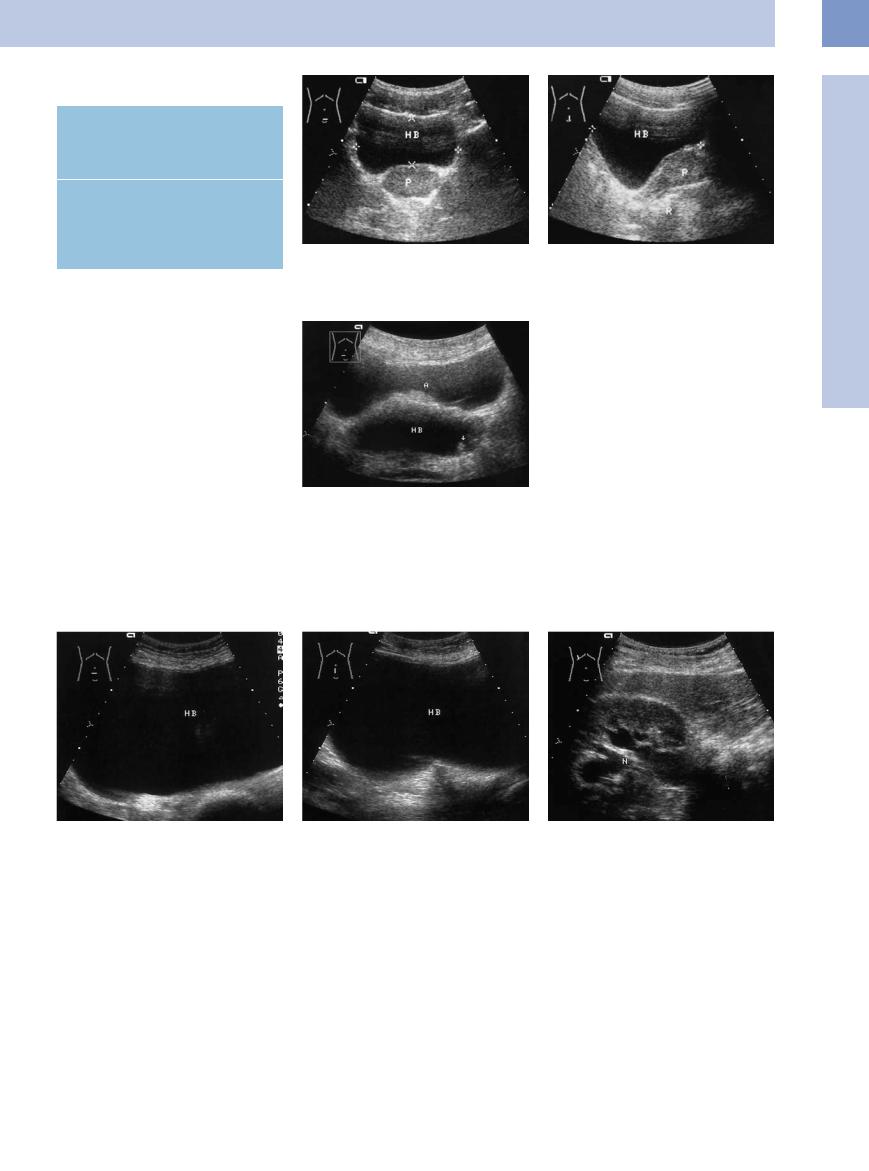
Table 11.3 Vesical and infravesical causes of urinary retention
Vesical causes
●Neurogenic bladder dysfunction
●Bladder neck stones
●Bladder tumors
Infravesical causes
●Prostatic hyperplasia
●Prostatic carcinoma
●Foreign bodies
●Phimosis
Misinterpretation may be caused by paravesical anechoic masses such as ovarian cysts and loculated ascites (Fig.11.55).
Fig. 11.54 Measurement of bladder volume in a full bladder (HB).
a Lower abdominal transverse scan: width × depth (cursors).
b Lower abdominal longitudinal scan: greatest length (cursors). P = normal prostate; R = rectum.
Fig. 11.55 Ascites in the lower abdomen (A) assuming the shape of the bladder. The actual bladder (HB) can be positively identified as such only by scanning it after voiding and when distended (if necessary, by retrograde filling). A small papillomatous bladder tumor is noted as an incidental finding (arrow).
