


22 Heart
STUDYAIMS
At the end of your study, you should be able to:
Identifythe pericardium and its relationships
Know the layers of the pericardium
Understand the surface projection of the heart and its chambers
Know the internal features of the atria and ventricles
Understand coronarycirculation
Know the innervation and conduction system of the heart
158 / 425
GUIDES
Thorax: Heart
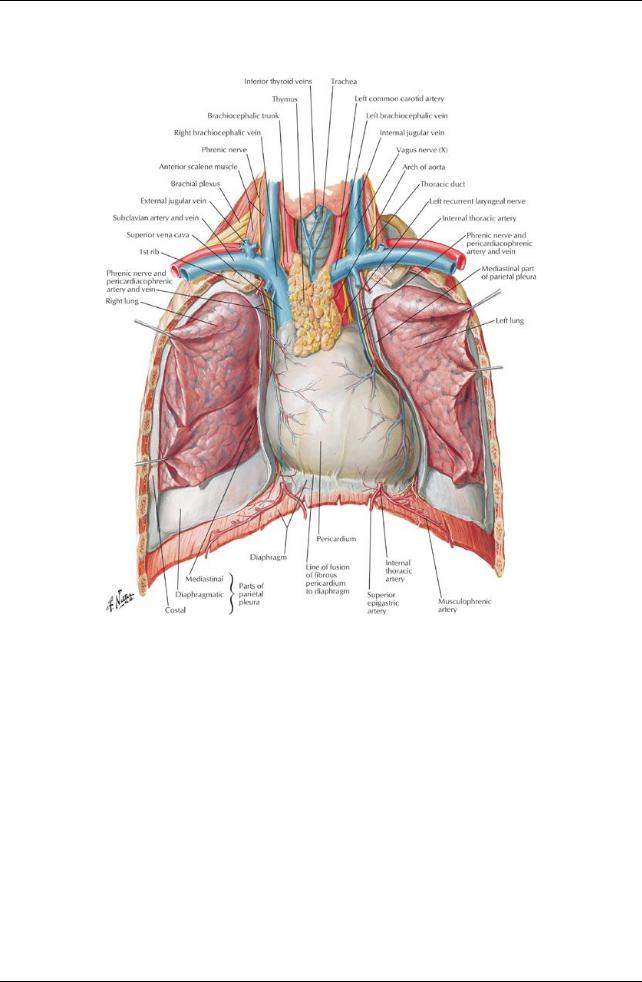
[Plate 205, Heart in Situ]
159 / 425
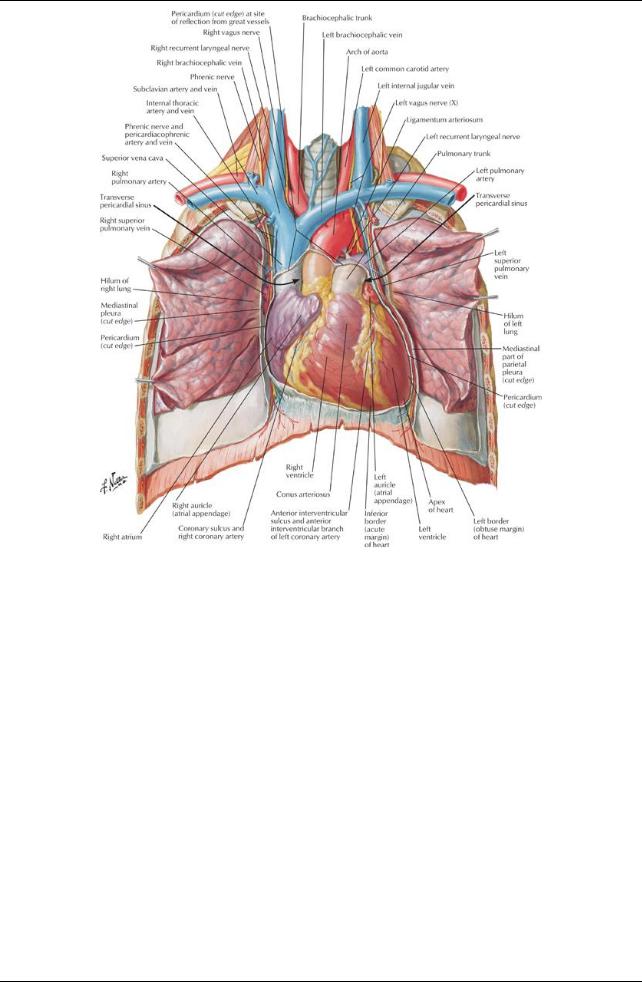
[Plate 206, Heart: Anterior Exposure]
Pericardium
160 / 425
[Plate 209, Pericardial Sac]
The pericardium is a double-layered sac that encloses the heart and the roots of the great vessels. The fibrous outer layer of the pericardium (the fibrous pericardium) consists of dense connective tissue.
