

- •Preface to the 3rd edition
- •General Pharmacology
- •Systems Pharmacology
- •Therapy of Selected Diseases
- •Subject Index
- •Abbreviations
- •General Pharmacology
- •History of Pharmacology
- •Drug and Active Principle
- •The Aims of Isolating Active Principles
- •European Plants as Sources of Effective Medicines
- •Drug Development
- •Congeneric Drugs and Name Diversity
- •Oral Dosage Forms
- •Drug Administration by Inhalation
- •Dermatological Agents
- •From Application to Distribution in the Body
- •Potential Targets of Drug Action
- •External Barriers of the Body
- •Blood–Tissue Barriers
- •Membrane Permeation
- •Binding to Plasma Proteins
- •The Liver as an Excretory Organ
- •Biotransformation of Drugs
- •Drug Metabolism by Cytochrome P450
- •The Kidney as an Excretory Organ
- •Presystemic Elimination
- •Drug Concentration in the Body as a Function of Time—First Order (Exponential) Rate Processes
- •Time Course of Drug Concentration in Plasma
- •Time Course of Drug Plasma Levels during Repeated Dosing (A)
- •Time Course of Drug Plasma Levels during Irregular Intake (B)
- •Accumulation: Dose, Dose Interval, and Plasma Level Fluctuation (A)
- •Dose–Response Relationship
- •Concentration–Effect Curves (B)
- •Concentration–Binding Curves
- •Types of Binding Forces
- •Agonists—Antagonists
- •Other Forms of Antagonism
- •Enantioselectivity of Drug Action
- •Receptor Types
- •Undesirable Drug Effects, Side Effects
- •Drug Allergy
- •Cutaneous Reactions
- •Drug Toxicity in Pregnancy and Lactation
- •Pharmacogenetics
- •Placebo (A)
- •Systems Pharmacology
- •Sympathetic Nervous System
- •Structure of the Sympathetic Nervous System
- •Adrenergic Synapse
- •Adrenoceptor Subtypes and Catecholamine Actions
- •Smooth Muscle Effects
- •Cardiostimulation
- •Metabolic Effects
- •Structure–Activity Relationships of Sympathomimetics
- •Indirect Sympathomimetics
- •Types of
- •Antiadrenergics
- •Parasympathetic Nervous System
- •Cholinergic Synapse
- •Parasympathomimetics
- •Parasympatholytics
- •Actions of Nicotine
- •Localization of Nicotinic ACh Receptors
- •Effects of Nicotine on Body Function
- •Aids for Smoking Cessation
- •Consequences of Tobacco Smoking
- •Dopamine
- •Histamine Effects and Their Pharmacological Properties
- •Serotonin
- •Vasodilators—Overview
- •Organic Nitrates
- •Calcium Antagonists
- •ACE Inhibitors
- •Drugs Used to Influence Smooth Muscle Organs
- •Cardiac Drugs
- •Cardiac Glycosides
- •Antiarrhythmic Drugs
- •Iron Compounds
- •Prophylaxis and Therapy of Thromboses
- •Possibilities for Interference (B)
- •Heparin (A)
- •Hirudin and Derivatives (B)
- •Fibrinolytics
- •Intra-arterial Thrombus Formation (A)
- •Formation, Activation, and Aggregation of Platelets (B)
- •Inhibitors of Platelet Aggregation (A)
- •Presystemic Effect of ASA
- •Plasma Volume Expanders
- •Lipid-lowering Agents
- •Diuretics—An Overview
- •NaCl Reabsorption in the Kidney (A)
- •Aquaporins (AQP)
- •Osmotic Diuretics (B)
- •Diuretics of the Sulfonamide Type
- •Potassium-sparing Diuretics (A)
- •Vasopressin and Derivatives (B)
- •Drugs for Gastric and Duodenal Ulcers
- •Laxatives
- •Antidiarrheal Agents
- •Drugs Affecting Motor Function
- •Muscle Relaxants
- •Nondepolarizing Muscle Relaxants
- •Depolarizing Muscle Relaxants
- •Antiparkinsonian Drugs
- •Antiepileptics
- •Pain Mechanisms and Pathways
- •Eicosanoids
- •Antipyretic Analgesics
- •Nonsteroidal Anti-inflammatory Drugs (NSAIDs)
- •Cyclooxygenase (COX) Inhibitors
- •Local Anesthetics
- •Opioid Analgesics—Morphine Type
- •General Anesthesia and General Anesthetic Drugs
- •Inhalational Anesthetics
- •Injectable Anesthetics
- •Sedatives, Hypnotics
- •Benzodiazepines
- •Pharmacokinetics of Benzodiazepines
- •Therapy of Depressive Illness
- •Mania
- •Therapy of Schizophrenia
- •Psychotomimetics (Psychedelics, Hallucinogens)
- •Hypothalamic and Hypophyseal Hormones
- •Thyroid Hormone Therapy
- •Glucocorticoid Therapy
- •Follicular Growth and Ovulation, Estrogen and Progestin Production
- •Oral Contraceptives
- •Antiestrogen and Antiprogestin Active Principles