11
Changes in Bladder Size or Shape
Overflow Bladder,
Bladder, Neurogenic
Neurogenic  Bladder
Bladder 






































Overflow bladder and neurogenic bladder are types of urine storage disorders. Their clinical hallmarks are frequent micturition, nycturia, and incontinence. Neurogenic bladder is diag-
nosed by exclusion and is classified on the basis of clinical findings.
The ultrasound appearance corresponds to that of urinary retention (Fig.11.56).
Fig. 11.56 a and b Maximally filled bladder (HB), transverse and longitudinal scan direction. Volume (measured in US) 1482 mL.
b Dilated pelvis. Clinically: long-standing diabetes; autonomic neuropathy?
399
11
Urinary Tract
Small Bladder
Tract |
Malformations |
|||||
|
|
|
||||
|
|
|
Dilated Renal Pelvis and Ureter |
|||
|
|
|
||||
|
|
|
Renal Pelvic Mass, Ureteral Mass |
|||
Urinary |
||||||
Changes in Bladder Size or Shape |
||||||
|
|
|
||||
|
|
|
|
|
Large Bladder |
|
|
|
|
|
|||
|
|
|
|
|
Small Bladder |
|
|
|
|
|
|
||
|
|
|
|
|
Altered Bladder Shape |
|
|
|
|
|
|
||
|
|
|
Intracavitary Mass |
|||
|
|
|
Wall Changes |
|||
|
|
|
||||
Empty Bladder
Residual Urine
Shrunken Bladder
Empty Bladder
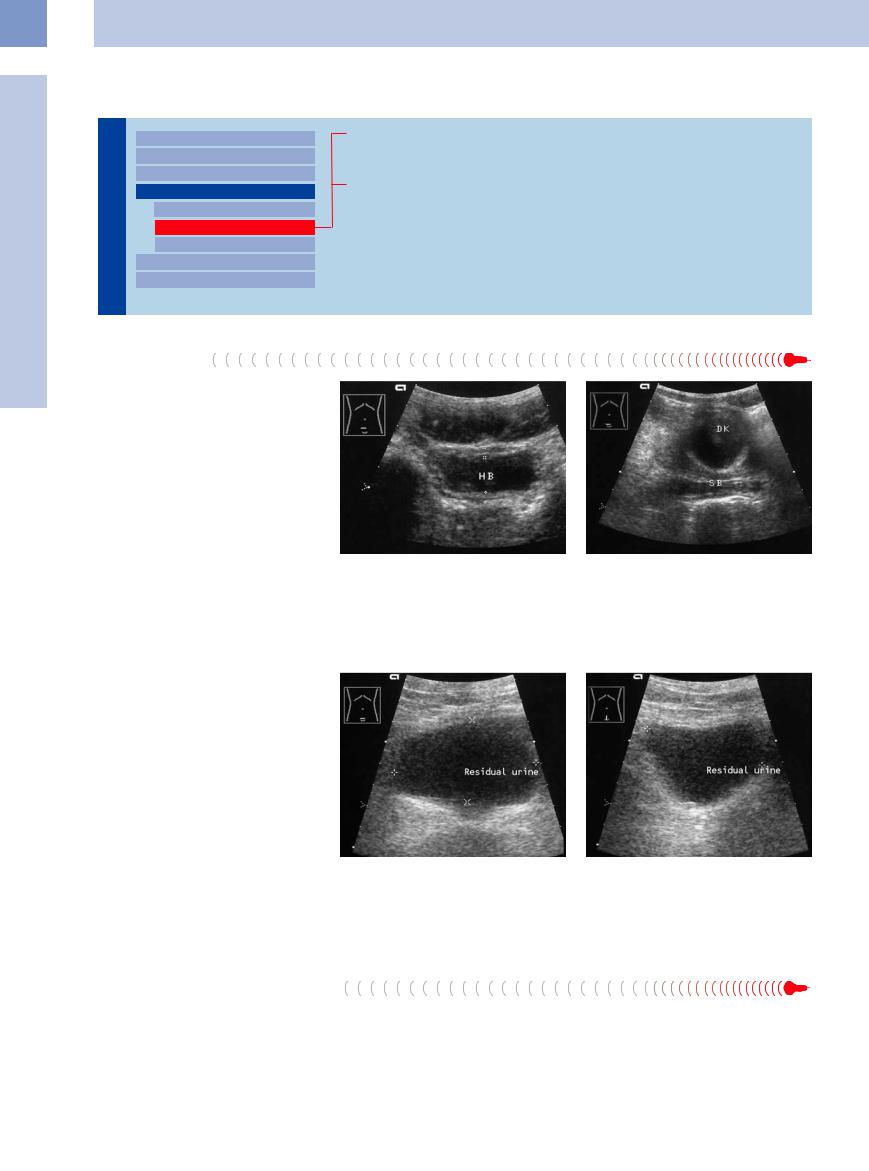
When the bladder is in an empty or almost empty state, its roof sags, giving it a bowlshaped appearance at ultrasound. Asking the patient when he or she last voided can explain a “small bladder” in doubtful cases and exclude inflammatory shrinkage (Fig.11.57, Fig.11.58).
