

- •Preface to the 3rd edition
- •General Pharmacology
- •Systems Pharmacology
- •Therapy of Selected Diseases
- •Subject Index
- •Abbreviations
- •General Pharmacology
- •History of Pharmacology
- •Drug and Active Principle
- •The Aims of Isolating Active Principles
- •European Plants as Sources of Effective Medicines
- •Drug Development
- •Congeneric Drugs and Name Diversity
- •Oral Dosage Forms
- •Drug Administration by Inhalation
- •Dermatological Agents
- •From Application to Distribution in the Body
- •Potential Targets of Drug Action
- •External Barriers of the Body
- •Blood–Tissue Barriers
- •Membrane Permeation
- •Binding to Plasma Proteins
- •The Liver as an Excretory Organ
- •Biotransformation of Drugs
- •Drug Metabolism by Cytochrome P450
- •The Kidney as an Excretory Organ
- •Presystemic Elimination
- •Drug Concentration in the Body as a Function of Time—First Order (Exponential) Rate Processes
- •Time Course of Drug Concentration in Plasma
- •Time Course of Drug Plasma Levels during Repeated Dosing (A)
- •Time Course of Drug Plasma Levels during Irregular Intake (B)
- •Accumulation: Dose, Dose Interval, and Plasma Level Fluctuation (A)
- •Dose–Response Relationship
- •Concentration–Effect Curves (B)
- •Concentration–Binding Curves
- •Types of Binding Forces
- •Agonists—Antagonists
- •Other Forms of Antagonism
- •Enantioselectivity of Drug Action
- •Receptor Types
- •Undesirable Drug Effects, Side Effects
- •Drug Allergy
- •Cutaneous Reactions
- •Drug Toxicity in Pregnancy and Lactation
- •Pharmacogenetics
- •Placebo (A)
- •Systems Pharmacology
- •Sympathetic Nervous System
- •Structure of the Sympathetic Nervous System
- •Adrenergic Synapse
- •Adrenoceptor Subtypes and Catecholamine Actions
- •Smooth Muscle Effects
- •Cardiostimulation
- •Metabolic Effects
- •Structure–Activity Relationships of Sympathomimetics
- •Indirect Sympathomimetics
- •Types of
- •Antiadrenergics
- •Parasympathetic Nervous System
- •Cholinergic Synapse
- •Parasympathomimetics
- •Parasympatholytics
- •Actions of Nicotine
- •Localization of Nicotinic ACh Receptors
- •Effects of Nicotine on Body Function
- •Aids for Smoking Cessation
- •Consequences of Tobacco Smoking
- •Dopamine
- •Histamine Effects and Their Pharmacological Properties
- •Serotonin
- •Vasodilators—Overview
- •Organic Nitrates
- •Calcium Antagonists
- •ACE Inhibitors
- •Drugs Used to Influence Smooth Muscle Organs
- •Cardiac Drugs
- •Cardiac Glycosides
- •Antiarrhythmic Drugs
- •Iron Compounds
- •Prophylaxis and Therapy of Thromboses
- •Possibilities for Interference (B)
- •Heparin (A)
- •Hirudin and Derivatives (B)
- •Fibrinolytics
- •Intra-arterial Thrombus Formation (A)
- •Formation, Activation, and Aggregation of Platelets (B)
- •Inhibitors of Platelet Aggregation (A)
- •Presystemic Effect of ASA
- •Plasma Volume Expanders
- •Lipid-lowering Agents
- •Diuretics—An Overview
- •NaCl Reabsorption in the Kidney (A)
- •Aquaporins (AQP)
- •Osmotic Diuretics (B)
- •Diuretics of the Sulfonamide Type
- •Potassium-sparing Diuretics (A)
- •Vasopressin and Derivatives (B)
- •Drugs for Gastric and Duodenal Ulcers
- •Laxatives
- •Antidiarrheal Agents
- •Drugs Affecting Motor Function
- •Muscle Relaxants
