


21 Lungs
STUDYAIMS
At the end of your study, you should be able to:
Understand the relationship of the pleural cavities to the mediastinum
Identifythe pleurae and the parts of the parietal pleura
Understand the anatomyof the lungs
Know the segments of the lungs
Understand vasculature and innervation of the lungs and the pleurae
150 / 425
GUIDES
Thorax: Lungs
[Plate 192, Lungs in Situ: Anterior View]
Thoracic Cavity, Pleurae and Pleural Cavity
Thoracic cavityhas
two lateral pleural cavities, containing the lungs and pleurae
 a central compartment, the mediastinum, containing all the other thoracic structures Each lung is surrounded by, and covered with, a continuous membrane, which is defined as
a central compartment, the mediastinum, containing all the other thoracic structures Each lung is surrounded by, and covered with, a continuous membrane, which is defined as
the visceral pleura, which covers the lungs and cannot be dissected from the lung
the parietal pleura, which lines the pleural cavities
The visceral and parietal pleura are continuous at the hilum of the lung where structures enter and leave the lung (bronchus, pulmonary vessels, bronchial vessels, lymphatics)
The parietal pleura has four named parts:
Costal pleura lining the internal surface of the thoracic wall
Mediastinal pleura covering the sides of the mediastinum
Diaphragmatic pleura covering the superior surface of the dome of each hemidiaphragm
 Cervical pleura-a dome of pleura extending superiorlyinto the superior thoracic aperture Visceral pleura does not have anygeneral sensoryinnervation and is insensitive to pain
Cervical pleura-a dome of pleura extending superiorlyinto the superior thoracic aperture Visceral pleura does not have anygeneral sensoryinnervation and is insensitive to pain
The parietal pleura is verysensitive to pain because of its sensorysupplybybranches of the intercostal and phrenic nerves The pleural cavityis the potential space between the parietal and visceral pleura.
The pleural cavitycontains a thin layer of serous pleural fluid, which lubricates and allows the pleurae to move smoothlyover each other during respiration.
Surface tension keeps the lung surface in contact with the thoracic wall. The lung expands and fills with air when the thoracic cavityexpands.
Lines of pleural reflection
page 105 page 106
151 / 425
Lines of pleural reflection are lines along which the parietal pleura changes directions from one wall to another.
The sternal line of pleural reflection is the sharp line along which the costal pleura becomes the mediastinal pleura
The costal line of pleural reflection is the sharp line along which the costal pleura becomes the diaphragmatic pleura
 The vertebral line of pleural reflection is a smooth reflection of the costal pleura onto the vertebrae posteriorly. The lines of pleural reflection on the left side can be remembered as 4-6-8-10-12.
The vertebral line of pleural reflection is a smooth reflection of the costal pleura onto the vertebrae posteriorly. The lines of pleural reflection on the left side can be remembered as 4-6-8-10-12.
The line of pleural reflection on the left descends in the midline of the sternum to the 4th costal cartilage, where it deviates to the left margin of the sternum at the 6th costal cartilage to accommodate the pericardium and the heart (cardiac notch).
This line then deviates to cross the 8th rib at the midclavicular line.
It crosses the 10th rib at the midaxillaryline
It then crosses the 12th rib at approximatelythe neck.
On the right side, the line of pleural reflection descends at the midline of the sternum to the xiphoid process, and then deviates 8-10-12. The lungs do not fullyoccupythe pleural cavities during expiration
There are peripheral areas where the diaphragmatic and costal pleura come in contact and these are called the costodiaphragmatic recesses.
There are areas posterior to the sternum where the costal and mediastinal pleura come in contact with each other, and these are called costomediastinal recesses.
The costomediastinal recess is larger on the left, because of the cardiac notch.
During expiration, the lower limit of the lungs is two costal spaces above the line of pleural reflection:
6-8-10: the sixth rib at the midclavicular line, the 8th rib at the midaxillaryline, and the 10th rib at the neck. Thus the costodiaphragmatic recess is approximatelytwo costal spaces deep.