Fig. 11.57 Almost empty bladder (HB) in a lower abdomi- |
Fig. 11.58 Completely empty bladder. A lumen is no lon- |
nal transverse scan. Here the bladder wall appears thick- |
ger visualized. The bladder location is indicated by an |
ened (5 mm between cursors). |
indwelling balloon catheter (DK). SB = seminal vesicle. |
Residual Urine




















































The presence of residual urine, which can be misinterpreted as a small bladder, is demonstrated by imaging the bladder in the distended state and immediately after voiding. The volume formula is used to calculate volume (Fig.11.59). Normally no residual urine is found. Small amounts (< 15 mL) are not clinically significant in older adults.
Fig. 11.59 |
b Lower abdominal longitudinal scan to determine the |
a Residual urine after complete voiding, in this case |
craniocaudal diameter. |
68.6 mL. Lower abdominal transverse scan to determine |
|
the transverse and anteroposterior diameters. |
|
Shrunken Bladder








Unlike a partially emptied bladder, a shrunken |
tuberculosis and radiocystitis. The inflamma- |
duration of the wall muscles and a diminished |
bladder exhibits shape and wall changes in |
tory bladder changes in urinary tuberculosis |
bladder capacity (Fig.11.60). |
addition to its small size. The causes are |
start around the ureteral orifices and then |
|
chronic inflammatory disorders such as urinary |
spread deep into the bladder wall, causing in- |
|
400
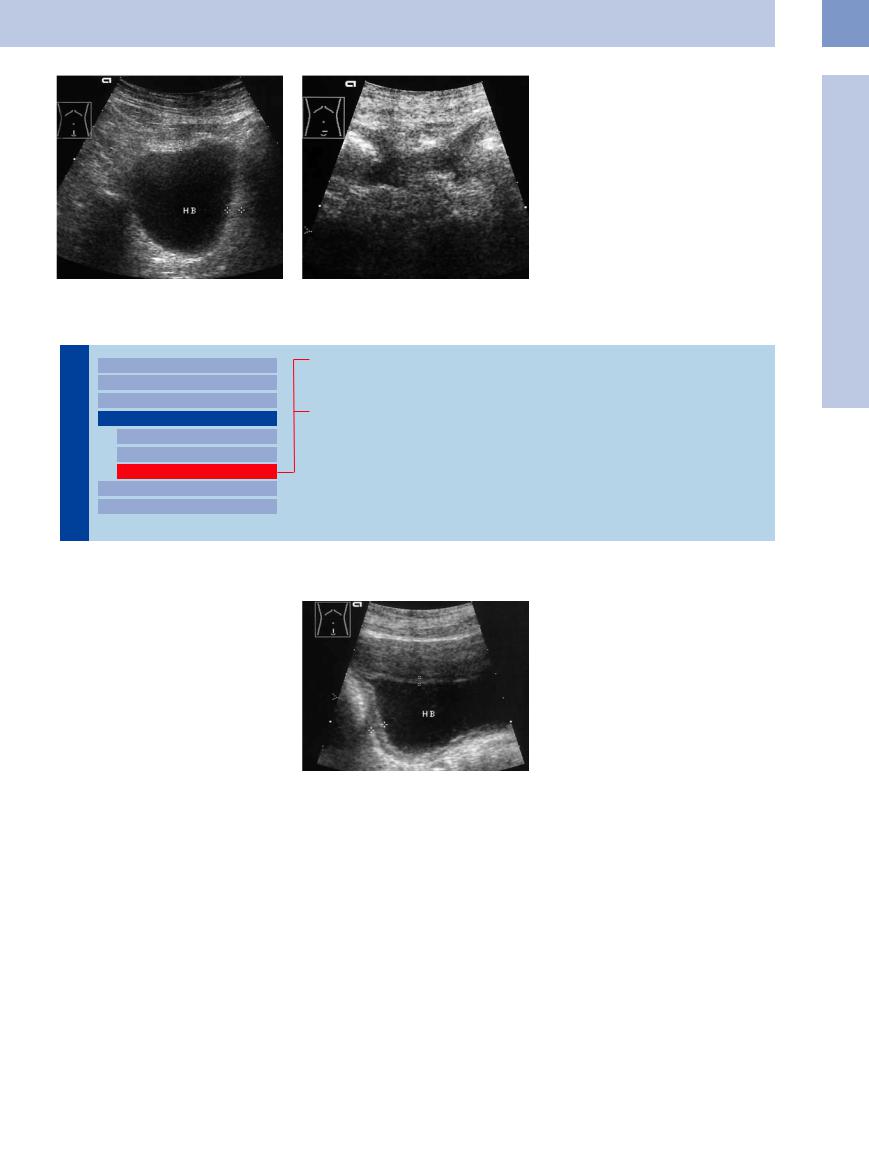
Fig. 11.60 Shrunken bladder.
a After urinary tuberculosis. HB = bladder. Maximum bladder capacity is 153 mL, residual urine volume is 43 mL. Thickened wall (cursors).
b Neurogenic shrunken bladder with reflux. Maximum bladder capacity is 60 mL.