The fibrous pericardium is attached to the central tendon of the diaphragm bythe pericardiacophrenic ligament.
It blends with the tunica adventitia of the vessels entering and leaving the heart.
It has ligamentous attachments to the sternum
It is thus affected bymovements of the heart, the great vessels, the sternum, and the diaphragm.
It protects the heart against overfilling because it is fibrous and unyielding
The inner layer of the pericardium is a serous membrane that lines the fibrous pericardium: the serous pericardium, also called the parietal pericardium.
The serous pericardium is a mesothelial layer that reflects onto the roots of the great vessels and is continuous over the external surface of the heart, where it is called the epicardium or visceral pericardium.
Between the serous pericardium (parietal pericardium) and the epicardium (visceral pericardium) is a potential space: the pericardial cavity. The pericardial cavitynormallycontains a thin film of fluid that allows the two layers to move over each other without friction or rubbing. There are two sinuses within the pericardial cavity: the transverse sinus and the oblique sinus.
The transverse pericardial sinus runs transverselyin the pericardial sac between the origins of the great vessels: posterior to the ascending aorta and pulmonarytrunk and anterior to the superior vena cava.
The oblique pericardial sinus is a wide recess in the posterior wall of the pericardial sac bounded laterallybythe entrances of the pulmonaryveins and inferiorlybythe orifice of the inferior vena cava.
Blood supplyto the layers of the pericardium is mainlyfrom the pericardiacophrenic vessels, from the internal thoracic arteries and veins. The nerve supplyto the pericardium is from the phrenic nerves, primarilysensoryfibers for pain, and the sympathetic trunks (vasomotor).
page 110 page 111
Heart
The heart is a muscular pump for the propulsion of blood to all parts of the body.
The right side of the heart receives poorlyoxygenated blood from the superior and inferior vena cava and pumps it to the lungs for oxygenation.
The left side of the heart receives oxygenated blood from the lungs via the pulmonaryveins and pumps it to the bodyvia the aorta and its branches.
The heart consists of four chambers: the right and left atria and the right and left ventricles. The chambers of the heart have walls that consist of three layers:
161 / 425
Endocardium: internal layer of endothelium and connective tissue
Myocardium: the middle, thick muscular layer of the heart
Epicardium, or visceral pericardium
The fibrous skeleton of the heart is a framework of dense collagen that encircles the orifices of the four valves (pulmonary, aortic, tricuspid and mitral).