- •Aromatase Inhibitors
- •Insulin Formulations
- •Treatment of Insulin-dependent Diabetes Mellitus
- •Treatment of Maturity-Onset (Type II) Diabetes Mellitus
- •Oral Antidiabetics
- •Drugs for Maintaining Calcium Homeostasis
- •Drugs for Treating Bacterial Infections
- •Inhibitors of Cell Wall Synthesis
- •Inhibitors of Tetrahydrofolate Synthesis
- •Inhibitors of DNA Function
- •Inhibitors of Protein Synthesis
- •Drugs for Treating Mycobacterial Infections
- •Drugs Used in the Treatment of Fungal Infections
- •Chemotherapy of Viral Infections
- •Drugs for the Treatment of AIDS
- •Drugs for Treating Endoparasitic and Ectoparasitic Infestations
- •Antimalarials
- •Other Tropical Diseases
- •Chemotherapy of Malignant Tumors
- •Targeting of Antineoplastic Drug Action (A)
- •Mechanisms of Resistance to Cytostatics (B)
- •Inhibition of Immune Responses
- •Antidotes and Treatment of Poisonings
- •Therapy of Selected Diseases
- •Hypertension
- •Angina Pectoris
- •Antianginal Drugs
- •Acute Coronary Syndrome— Myocardial Infarction
- •Congestive Heart Failure
- •Hypotension
- •Gout
- •Obesity—Sequelae and Therapeutic Approaches
- •Osteoporosis
- •Rheumatoid Arthritis
- •Migraine
- •Common Cold
- •Bronchial Asthma
- •Emesis
- •Alcohol Abuse
- •Local Treatment of Glaucoma
- •Further Reading
- •Further Reading
- •Picture Credits
- •Drug Indexes

262 Hormones
Treatment of Maturity-Onset (Type II) Diabetes Mellitus
In overweight adults, a diabetic metabolic condition may develop (type II or non-insu- lin-dependent diabetes) when there is a relative insulin deficiency—enhanced demand cannot be met by a diminishing insulin secretion.
The cause of increased insulin requirement is an insulin resistance of target organs. The decrease in the effectiveness of insulin is due to a reduction in the density of insulin receptors in target tissues and a decreased ef ciencyof signal transduction of insulin-receptor complexes. Conceivably, obesity with increased storage of triglycerides causes a decrease in insulin sensitivity of target organs. The loss insensitivitycanbe compensated by enhancing insulin concentration. In panel (A), this situation is represented schematically by the decreased receptor density. In the obese patient, the maximum binding possible (plateau of curve) is displaced downward, indicative of the reduction in receptor numbers. At low insulin concentrations, correspondingly less binding of insulin occurs, compared with the control condition (normal weight). For a given metabolic effect (say, utilization of carbohydrates contained in a piece of cake), a certain number of receptors must be occupied. As shown by the binding curves (dashed lines), this can still be achieved with areduced receptor number; although onlyat a higher concentration of insulin.
Development of adult diabetes (B). A subject with normal body weight (left) ingests a specified amount of carbohydrate; to maintain blood glucose concentration within the physiological range, the necessary amount of insulin is released into the blood. Compared with a normal subject, the overweight patient with insulin resistance requires a continually elevated output of insulin (orange curves) to avoid an excessive rise of blood glucose levels (green curves) during an
equivalent carbohydrate load. When the insulin secretory capacity of the pancreas decreases, this is first noted as arise in blood glucose during glucose loading (latent diabetes mellitus). As insulin secretory capacity declines further, not even the fasting blood level can be maintained (manifest, overt diabetes).
Treatment. Caloric restriction to restore body weight to normal is associated with an increase in insulin responsiveness, even before a normal weight is reached. Moreover, physical activity is important because it enhances peripheral utilization of glucose. When changes in lifestyle are insuf cient in correcting the diabetic condition, therapy with oral antidiabetics is indicated (p.264).
Therapy of first choice is weight reduction, not administration of drugs!