Lungs
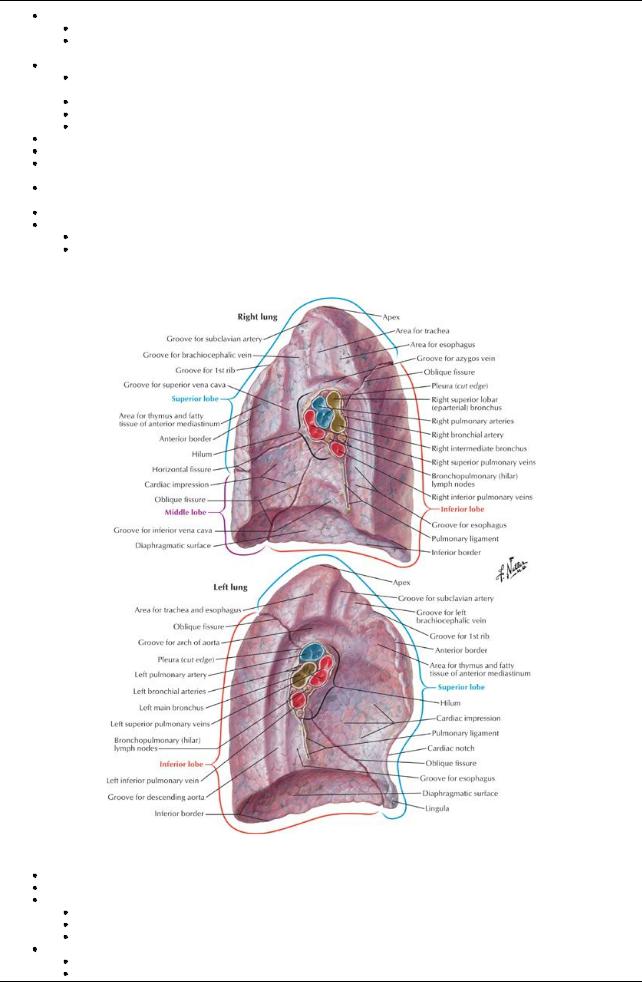
[Plate 193, Lungs: Medial Views]
Organs of respiration
Light, soft and elastic
The right lung is larger than the left and has three lobes:
Superior or upper
Middle
Inferior or lower
The left lung has two lobes
Superior or upper
Inferior or lower
152 / 425
Fissures divide the lungs into lobes
Each lung has an oblique fissure, separating the upper lobe from the lower lobe on the left and the upper and middle lobes from the lower lobe on the right
The right lung has a horizontal fissure, separating the middle lobe from the upper lobe on the right
The oblique fissure runs from the 2nd thoracic vertebra posteriorlyto the 6th costal cartilage anteriorly, or along the medial border of the scapula when the arm is raised above the head.
The horizontal fissure runs from the oblique fissure at the midaxillaryline along the 4th rib to its costal cartilage anteriorly.
The anterior margin of the left lung has an indentation-the cardiac notch, which often creates a thin process in the upper lobe called the lingula.
Each lung has three surfaces:
Costal
Mediastinal
Diaphragmatic
Each lung is connected to the mediastinum bythe root of the lung. Lung root contains:
Main stem or lobar bronchi
Pulmonaryvessels and bronchi.
Bronchial vessels, lymphatics, and autonomic nerves.