The functions of the fibrous skeleton are:
Maintains the patencyof the atrioventricular valves
Provides a fixed site for the attachment of the leaflets and cusps of the valves
Provides a fixed site for the attachments of the cardiac muscle fibers
 Insulates the atria from the ventricles so that theycan contract independently The cardiac cycle consists of
Insulates the atria from the ventricles so that theycan contract independently The cardiac cycle consists of
Relaxation of the ventricles (diastole) followed by
 Contraction of the ventricles (diastole) Heart sounds heard with a stethoscope:
Contraction of the ventricles (diastole) Heart sounds heard with a stethoscope:
"lub"-blood from the atria fills the ventricles "dub"-ventricles contract and push blood out of the heart
Orientation of the Heart: Border and Surfaces
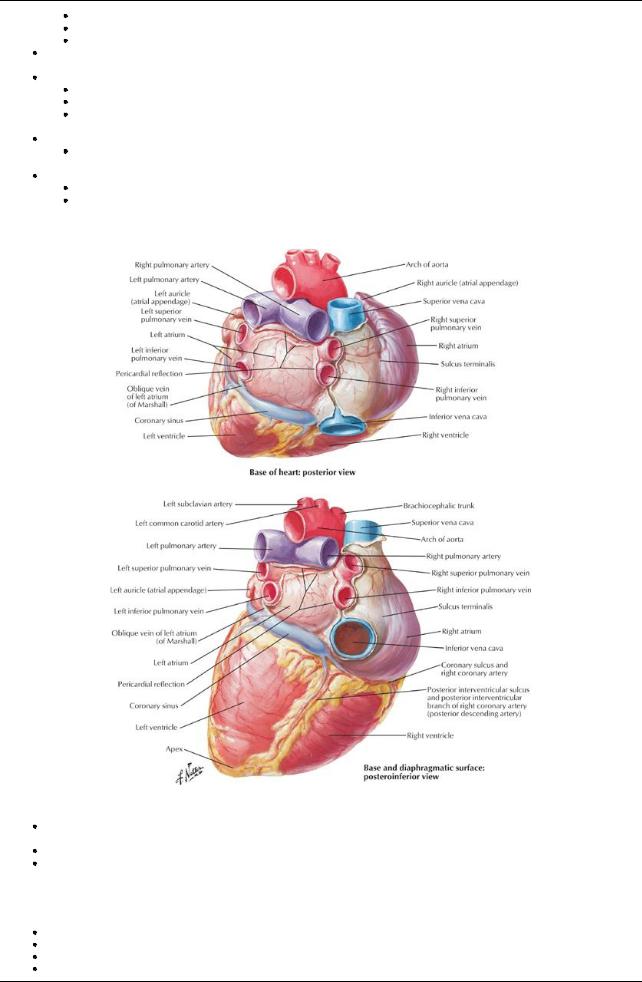
[Plate 208, Heart: Base and Diaphragmatic Surfaces]
The heart lies obliquelybetween the 3rd and the 5th ribs, mainlyon the left side of the midline of the thorax, but with roughlya third of it slightlyto the right.
The base of the heart is its posterior surface, which is the left atrium.
