334 Therapy of Selected Diseases
Migraine
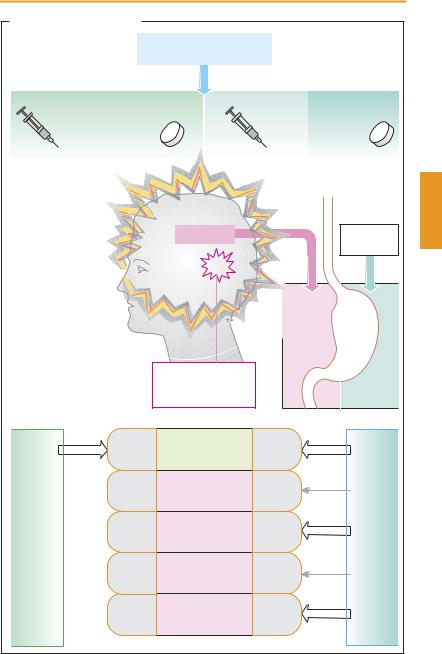
Migraine is a syndrome characterized by recurrent attacks of intense headache and nausea that occur at irregular intervals and last for several hours. In classical migraine, the attack is typically heralded by an “aura” accompanied by spreading homonymous visual field defects with colored sharp edges (“fortification” spectra). In addition, the patient cannot focus on certain objects, has a ravenous appetite for particular foods, and is hypersensitive to odors (hyperosmia) or light (photophobia). The exact cause of these complaints is unknown; conceivably, the underlying pathogenetic mechanisms involve local release of proinflammatory mediators from nociceptive primary afferents (neurogenic inflammation) or a disturbance in cranial blood flow. In addition to an often inherited predisposition, precipitating factors are required to provoke an attack, e. g., psychic stress, lack of sleep, certain foods. Pharmacotherapy of migraine has two aims: stopping the acute attack and preventing subsequent ones.
Treatment of the attack. For symptomatic relief, headaches are treated with analgesics (acetaminophen, acetylsalicylic acid), and nausea is treated with metoclopramide (pp.116, 342) or domperidone. Since there is delayed gastric emptying during the attack, drug absorption can be markedly retarded and hence effective plasma levels are not obtained. Because metoclopramide stimulates gastric emptying, it promotes absorption of ingested analgesic drugs and thus facilitates pain relief.
If acetylsalicylic acid is administered i.v. as the lysine salt, its bioavailability is complete. Therefore, i.v. injection may be advisable in acute attacks.
Should analgesics prove insuf ciently effective, sumatriptan (prototype of the triptans) or ergotamine may help prevent an imminent attack in many cases. Both substances are effective in migraine and cluster
headaches but not in other forms of headache. The probable common mechanism of action is a stimulation of serotonin receptors of the 5-HT1D subtype. Moreover, ergotamine has af nity for dopamine receptors (†nausea, emesis), as well as α-adrenocep- tors and 5-HT2 receptors (⁄ vascular tone, ⁄ platelet aggregation). With frequent use, the vascular side effects may give rise to severe peripheral ischemia (ergotism). Paradoxically, overuse of ergotamine (> once per week) may provoke “rebound” headaches, thought to result from persistent vasodilation. Though different in character (tensiontype headache), these prompt further consumption of ergotamine. Thus, a vicious circle develops with chronic abuse of ergotamine or other analgesics that may end with irreversible disturbances of peripheral blood flow and impairment of renal function.
Administered orally, ergotamine and sumatriptan have only limited bioavailability. Dihydroergotamine may be given by i.m. or slow i.v. injection, sumatriptan subcutaneously, by nasal spray, or as a suppository. When given orally, other triptans such as zolmitriptan, naratriptan, and rizatriptan have higher bioavailability than sumatriptan.
Prophylaxis. Taken regularly over a longer period, a heterogeneous group of drugs comprising propranolol, nadolol, atenolol, and metoprolol (β-blockers), flunarizine (H1-his- tamine, dopamine, and calcium antagonist), pizotifen (pizotyline, 5-HT antagonist with structural resemblance to tricyclic antidepressants), and methysergide (partial 5-HT antagonist) may decrease the frequency, intensity, and duration of migraine attacks. The drug of first choice is one of the β-block- ers mentioned.