Altered Bladder Shape
Tract |
Malformations |
||||
|
|
|
|||
|
|
|
Dilated Renal Pelvis and Ureter |
||
|
|
|
|||
|
|
|
Renal Pelvic Mass, Ureteral Mass |
||
Urinary |
|||||
Changes in Bladder Size or Shape |
|||||
|
|
|
|||
|
|
|
|
Large Bladder |
|
|
|
|
|
Small Bladder |
|
|
|
|
|
Altered Bladder Shape |
|
|
|
|
|
||
|
|
|
Intracavitary Mass |
||
|
|
|
Wall Changes |
||
|
|
|
|||
Partially Contracted Bladder
Diverticulum, Pseudodiverticulum
Indented Bladder, Operated Bladder
Partially Contracted Bladder
Bladder 












































The bladder roof sags during micturition, creating a bowl-shaped lumen with tapered lateral extensions that may be mistaken for diverticula.
An almost empty bladder has a variable ultrasound appearance: crescent-shaped, rounded, or oval. The contracted muscles give the wall an irregular border and increase its thickness to as much as 6–8 mm. A wall thickness greater than 10 mm is definitely abnormal (Fig.11.57, Fig.11.61).
Fig. 11.61 Partially contracted bladder (HB) with apparent wall thickening due to the contracted muscles (cursors). The three-part wall structure is clearly visualized.
Diverticulum, Pseudodiverticulum









































Multiple pseudodiverticula resulting from a |
bladder that is difficult to recognize sono- |
full or partially empty state or by imaging the |
subvesical obstruction (benign prostatic hyper- |
graphically as having a diverticular cause. The |
bladder in different planes (Fig.11.62, |
plasia, BPH) or large diverticula without a dis- |
correct diagnosis can usually be made, how- |
Fig.11.63). |
tinct neck can impart a bizarre shape to the |
ever, by examining the bladder in a partially |
|
11
Changes in Bladder Size or Shape
401