The apexof the heart is formed from the most inferior and lateral part of the left ventricle and lies beneath the left 5th intercostal space at approximatelythe midclavicular line.
Borders
Right border: the right atrium between the superior and inferior vena cavae
Left border: left auricle and left ventricle
Inferior border: mainlyright ventricle with some contribution from the left ventricle
Superior border (anterior view): right and left atria and their auricles
162 / 425
Surfaces (in normal anatomic position)
Anterior (sternocostal): right ventricle
Diaphragmatic (inferior): mainlybythe left ventricle with some contribution bythe right ventricle
Pulmonarysurface (left, filling the cardiac impression in the left lung): left ventricle
Chambers of the Heart
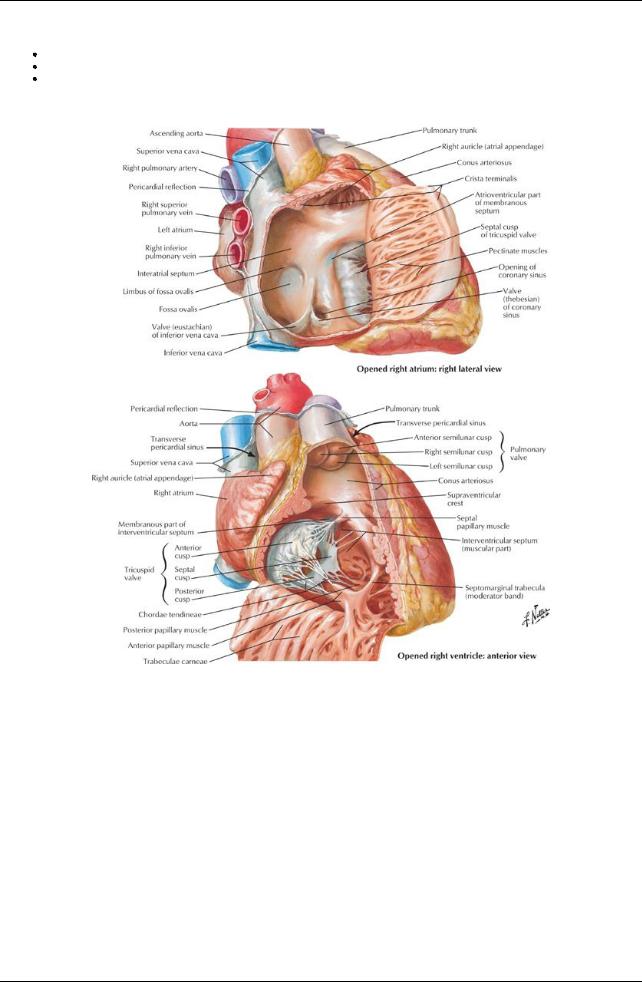
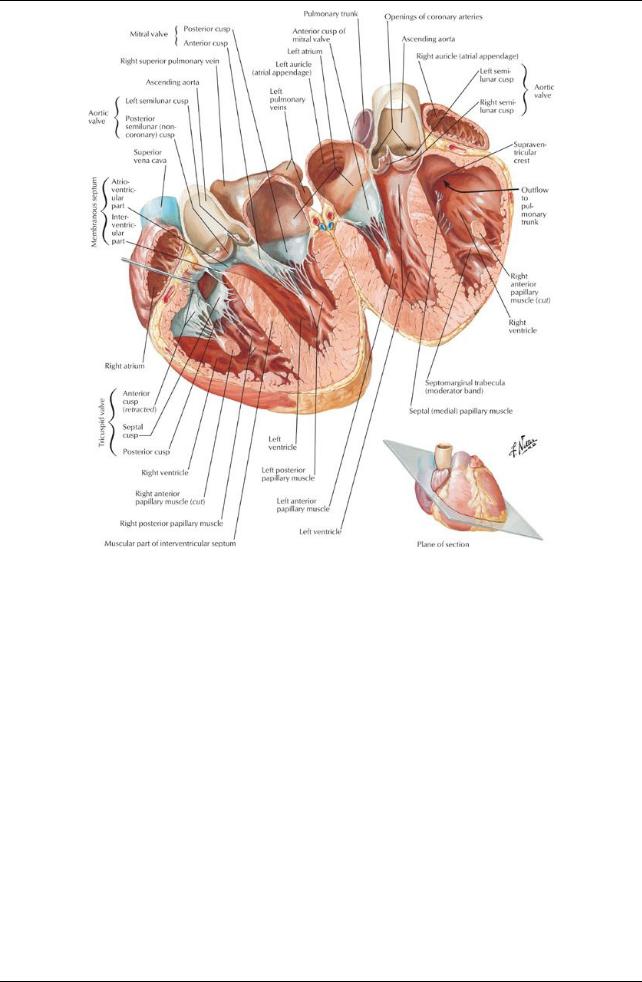
[Plate 214, Right Atrium and Ventricle]
163 / 425
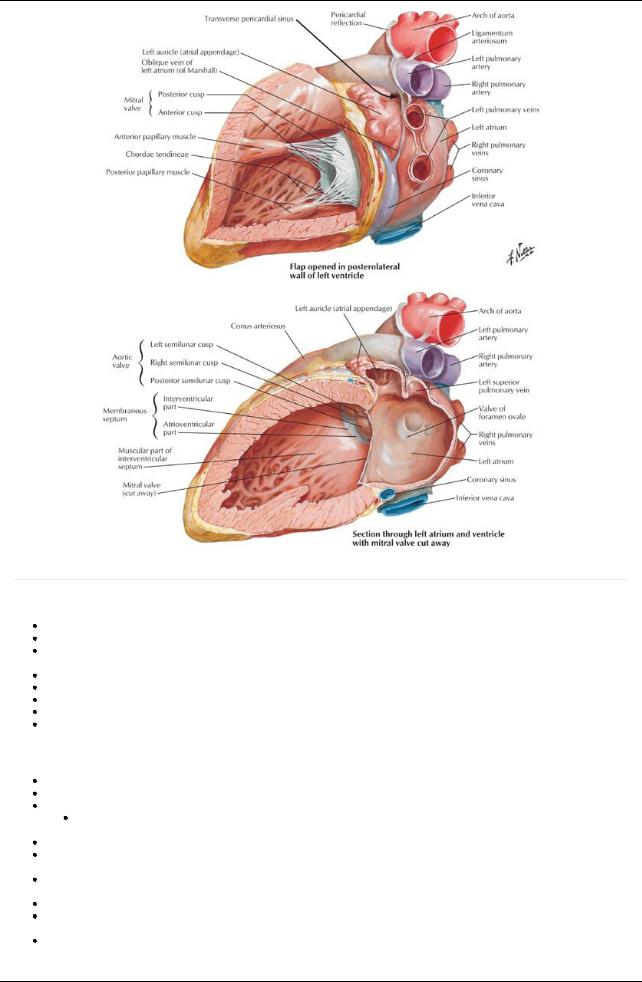
[Plate 215, Left Atrium and Ventricle]
page 111 page 112
Right atrium
The posterior wall of the right atrium is smooth (sinus venarum) and contains the orifices of the superior vena cava and coronarysinus. The anterior wall is ridged with the pectinate muscles.