The lung root is surrounded bya pleural sleeve, from which extends the pulmonaryligament inferiorly. The pulmonaryligament
page 106 page 107
Bronchopulmonary segments
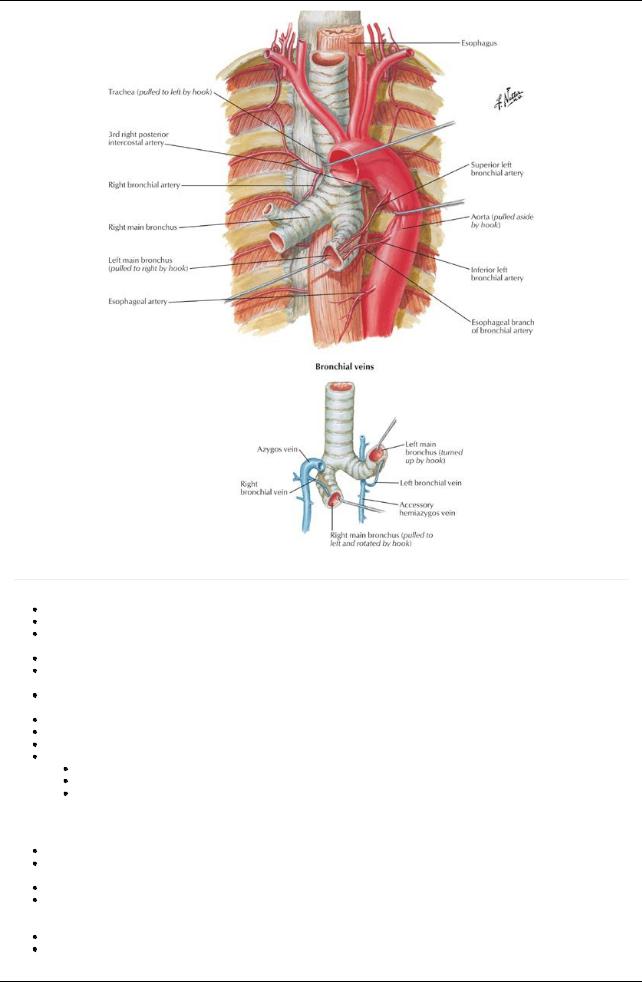
The trachea bifurcates into two main stem bronchi, right and left, at the level of the T4/5 intervertebral disc (also the sternal angle of Louis). The carina is the keel-like ridge between the two openings of the main stem bronchi.
The right main stem bronchus divides into upper and lower lobar bronchi before reaching the substance of the right lung. The main bronchi branch to form the bronchial tree.
There are three lobar bronchi on the right: upper, middle, and lower There are two lobar bronchi on the left: upper and lower
Each lobar bronchus branches into segmental bronchi that supplya bronchopulmonarysegment. Abronchopulmonarysegment
Is a pyramidallyshaped section of the lung with its base covered byvisceral pleura
Is separated from adjacent segments byconnective tissue septa
Is names for the segmental bronchus that supplies it
Has its own bronchus and segmental branch of the pulmonaryartery
Each bronchopulmonarysegment can be surgicallyresected, independent of adjacent segments The right lung has 10 bronchopulmonarysegments
Upper lobe:Apical
Anterior
Posterior
Middle lobe: Medial
Lateral
Lower lobe: Superior
Anterior basal
Posterior basal
Medial basal
Lateral basal
The left lobe has 8 to 10 bronchopulmonarysegments
Upper lobe:Apical (maybe combined with posterior to form apicoposterior)
Posterior
Anterior
Superior lingular
Inferior lingular
Lower lobe: Superior
Anterior basal (maybe combined with medial to form anteromedial basal)
Medial basal
Lateral basal
Posterior basal
The right main stem bronchus is wider and shorter than the left one and descends in a more vertical plane, so aspirated foreign objects are more likelyto lodge in it or one of its branches
Because the posterior segmental bronchus of the right lower lobe runs directlyposterior, foreign objects that are inhaled when the person is lying down, such as food, mayend up in this segmental bronchus.
