

44. Nasal Reconstruction Using Bone Grafts and Rigid Internal Fixation |
487 |
|||||||
e |
|
|
|
f |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
g |
|
|
|
|
|
|
|
h |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
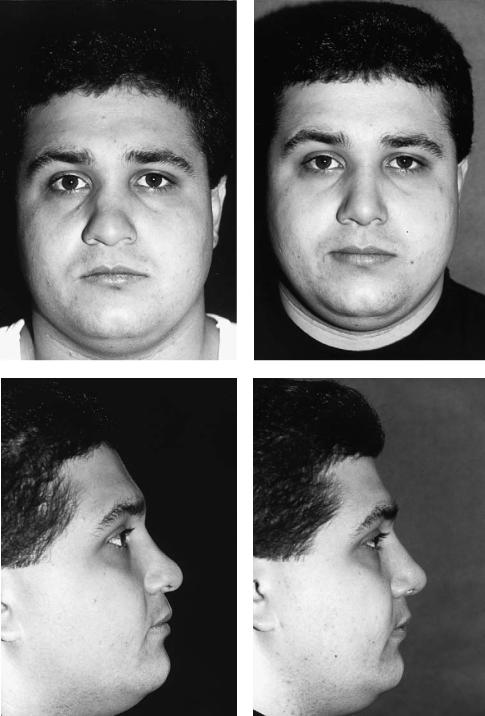
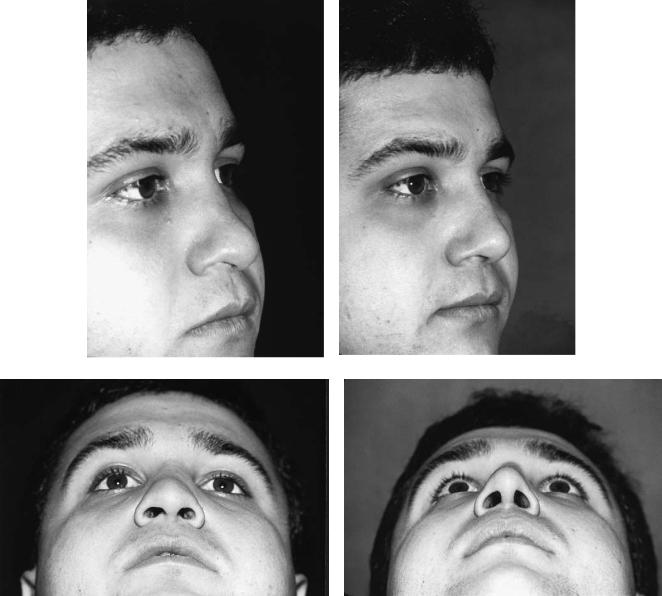
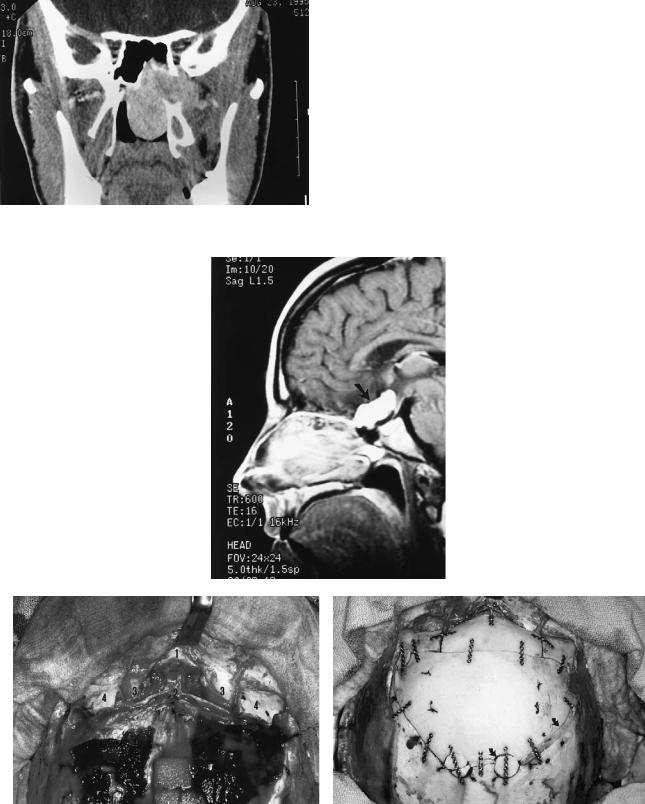
FIGURE 44.3 Continued.