The smooth and rough parts of the right atrium are separated internallybya smooth ridge, the crista terminalis, which presents externally as shallow groove, the sulcus terminalis.
The superior vena cava opens into the superior aspect of the right atrium.
The inferior vena cava opens into the inferior part, in a direct line with the superior vena cava. An interatrial septum separates the right and left atria.
An oval depression in the interatrial septum, the fossa ovalis, represents the fetal foramen ovale and its valve. Aright atrioventricular (AV) orifice opens into the right ventricle
Right ventricle
The right ventricle is situated in front and to the left of the rightAVorifice. The interior has prominent muscular ridges, the trabeculae carnea. The tricuspid valve or rightAVvalve usuallyconsists of three leaflets.
The bases of the leaflets or cusps are attached to the fibrous ring around the orifice.
 The free edge of each leaflet is attached to two of the three papillarymuscles bytendinous cords (chordae tendinea). The papillarymuscles are three in number: septal, anterior and posterior.
The free edge of each leaflet is attached to two of the three papillarymuscles bytendinous cords (chordae tendinea). The papillarymuscles are three in number: septal, anterior and posterior.
These muscles contract before the ventricle itself contracts, tightening the chordae tendinea and drawing the cusps of the valve together to prevent backflow of blood into the right atrium.
The septomarginal trabecula, or moderator band, is a free band of muscle extending from the interventricular septum to the anterior wall of the ventricle, and it contains Purkinje fibers from the right bundle branch (see conducting system).
The outflow tract of the ventricle is separated from the inflow tract bya smooth crest, the supraventricular crest.
The outflow tract, or conus arteriosus, is smooth walled and leads to the pulmonarytrunk and the valve that guards its orifice, the pulmonary valve.
The pulmonaryvalve has three cusps, which open like pockets to catch regurgitated blood during ventricular diastole
Left Atrium
164 / 425
The left atrium forms the base of the heart.
It has a smooth walled portion from the developmental incorporation of a portion of the pulmonaryveins and an auricular appendage which is ridged with pectinate muscles and which was the primitive left atrium.
Four pulmonaryveins emptyinto the left atrium.
The interatrial septum is nearlytransverse, sloping posteriorlyand to the right The left atrioventricular orifice leads to the left ventricle.
Left Ventricle
page 112 page 113
The left ventricle is nearlytwice as thick as the right ventricle, since it performs more work to circulate blood to the body. It has a conical cavity, the apexof which is the apexof the heart.
Its walls are lined with trabeculae carnea, which are more numerous and not as massive as the ones in the right ventricle.
It contains onlytwo papillarymuscles, anterior and posterior, which both attach to the two leaflets of the left atrioventricular, or mitral, valve via chordae tendinea.
These muscles contract before the ventricle itself contracts, tightening the chordae tendinea and drawing the cusps of the valve together to prevent backflow of blood into the left atrium.
The aortic orifice is located posteriorlyand superiorlyand, like the pulmonaryorifice, is surrounded bya fibrous ring to which the three cusps of the aortic valve are attached.
The aortic valve has three cusps, which open like pockets to catch blood that backflows from the aorta during ventricular diastole. There are dilations in the wall of the aorta beneath each cusp: the aortic sinuses.
The right coronaryarteryoriginates in the right aortic sinus, while the left coronaryarteryoriginates in the left aortic sinus.