Vasculature of the lungs
153 / 425
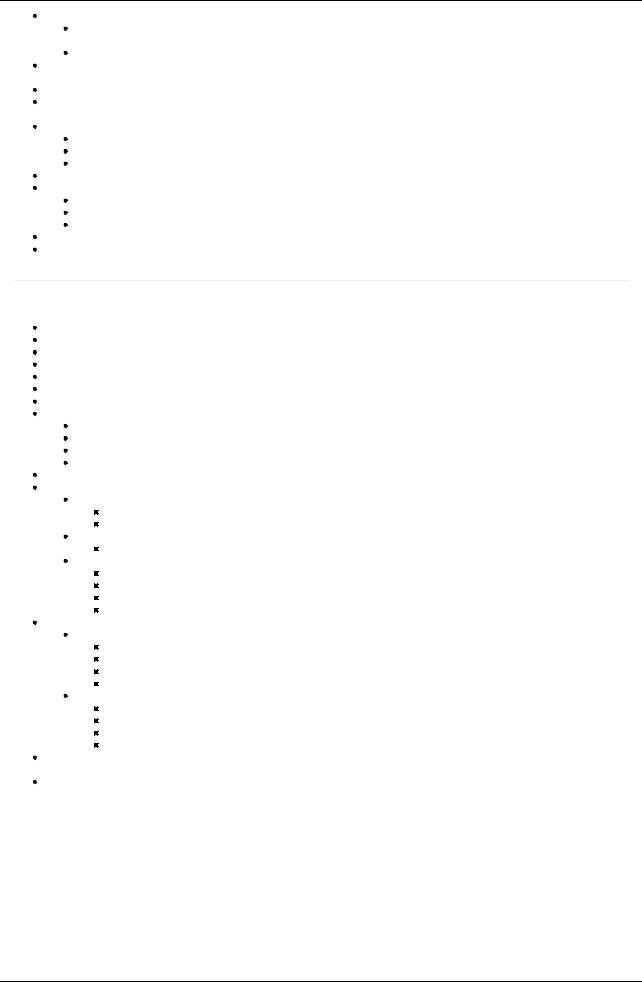
[Plate 200, Great Vessels of Superior Mediastinum]
154 / 425
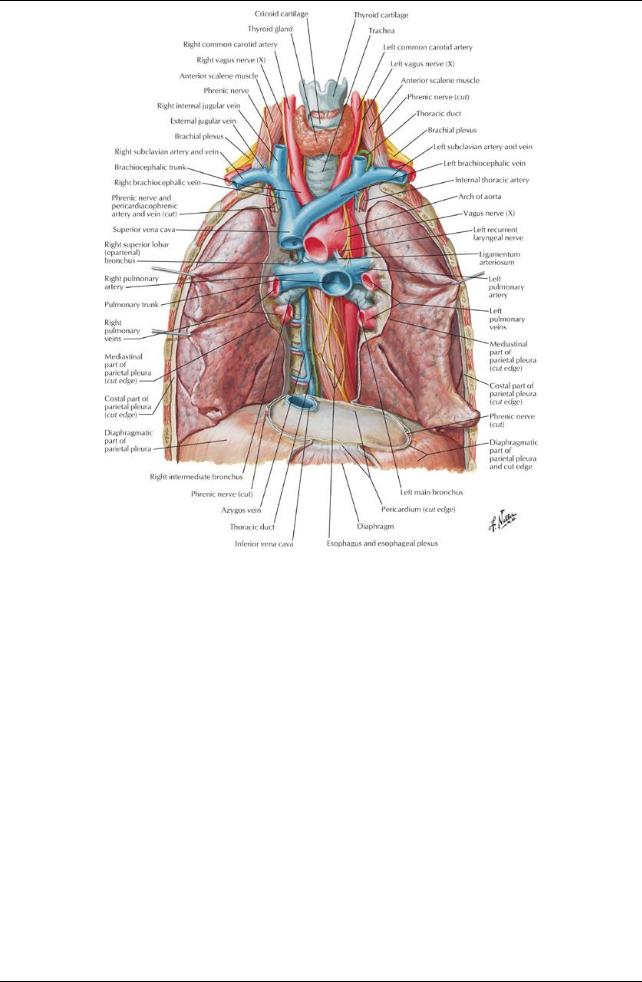
[Plate 201, Bronchial Arteries and Veins]
page 107 page 108
Each lung is supplied bya pulmonaryartery, which carries unoxygenated blood from the pulmonarytrunk from the right ventricle of the heart. Each pulmonaryarterygives rise to lobar and segmental arteries.
Intrasegmental veins drain to intersegmental veins in the pulmonarysepta, which run a separate course from the pulmonaryand segmental arteries and which drain to two pulmonaryveins for each lung.