- •Nondepolarizing Muscle Relaxants
- •Depolarizing Muscle Relaxants
- •Antiparkinsonian Drugs
- •Antiepileptics
- •Pain Mechanisms and Pathways
- •Eicosanoids
- •Antipyretic Analgesics
- •Nonsteroidal Anti-inflammatory Drugs (NSAIDs)
- •Cyclooxygenase (COX) Inhibitors
- •Local Anesthetics
- •Opioid Analgesics—Morphine Type
- •General Anesthesia and General Anesthetic Drugs
- •Inhalational Anesthetics
- •Injectable Anesthetics
- •Sedatives, Hypnotics
- •Benzodiazepines
- •Pharmacokinetics of Benzodiazepines
- •Therapy of Depressive Illness
- •Mania
- •Therapy of Schizophrenia
- •Psychotomimetics (Psychedelics, Hallucinogens)
- •Hypothalamic and Hypophyseal Hormones
- •Thyroid Hormone Therapy
- •Glucocorticoid Therapy
- •Follicular Growth and Ovulation, Estrogen and Progestin Production
- •Oral Contraceptives
- •Antiestrogen and Antiprogestin Active Principles
- •Aromatase Inhibitors
- •Insulin Formulations
- •Treatment of Insulin-dependent Diabetes Mellitus
- •Treatment of Maturity-Onset (Type II) Diabetes Mellitus
- •Oral Antidiabetics
- •Drugs for Maintaining Calcium Homeostasis
- •Drugs for Treating Bacterial Infections
- •Inhibitors of Cell Wall Synthesis
- •Inhibitors of Tetrahydrofolate Synthesis
- •Inhibitors of DNA Function
- •Inhibitors of Protein Synthesis
- •Drugs for Treating Mycobacterial Infections
- •Drugs Used in the Treatment of Fungal Infections
- •Chemotherapy of Viral Infections
- •Drugs for the Treatment of AIDS
- •Drugs for Treating Endoparasitic and Ectoparasitic Infestations
- •Antimalarials
- •Other Tropical Diseases
- •Chemotherapy of Malignant Tumors
- •Targeting of Antineoplastic Drug Action (A)
- •Mechanisms of Resistance to Cytostatics (B)
- •Inhibition of Immune Responses
- •Antidotes and Treatment of Poisonings
- •Therapy of Selected Diseases
- •Hypertension
- •Angina Pectoris
- •Antianginal Drugs
- •Acute Coronary Syndrome— Myocardial Infarction
- •Congestive Heart Failure
- •Hypotension
- •Gout
- •Obesity—Sequelae and Therapeutic Approaches
- •Osteoporosis
- •Rheumatoid Arthritis
- •Migraine
- •Common Cold
- •Bronchial Asthma
- •Emesis
- •Alcohol Abuse
- •Local Treatment of Glaucoma
- •Further Reading
- •Further Reading
- •Picture Credits
- •Drug Indexes
326 Therapy of Selected Diseases
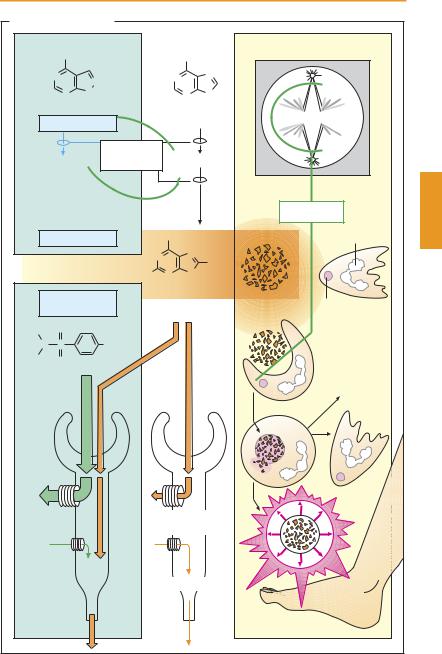
Gout
Gout is an inherited metabolic disease that results from hyperuricemia, an elevation in the blood of uric acid, the end-product of purine degradation. Uric acid is not readily water-soluble; it therefore tends to crystallize at unphysiologically elevated concentrations, predominantly in bradytrophic tissues (such as the metatarsophalangeal joint). Like other crystals, urate crystals provide a strong stimulus for neutrophilic granulocytes and macrophages. Neutrophils are attracted (1) and phagocytose (2) this indigestible material. In the process, neutrophils release (3) proinflammatory cytokines. Macrophages also phagocytose the crystals, injure themselves, and liberate lysosomal enzymes that likewise promote inflammation and attack tissues. As a result, an acute and very painful gout attack may develop (4).
The therapy of gout is twofold: (1) treatment of the acute attack; and (2) chronic lowering of hyperuricemia.