Coronary Circulation
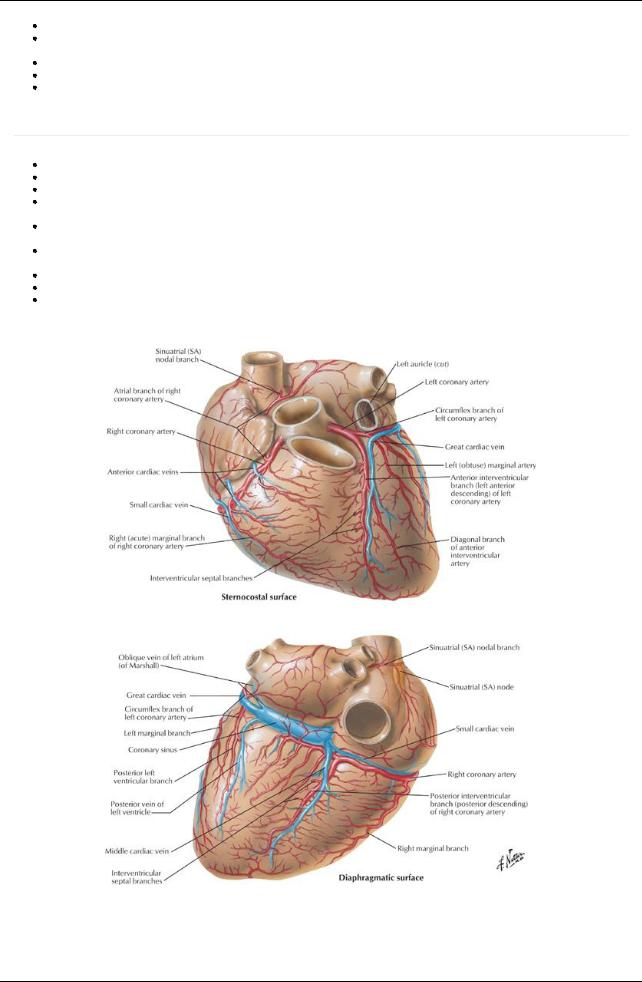
[Plate 211, Coronary Arteries and Cardiac Veins]
165 / 425
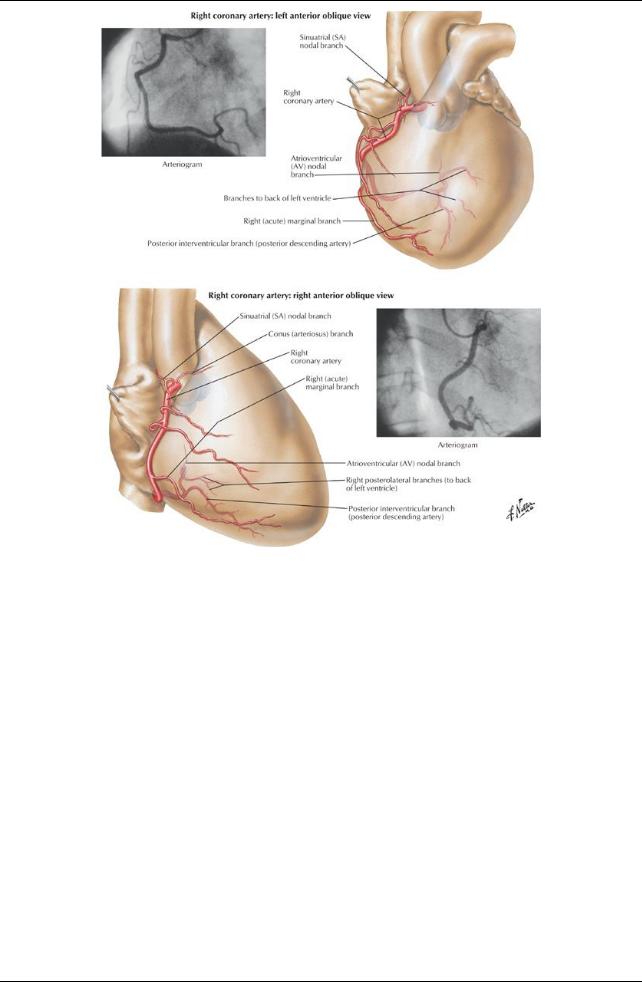
[Plate 212, Coronary Arteries: Arteriographic Views]
166 / 425
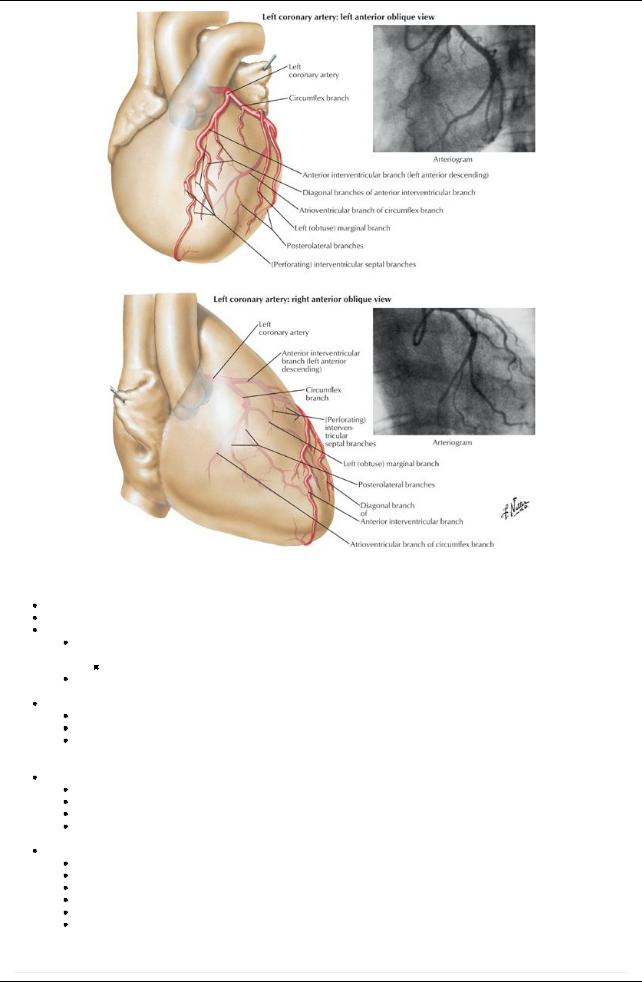
[Plate 213, Coronary Arteries: Arteriographic Views (Continued)]
Arteries
The arterial supplyto the heart is the right and left coronaryarteries, the first branches of the aorta. Theyarise from the corresponding aortic sinuses, just distal to the origin of the aortic valve.
The left coronaryarterypasses between the left auricle and the pulmonarytrunk. Its main branches are
Acircumflexbranch, which reaches the posterior surface of the heart bytraveling in the atrioventricular groove around the left side of the heart
In slightlyless than half of all people, a sinoatrial (SA) nodal branch from the circumflexbranch will supplythe SAnode.
An anterior interventricular branch (left anterior descending arteryor LAD), which descends in the anterior interventricular groove to the apexof the heart and then anastomoses with the posterior interventricular artery.
The right coronaryarteryruns in the atrioventricular groove to the right and around to the posterior surface of the heart. It gives rise to
The SAnodal branch near its origin (in most people)
Aright marginal branch to the right margin of the heart
AnAVnodal branch to the atrioventricular node, as the junction of the septa and four chambers of the heart on the posterior side of the heart
 Aposterior interventricular branch that runs in the posterior interventricular groove. The left coronaryarterysupplies
