32. Condylar Prosthesis for the Replacement of the Mandibular Condyle |
375 |
|
a |
|
Occlusal problems have been observed, especially in se- |
|
vere trauma cases. In one patient, this problem developed be- |
|
|
cause regular treatment in due time with correct intermaxil- |
|
|
lar fixation was impossible as a result of the patient’s unstable |
|
|
general condition and paraplegia. Her accident occurred in |
|
|
1985, when immediate repair and stabilization of all facial |
|
|
fractures with plates was not yet a routine procedure. Her fa- |
|
|
cial structure would, without doubt, be much better today with |
|
|
the appropriate application of our treatment protocol for pan- |
|
|
facial fractures. |
|
|
|
Scars were problematic in only one young patient who de- |
|
veloped a broad hypertrophic scar. He had several interven- |
|
|
tions through his scar because of a laceration of his facial |
|
|
nerve (as a result of an accident) together with a severe frac- |
|
|
ture of his mandible. |
|
|
|
In most of our patients with ankylosis, considerable im- |
|
provement was achieved. Two patients with three prostheses |
|
b |
experienced occasional spontaneous locking with pain, which |
|
|
subsided after appropriate pain medication. In all patients, the |
|
|
range of motion with postoperative exercise was considerably |
|
|
improved. One patient felt some discomfort when it was very |
|
|
cold outside. In all instances, only rotational—and almost no |
|
|
gliding—movements were possible in the area of the artifi- |
|
|
cial joint. |
|
|
|
In all patients with wide resections because of tumor inva- |
|
sion and reconstruction with a long plate with a condyle, func- |
|
|
tion was better than in those patients with a condylar pros- |
|
|
thesis alone (Figure 32.6). This is remarkable, especially in |
|
|
view of the fact that placement of the artificial condyle in |
|
|
these instances is less accurate than for the patients with only |
|
|
the condylar prosthesis. |
|
Radiology
|
We observed no screw loosening. On PA views the position- |
|
|
ing of the prosthesis was correct in 50% of the cases. In 40% |
|
c |
of the patients, the artificial condyle was placed laterally and |
|
in 10% dislocation was observed. In 53% of the cases, appo- |
||
|
||
|
sitional bone deposition around the head of the prosthesis oc- |
|
|
curred. To a certain degree this leads to a limitation of mo- |
|
|
tion (Figure 32.7). |
|
|
In two patients with bilateral prostheses, bony resorption |
|
|
cranially from the condyle was seen without perforation of |
|
|
the middle cranial fossa. Only the two prostheses placed in |
|
d |
1974 and 1975 were positioned slightly too high. |
|
|
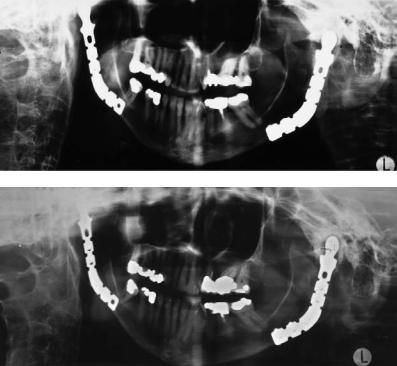
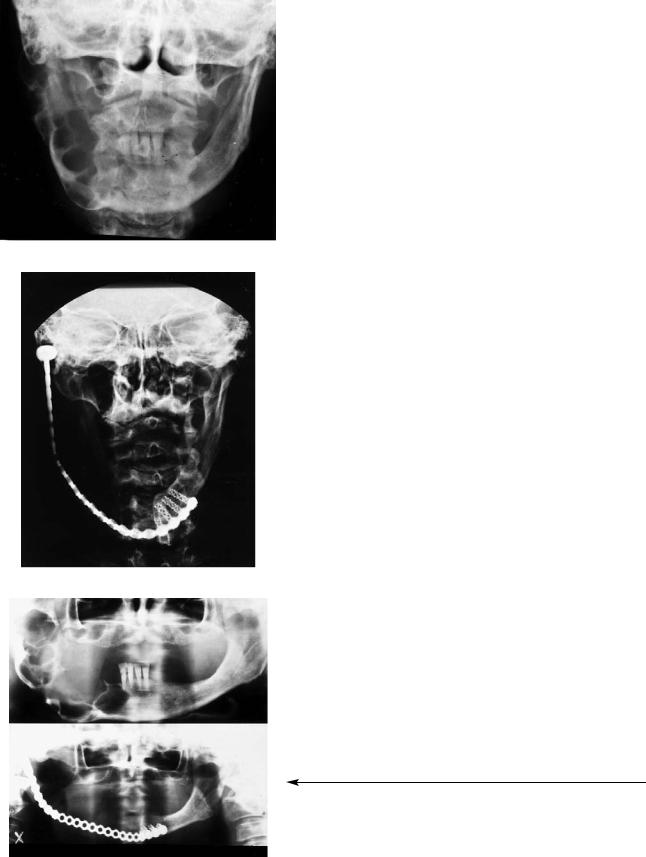
FIGURE 32.6 AP views (a) preoperatively and (b) postoperatively after resection of an extensive ameloblastoma. (c) Preoperative and (d) postoperative panoramic radiographs of the same patient. Surgery was done in 1984. The patient refused a bony reconstruction. The plate has been in place since 1984.