Pulmonaryveins carryoxygenated blood to the left atrium of the heart.
Bronchial arteries from the thoracic aorta carryoxygenated blood to the tissue of the lungs, traveling along the posterior surface of the bronchi.
The left bronchial arteries come from the thoracic aorta; the single right bronchial arterymayalso arise from the superior posterior intercostal or a left superior bronchial artery.
The bronchial arteries anastomose with branches of the pulmonaryarteries.
Pulmonaryveins drain the blood to the lungs supplied bythe bronchial veins and emptyinto the azygos and accessoryhemiazygos veins. The lungs have a rich, freelyconnecting network of lymphatic vessels.
Lymph from the lungs drains to
Pulmonarylymph nodes (along the lobar bronchi)
Bronchopulmonarylymph nodes (along the main stem bronchi)
Superior and inferior tracheobronchial lymph nodes (superior and inferior to the bifurcation of the trachea)
Innervation of the lungs
Innervation is via the pulmonaryplexuses located anterior and posterior to the lung roots.
The plexuses contain postganglionic sympathetic fibers from the sympathetic trunks that innervate the smooth muscle of the bronchial tree, pulmonaryvessels, and glands of the bronchial tree.
Sympathetic fibers are bronchodilators, vasoconstrictors, and inhibit glandular secretion.
The plexuses contain preganglionic parasympathetic fibers from the vagus nerve (CN X), small parasympathetic ganglia, and postganglionic parasympathetic nerves that innervate the smooth muscle of the bronchial tree, pulmonaryvessels, and glands of the bronchial tree.
Parasympathetic fibers are bronchoconstrictors, vasodilators, and secretomotor to the glands.
Visceral afferent fibers carryinformation involved in cough reflexes, stretch reception, blood pressure, chemoreception, and nociception
155 / 425
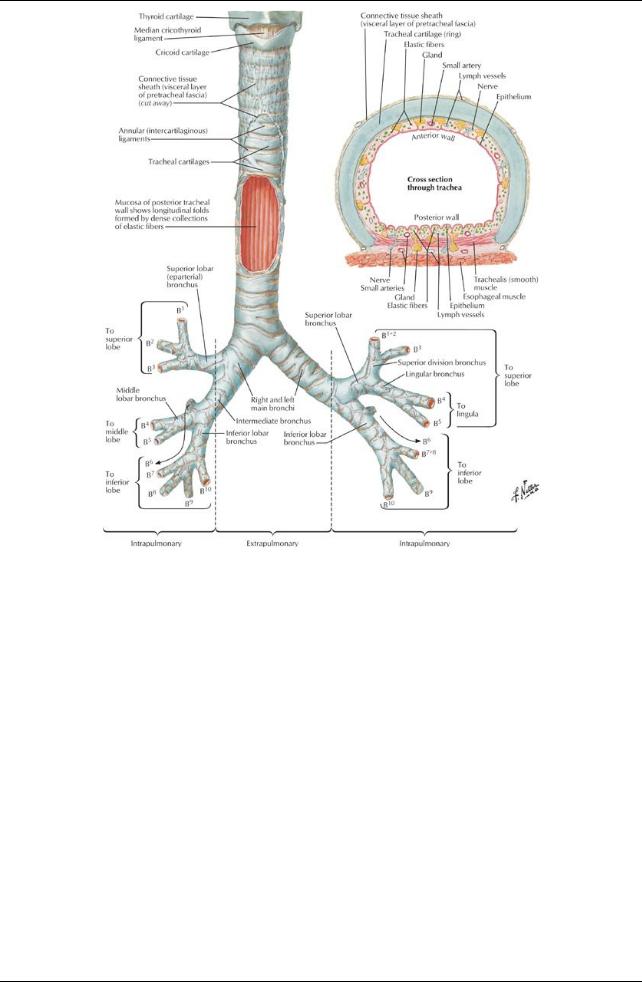
[Plate 196, Trachea and Major Bronchi]
156 / 425