1.The acute attack demands prompt action to relieve the patient from his painful state. The classical remedy (already used by Hippocrates) is colchicine, an alkaloid from the autumn crocus (Colchicum autumnale). This substance binds with high af nity to microtubular proteins and impairstheirfunction,causinginteraliaarrest ofmitosisatmetaphase(“spindlepoison”). Its acute antigout activity is due to inhibition of neutrophil and macrophage reactions. The details of these mechanisms are notcompletelyclear; atanyrate,release of
proinflammatory cytokines is prevented. Colchicine is usually given orally (e. g., 0.5 mg hourly up to a maximum daily dose of 8 mg). Colchicine therapy is limited by injury to the gastrointestinal epithelium, which divides rapidly and therefore reacts with high sensitivity to the spindle poison. Nonsteroidal anti-inflammatory drugs, such as diclofenac and indometacin, are also effective; on occasion, glucocorticoids may be of additional help.
2.Chronic lowering of urate levels below 6 mg/l blood requires (a) an appropriate diet that avoids purine (cell nuclei)-rich foods (e. g., organ offal); and (b) urico-
statics for decreasing uric acid production.
Allopurinol, as well as its accumulating metabolite, oxypurinol (“alloxanthine”), inhibits xanthine oxidase, which catalyzes urate formation from hypoxanthine via xanthine. These precursors are readily eliminated via the urine. Allopurinol is given orally (300–800 mg/day). Apart from infrequent allergic reactions, it is well tolerated and is the drug of choice for gout prophylaxis. Gout attacks may occur at the start of therapy but they can be prevented by concurrent administration of colchicine (0.5–1.5 mg/day).
Uricosurics, such as probenecid or benzbromarone (100 mg/day), promote renal excretion of uric acid. They saturate the organic acid transport system in the proximal renal tubules, making it unavailable for urate reabsorption. When underdosed, they inhibit only the acid secretory system, which has a smaller transport capacity. Urate elimination is then inhibited and a gout attack is possible. In patients with urate stones in the urinary tract, uricosurics are contraindicated.
Uricolytics. Nonprimates are able, via the enzyme urate oxidase, to metabolize uric acid to allantoin, a product with better water solubility and faster renal elimination. Rasburicase, a recombinant urate oxidase, can be given by infusion in patients with malignant neoplasias, in whom chemotherapy is liable to generate a massive amount of uric acid.
Luellmann, Color Atlas of Pharmacology © 2005 Thieme
All rights reserved. Usage subject to terms and conditions of license.
|
|
|
|
|
|
Gout |
327 |
A. Gout and its therapy |
|
|
|
|
|||
|
OH |
|
|
|
OH |
|
|
|
N |
N |
|
N |
|
N |
|
|
|
|
|
|
|
|
|
|
N |
N |
|
|
N |
N |
|
|
|
H |
|
|
|
H |
|
|
Allopurinol |
|
Hypoxanthine |
|
|||
|
|
|
Xanthine |
|
Xanthine |
|
|
Alloxanthine |
Oxidase |
|
|
||||
|
|
|
|
|
|
Colchicine |
|
|
Uricostatic |
|
OH |
|
Nucleus |
|
|
|
|
|
|
N |
N |
O– H+ |
|
|
|
|
|
|
|
||
|
|
|
|
|
N |
|
|
|
|
|
HO |
N |
|
|
|
|
|
|
|
|
H |
|
|
|
Uricosuric |
|
Uric acid |
|
|
||
|
|
|
|
|
1 |
||
|
Probenecid |
|
|
|
Lysosome |
||
|
|
|
|
|
|||
H7 C3 |
O |
|
|
|
|
Neutrophil |
|
|
|
|
|
|
|
||
N |
S |
|
COO– H+ |
|
|
|
|
|
|
|
granulocyte |
|
|||
H7 C3 |
|
|
|
|
|
|
|
O |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
factors |
|
|
|
|
|
|
|
Chemotactic |
|
|
|
|
|
|
|
3 |
|
|
|
|
|
Anion (urate) |
|
||
|
|
|
|
reabsorption |
|
||
|
|
|
|
Anion secretion |
|
||
|
|
|
|
|
|
Gout attack |
|
Luellmann, Color Atlas of Pharmacology © 2005 Thieme
All rights reserved. Usage subject to terms and conditions of license.
328 Therapy of Selected Diseases
Obesity—Sequelae and Therapeutic Approaches
In industrialized nations, a significant portion of the population is overweight. The Body-Mass-Index (BMI) provides a reliable and simple quantitative criterion for assessing this condition; it is calculated as follows:
= body weight in kg BMI square of body height in m
Normal values range from 22 to 28. Values > 30 are indicative of an overweight condition. Obesity is always the consequence of a disturbed energy balance: caloric intake exceeds consumption. Almost unavoidably, excess body weight and obesity lead to diseases and a shortened lifespan.