Aposterior interventricular branch that runs in the posterior interventricular groove. The left coronaryarterysupplies
Left atrium
Most of left ventricle
Some of the right ventricle
Interventricular septum
 SAnode (40% of people) The right coronaryarterysupplies
SAnode (40% of people) The right coronaryarterysupplies
Right atrium
Most of right ventricle
Diaphragmatic surface of left ventricle
Some of the interatrial and interventricular septa
SAnode (60% of people) AVnode
Veins
page 113 page 114
167 / 425

The coronarysinus is a wide vein that runs transverselyacross the posterior surface of the heart in the coronarygroove. The coronarysinus receives blood from
The great cardiac vein that ascends in the anterior interventricular groove and enters the coronarysinus at its left end
The middle cardiac vein (posterior interventricular vein) that ascends in the posterior interventricular groove and enters the coronary sinus at its right end
Small cardiac veins
Left marginal vein
Left posterior ventricular vein(s)
Anterior cardiac veins that enter the right atrium directly
Venae cordial minimae (smallest cardiac veins) that open directlyinto the chambers of the heart
Innervation and Conducting System of the Heart
[Plate 216, Valves and Fibrous Skeleton of Heart]
168 / 425
[Plate 218, Atria, Ventricles and Interventricular Septum]
169 / 425
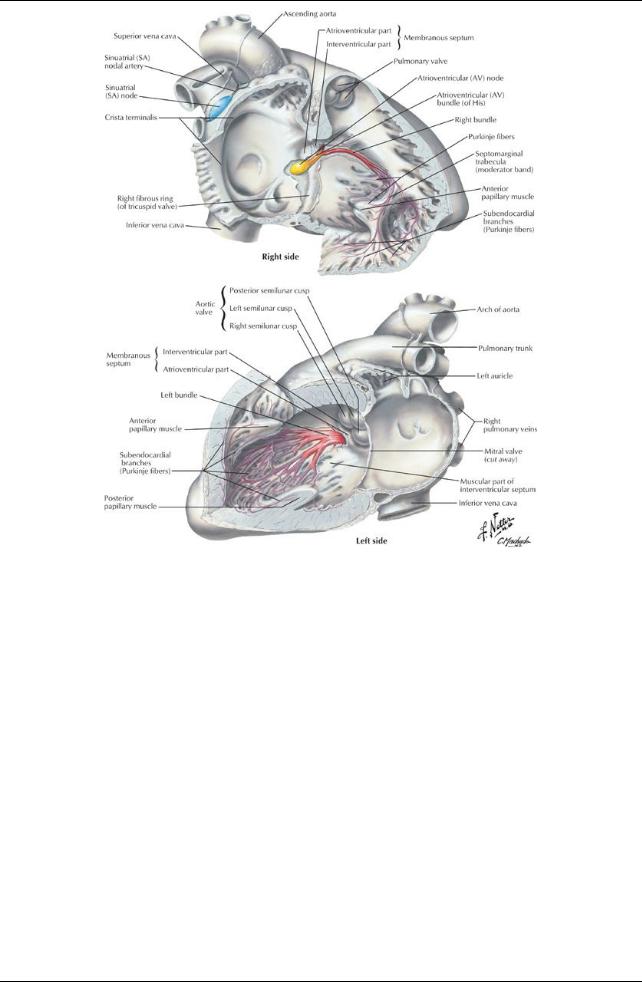
[Plate 219, Conducting System of Heart]
170 / 425
[Plate 221, Innervation of Heart: Schema]
Both divisions of the autonomic nervous system provide fibers to the cardiac plexus
The conducting system of the heart coordinates the cardiac cycle of contraction. It consists of