A metabolic syndrome is said to be present when at least three of the following five riskfactors can be identified in apatient:
1.Elevated blood glucose levels
2.Elevated blood lipid levels
3.Obesity
4.Lowered HDL levels
5.Hypertension
Overweight and resistance to insulin appear to play pivotal roles in the pathophysiological process. The resulting hyperinsulinemia inducesarise in systemic arterial blood pressure and probably also a hyperglyceridemia associated with an unfavorable LDL/HDL quotient. This combination of risk factors lowers life expectancy and calls for therapeutic intervention. The metabolic syndrome has a high prevalence; in industrialized countries, up to 20% of adults are believed to suffer from it.
Luellmann, Color Atlas of Pharmacology © 2005 Thieme
All rights reserved. Usage subject to terms and conditions of license.

Treatment of Maturity-Onset Diabetes Mellitus |
263 |
A. Insulin concentration and binding in normal and overweight subjects |
|
|
Insulin binding |
|
Normal receptor number |
Insulin receptor |
Normal |
binding |
diet |
needed |
|
for euglycemia |
|
|
Decreased |
|
receptor |
|
number |
|
Obesity |
|
Insulin concentration |
B. Development of maturity-onset diabetes |
|
|
|
|
Oral |
|
|
anti- |
|
|
diabetic |
Insulin release |
|
|
Time |
|
|
Glucose in blood |
|
|
|
|
Diagnosis: |
|
latent |
overt |
Weight reduction |
Diabetes mellitus |
|
|
|
|
Therapy of 1st choice |
|
Therapy of 2nd choice |
Luellmann, Color Atlas of Pharmacology © 2005 Thieme
All rights reserved. Usage subject to terms and conditions of license.

264 Hormones
Oral Antidiabetics
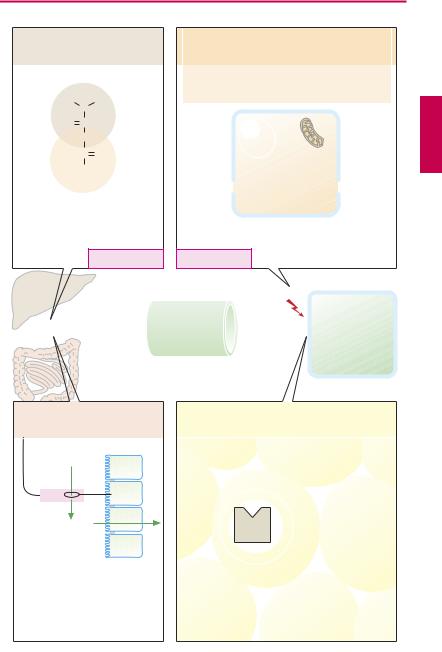
In principle, the blood concentration of glucose represents a balance between influx into the bloodstream (chiefly from liver and intestines) and egress from blood into consuming tissues and organs. In (A), drugs available for lowering an elevated level of glucose are grouped schematically in relation to these two processes.
Metformin is a biguanide derivative that can normalize an elevated blood glucose level, provided that insulin is present. The mechanism underlying this effect is not completely understood. Decreased glucose release from the liver appears to play an essential part. Metformin does not increase release of insulin and therefore does not promote hyperinsulinemia. The risk of hypoglycemia is relatively less common. Triglyceride concentrations can decrease. Metformin has proved itself as a monotherapeutic in obese type II diabetics. It can be combined with other oral antidiabetics as well as insulin. Frequent adverse effects include anorexia, nausea, and diarrhea. Overproduction of lactic acid (lactate acidosis) is a rare, potentially fatal reaction. It is contraindicated in renal insuf ciency and therefore should be avoided in elderly patients.
Oral antidiabetics of the sulfonylurea type increase the release of insulin from pancreatic B-cells. They inhibit ATP-gated K+ channels and thereby cause depolarization of the B-cell membrane. Normally, these channels are closed when intracellular levels of glucose, and hence of ATP, increase. This drug class includes tolbutamide (500– 2000 mg/day) and glyburide (glibenclamide) (1.75–10.5 mg/day). In some patients, it is not possible to stimulate insulin secretion from the outset; in others, therapy fails later. Matching of dosage of the oral antidiabetic and caloric intake is necessary. Hypoglycemia is the most important unwanted effect. Enhancement of the hypoglycemic effect can result from drug interactions: displacement of antidiabetic drug from plasma
protein binding sites, for example, by sulfonamides or acetylsalicylic acid.
Repaglinide possesses the same mechanism of action as the sulfonylureas but differs in chemical structure. After oral administration, the effect develops rapidly and fades away quickly. Therefore, repaglinide can be taken immediately before a meal.