496 |
|
R.B. Stanley, Jr. |
|
Transorbitozygomatic |
ative edema to further facilitate the approaches, and their |
||
This is a combined osteoplastic-free-segment approach |
short-term administration does not appear to increase the risk |
||
of infection, even with the transoral approaches. An attempt |
|||
through the temporal fossa. It necessitates complete exposure |
should be made to obtain a watertight suture closure of dural |
||
of the lateral orbit, body of zygoma, and zygomatic arch |
and mucosal incisions. However, this may not always be pos- |
||
through an extended hemicoronal dissection. This dissection |
sible at sites deep within the intracranial cavity or high in the |
||
must be maintained at a level deep to the superficial layer of |
nasopharynx. Short-term augmentation of a tenuous closure |
||
the deep temporal fascia to avoid damage to the frontal branch |
of either suture line can be obtained with fibrin adhesive, and |
||
of the facial nerve. Two osteotomies through the arch, one |
pressure from cerebrospinal fluid on the dural closure can be |
||
placed obliquely through the articular eminence and one |
reduced with lumbar drainage for a 3- to 5-day period. Ali- |
||
placed paralleling the lateral margin of the orbital rim (Fig- |
mentation should be given by way of a small-diameter, soft |
||
ure 45.7b), allow for lateral and inferior retraction of the arch |
nasogastric feeding tube also for a 3- to 5-day period in pa- |
||
without the need for detachment of the masseter muscle. This |
tients who undergo transoral approaches. An orogastric tube, |
||
prevents the inferior retraction of the muscle and the resul- |
which is somewhat more uncomfortable for the patient, or pe- |
||
tant transcutaneous accentuation of the arch outline that oc- |
ripheral intravenous alimentation can be used if there is con- |
||
curs when the arch is removed and replaced as a free seg- |
cern regarding the presence of a tube in close proximity to a |
||
ment. The body of the zygoma is then removed as a free |
nasopharyngeal repair. A tracheostomy should not be neces- |
||
segment by first detaching the temporalis muscle from the lat- |
sary except in patients who undergo a midline labio- |
||
eral orbit and temporal fossa, and then creating two additional |
mandibular glossotomy or in patients who will likely have |
||
osteotomies (Figure 45.7b). One osteotomy extends through |
airway or aspiration problems related to postoperative lower |
||
the body of the zygoma into the lateral end of the inferior or- |
cranial nerve palsies caused by the neurosurgical portion of |
||
bital fissure, and the other extends from the lateral end of the |
the case. |
||
fissure superiorly along the zygomaticosphenoid suture line |
|
|
|
to pass obliquely through the base of the zygomatic process |
Acknowledgments. The author would like to thank H. Richard |
||
of the frontal bone. When used in conjunction with a tempo- |
Winn, M.D., Professor and Chairman, and M. Sean Grady, |
||
ral craniotomy, increased exposure of the junction of the tem- |
M.D., Associate Professor, of the Department of Neurologi- |
||
poral fossa and infratemporal fossa, posterior orbit, middle |
cal Surgery, University of Washington School of Medicine, |
||
cranial fossa, parasellar area, and interpenduncular fossa is |
Seattle, WA, for the opportunity to participate in the care of |
||
obtained. |
their patients. |
||
Following completion of the neurosurgical procedure, the |
|||
|
|
||
posterior orbit is reconstructed as necessary with split cranial |
References |
||
bone grafts, and the zygoma and zygomatic arch are reposi- |
|||
tioned and stabilized (Figure 45.7c). The osteotomy gaps |
1. |
Archer DJ, Young S, Utley D. Basilar aneurysms: a new trans- |
|
through the body of the zygoma and the anterior arch are |
|
clival approach via maxillotomy. J Neurosurg. 1987;67:54–58. |
|
closed and stabilized with 1.0- or 1.3-mm plates and screws. |
|
||
2. |
Grime PD, Haskell R, Robertson I, Gullan R. Transfacial access |
||
The oblique osteotomies through the zygomatic process of the |
|
of neurosurgical procedures. I. The upper cervical spine and |
|
frontal bone and the articular eminence of the arch, which act |
|
clivus. Int J Oral Maxillofac Surg. 1991;20:285–290. |
|
as sliding osteotomies due to closure of the other gaps, can |
3. Sasaki CT, Lowlicht RA, Astrachan DI, Friedman CD, Goodwin |
||
be stabilized with plates or with lag screws. The temporalis |
|
WJ, Morales M. LeFort I osteotomy approach to skull base. |
|
muscle must be firmly reattached to the lateral orbital rim and |
|
Laryngoscope. 1990;100:1073–1076. |
|
superior temporal line if temporal hollowing is to be avoided. |
4. |
Raveh J, Vuillemin T. The subcranial-supraorbital and temporal |
|
Additionally, bone grafting to the floor of the temporal fossa |
|
approach for tumor resection. J Craniofac Surg. 1990;1:53–59. |
|
5. Shekahr LN, Nanda A, Sen CN, Snyderman CN, Janecka IP. The |
|||
should be considered to help maintain overlying soft tissue |
|||
contours. |
|
extended frontal approach to tumors of the anterior, middle, and |
|
|
posterior skull base. J Neurosurg. 1992;76:198–206. |
||
|
|
||
|
6. Grime PD, Haskall R, Robertson I, Gullan R. Transfacial access |
||
Miscellaneous Considerations |
|
for neurosurgical procedures. II. Middle cranial fossa, infratem- |
|
|
poral fossa, and pterygoid space. Int J Oral Maxillofac Surg. |
||
|
|
1991;20:291–295. |
|
A broad-spectrum antibiotic, typically a cephalosporin, is ad- |
7. Alaywan M, Sindou M. Fronto-temporal approach with orbito- |
||
ministered to all patients preoperatively and continued for 72 |
|
zygomatic removal. Acta Reconstr Surg. 1992;87:362–364. |
|
8. Hale RG, Timmis DP, Bays RA. A new mandibulotomy tech- |
|||
hours postoperatively. For transoral procedures that include |
|
nique for the dentate patient. Plast Reconstr Surg. 1991;87:362– |
|
exposure of the dura, metronidazole is added. A steroid bo- |
|
||
|
364. |
||
lus, usually 12 mg of dexamethasome, is also given preoper- |
|
||
9. |
Janes D, Crockard HA. Surgical access to the base of skull and |
||
atively, and doses of 6 mg are continued every 6 hours for 24 |
|
upper cervical spine by extended maxillotomy. Neurosurgery. |
|
hours postoperatively. The steroids greatly reduce intraoper- |
|
1991;29:411–416. |
|
Section V
Craniomaxillofacial Corrective
Bone Surgery