The sinoatrial node (SAnode), located at the superior end of the sulcus terminalis of the right atrium, near the entrance of the superior vena cava
The SAnode is the so-called pacemaker of the heart, from which impulses for contraction are initiated and spread through the musculature of both atria.
Fibers from the cardiac plexus supplythe SAnode.
Sympathetic innervation accelerates the rate and force of contraction of heart muscle.
 Parasympathetic stimulation slows down the rate and force of contraction of heart muscle. Signal from the SAnode is propagated bythe cardiac muscle to theAVnode.
Parasympathetic stimulation slows down the rate and force of contraction of heart muscle. Signal from the SAnode is propagated bythe cardiac muscle to theAVnode.
TheAVnode is located near the inferior end of the interatrial septum posteriorly, near the septal cusp of the tricuspid valve.
TheAVbundle carries the signal from theAVnode through the fibrous skeleton of the heart and the membranous interventricular septum.
It divides into right and left bundles that pass on either side of the muscular interventricular septum.
The fibers of the right and left bundles (Purkinje fibers) spread into the walls and papillarymuscles of the ventricles.
Purkinje fibers from the right bundle innervate the anterior papillarymuscle of the right ventricle via the septomarginal trabecula or moderator band, to coordinate the timing of the contraction of the papillarymuscles.
Heart Sounds
Clinicians need to listen to valve sounds.
Blood carries sound in the direction of its flow, so valve sounds are best heard (auscultated) directlysuperficial to their location or at the end of a line of blood flow through the valve.
171 / 425