The most important secondary disorders include development of type II diabetes mellitus, which alone shortens life, and hypertension, which together with disturbed lipid metabolism gives rise to atherosclerosis (angina pectoris, inadequate cerebral blood flow, etc.). Owing to the constant mechanical stress, weight-bearing joints suffer, resulting in arthrotic complaints. Finally, obesity gives rise to psychological problems that may overwhelm the coping ability of both adults and children.
The treatment of obesity—and it should be treated to safeguard normal life expec- tancy—is extraordinarily dif cult. Although the principle “eat much less, move much more” is so simple, no more than a depressingly low percentage of patients can be relieved of their condition. Not until the obese individual, after suf cient counseling, realizes that he or she needs to make a change in lifestyle and can then muster suf cient selfdiscipline to stick to the “new life,” will a return to normal body weight and protection from secondary diseases be achieved. Requisite changes include a diet low in fat with reduced caloric content (~ 1000 kcal/day), no snacks (sweets, potato chips, lemonades, beer, etc.), and plenty of physical exercise
(sports, hiking, swimming, tennis, etc. instead of the TV easy-chair). Under these conditions, body weight will drop slowly; dramatic changes of several kilograms in a few days are not to be expected. This reduction therapy must be kept up for months.
Regrettably, the pharmacologist must confess that no drugs exist that can be recommended for the purpose of weight reduction. The so-called appetite suppressants
(anorexiants) act only, if at all, for a limited period and are fraught with side effects. Most anorexiants are derivatives of methamphetamine that have been withdrawn from the market. A different mechanism of action is involved in the case of an inhibitor of pancreatic lipase, which is required in the intestines for fat absorption. This inhibitor (orlistat) diminishes fat absorption so that fats reach the lower bowel, where they can cause disturbances: flatulence, steatorrhea, and frequent need to relieve the bowels occur in about 30% of affected subjects. These symptoms correspond exactly to those seen in pancreatic hypofunction which are then usually treated with pancreatic lipase. Before an obese person submits to treatment with orlistat, he or she should voluntarily reduce the food fat content by one half to live free of such unpleasant adverse effects.
In summary, the obese individual has no choice but to normalize the energy balance under sympathetic guidance and by strength of will, and thus evade any secondary diseases.
Luellmann, Color Atlas of Pharmacology © 2005 Thieme
All rights reserved. Usage subject to terms and conditions of license.
|
|
|
|
|
|
|
|
|
|
|
|
Obesity |
329 |
A. Obesity: Sequelae and therapeutic approaches |
|
|
|
|
|
|
|||||||
|
|
|
|
|
E n e r g y b a l a n c e |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
Consumption |
|
|
|
||
Consumption BMI 25 - 27 |
Intake |
|
|
|
|
BMI >> 30 |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
Intake |
|
|
|
Therapy |
|
|
|
|
Consequences: life expectancy |
||||||
Caloric restriction |
|
|
|
Diabetes mellitus |
|
|
|
||||||
Intensive psychological counseling, |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
||||||
much exercise |
|
|
|
|
|
|
Hyperlipoproteinemia |
||||||
|
|
|
|
|
|
|
|
|
|
||||
|
Drugs |
|
|
|
|
Hypertension |
|
|
|
||||
Anorexiants |
|
|
|
|
|
|
|
Joint mechanical stress |
|||||
Methamphetamine |
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
||||
derivatives |
|
|
|
|
|
|
|
|
|
|
|
||
Sibutramine |
|
|
|
|
|
|
|
|
|
|
|
||
Lipase inhibitor orlistat |
|
|
|
Psychosocial problems |
|
||||||||
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
CF3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
H |
|
|
Cl |
|
|
|
|
|
|
|
|
CH2 |
CH |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
CH3 |
CH2 |
CH3 |
|
|
|
|
|
|
|
|
|
|
H |
Fenfluramine |
|
|
|
|
|
|
CH3 |
|
|
|
|
|
(discontinued) |
|
C |
|
CH |
|
|
||||
|
|
|
|
|
|
|
|
|
N |
|
|||
CH2 |
CH |
N |
|
|
|
|
H2C |
CH2 |
|
|
CH3 |
CH3 |
|
|
|
|
|
|
|
|
|||||||
|
CH |
3 |
CH3 |
|
|
|
|
CH |
2 |
CH2 |
CH2 |
CH |
|
|
|
|
|
|
|
|
|
|
|
|
CH3 |
||
Methamphetamine (controlled substance) |
|
|
|
|
|
Sibutramine |
|||||||
Luellmann, Color Atlas of Pharmacology © 2005 Thieme
All rights reserved. Usage subject to terms and conditions of license.