“Glitazone” is an appellation referring to thiazolidinedione derivatives such as rosiglitazone and pioglitazone. These substances augment the insulin sensitivity of target tissues. They are agonists at the peroxisome proliferator-activated receptor of the γ subtype (PPARγ), a transcription-regulating receptor. As a result, they (a) promote the maturation of preadipocytes into adipocytes,
(b) increase insulin sensitivity, and (c) enhance cellular glucose uptake. Besides fat tissue, skeletal muscle is also affected.
Rosiglitazone and pioglitazone are approved only for combination therapy when adequate glycemic control cannot be achieved with either metformin or a sulfonylurea alone. A combination with insulin is contraindicated. Adverse effects include weight gain and fluid retention (thus contraindication for any stage of congestive heart failure). Hepatic function requires close monitoring (withdrawal of troglitazone because of fatal liver failure).
Acarbose is an inhibitor of α-glucosidase (localized in the brush border of intestinal epithelium), which liberates glucose from disaccharides. It retards breakdown of carbohydrates, and hence absorption of glucose. Owing to increased fermentation of carbohydrates by gut bacteria, flatulence and diarrhea may develop. Miglitol has a similar effect but is absorbed from the intestine.
Luellmann, Color Atlas of Pharmacology © 2005 Thieme
All rights reserved. Usage subject to terms and conditions of license.
|
|
|
|
|
|
Oral Antidiabetics |
|
|
265 |
|||
A. Oral antidiabetics |
|
|
|
|
|
|
|
|
|
|
||
Metformin, a biguanide derivative |
|
Glibenclamide, a sulfonylurea derivative |
Cl |
|||||||||
|
|
|
|
|
|
|
|
|
|
O |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NH |
SO2 |
|
CH2 |
CH2 |
NH |
C |
|
|
|
|
|
O |
C |
|
|
|
|
H3C |
O |
|
|
|
|
|
|
NH |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
H3C |
N |
CH3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HN |
C |
|
B-cells |
|
|
|
|
|
Glucose |
|
||
|
of pancreas |
|
|
|
|
|
|
|
||||
|
NH |
|
|
|
|
|
ATP-gated |
|
||||
|
|
|
|
|
|
|
|
|
|
|||
|
C |
NH |
|
|
|
|
|
|
|
K+-channel |
||
|
|
|
|
|
|
ATP |
|
|
|
|
||
|
NH2 |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
K+ |
|
|
Blockade |
|
|
K+ |
|
|
Inhibition of |
|
|
|
|
|
|
|
|
|
|
|
|
hepatic glucose release |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
Membrane |
|
||
|
|
|
|
|
|
|
|
|
potential depolarized |
|||
|
|
Lactic acidosis |
Hypoglycemia |
Insulin secretion |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
||||
Liver |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Insulin |
|
|
|
|
|
|
|
|
Glucose |
|
|
|
|
|
|
|
|
|
|
|
Influx |
concentration |
|
Egress |
|
|
|
|
|
||
|
|
|
in blood |
|
|
|
|
|
|
|
|
|
Intestines |
|
|
|
|
|
|
|
|
|
|
|
|
Acarbose, a “false” |
|
Rosiglitazone, a thiazolidinedione derivative |
|
|||||||||
tetrasaccharide |
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
N |
|
|
|
|
|
|
O |
|
|
|
|
|
|
|
|
|
|
|
S |
|
|
|
|
|
|
N |
CH2 |
CH2 |
O |
|
C 2 |
|
|
|
Disaccharide |
|
|
|
|
NH |
|
||||||
|
|
H3C |
|
|
|
|
H |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
O |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
α -Glucosidase |
|
|
|
|
|
Pre-adipocytes |
|
|||
|
|
|
|
|
|
|
|
Adipocytes |
|
|||
Glucose |
|
|
|
|
PPARγ |
|
Insulin sensitivity |
|
||||
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
DNA |
|
Glucose uptake |
|
|||
|
|
|
|
|
|
|
|
|
||||
retards enteral |
|
|
|
|
|
|
|
|
|
|
||
absorption of glucose |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
Fatty tissue |
|
|
|
|
|
|
|
|
|
|
|
|
Weight gain |
|
Contraindication in congestive |
||||||
|
Intestinal complaints |
|
|
|
|
heart failure, NYHA 1–4 |
|
|||||
Luellmann, Color Atlas of Pharmacology © 2005 Thieme
All rights reserved. Usage subject to terms and conditions of license.