Luellmann, Color Atlas of Pharmacology © 2005 Thieme
All rights reserved. Usage subject to terms and conditions of license.
|
|
|
|
|
Migraine |
335 |
A: Migraine and its treatment |
|
|
|
|
|
|
Acetylsalicylic acid 1000 mg |
|
|
|
or acetaminophen 1000 mg |
|
|
When therapeutic effect inadequate |
|
|
|
|
Sumatriptan |
or |
(Dihydro)-Ergotamine |
|
and other triptans |
|
|
|
|
|
6 mg |
50–100 mg |
|
|
1 mg |
1–2 mg |
|
|
Migraine |
|
|
|
Meto- |
|
|
|
|
|
|
clopramide |
Migraine attack: |
|
|
|
|
Gastric emptying |
|
|
|
|
|
Headache |
|
|
|
inhibited |
accelerated |
Hypersensitivity of |
|
|
|
|
|
|
|
|
|
olfaction, gustation, |
|
|
|
|
|
|
audition, vision, |
|
|
|
|
|
|
nausea, vomiting |
|
|
|
|
Drug |
|
|
|
Neurogenic |
|
|
|
|
|
|
|
absorption |
|
|
inflammation, |
|
|
|
|
|
|
local edema, |
|
delayed |
improved |
|
|
vasodilation |
|
|
|
|
|
5-HT1B/1D |
Relief of migraine |
|
5-HT1B/1D |
|
|
Sumatriptan and other triptans |
5-HT1A |
Psychosis |
|
5-HT1A |
|
|
D2 |
Nausea, |
|
D2 |
|
Ergotamine |
|
vomiting |
|
|
|
5-HT2 |
Platelet aggregation |
5-HT2 |
|
|
|
|
|
α 1 + α 2 |
Vasoconstriction |
|
α 1 + α 2 |
|
|
Luellmann, Color Atlas of Pharmacology © 2005 Thieme
All rights reserved. Usage subject to terms and conditions of license.
336 Therapy of Selected Diseases
Common Cold
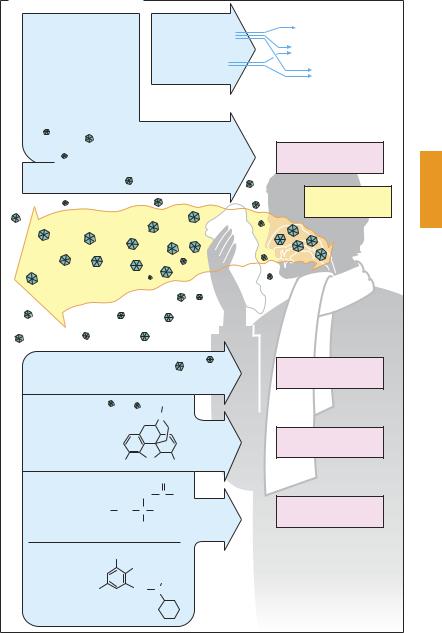
The common cold—colloquially the flu, catarrh, or grippe (strictly speaking the rarer infection with influenza viruses)—is an acute infectious inflammation of the upper respiratory tract. Its symptoms—sneezing, running nose (due to rhinitis), hoarseness (laryngitis), dif culty in swallowing and sore throat (pharyngitis and tonsillitis), cough associated with first serous then mucous sputum (tracheitis, bronchitis), sore muscles, and general malaise—can be present individually or concurrently in varying combination or sequence. The term stems from an old popular belief that these complaints are caused by exposure to chilling or dampness. The causative pathogensare differentviruses (rhino-, adeno-, and parainfluenza viruses) that may be transmitted by aerosol droplets produced by coughing and sneezing.
Therapeutic measures. Causal treatment with a virustatic is not possible at present. Since cold symptoms abate spontaneously, there is no compelling need to use drugs. However, conventional remedies are intended for symptomatic relief.
Rhinitis. Nasal discharge could be prevented by parasympatholytics; however, other atropine-like effects (p.108) would have to be accepted. Parasympatholytics are threfore hardly ever used, although a corresponding action is probably exploited in the case of H1-antihistaminics, an ingredient of many cold remedies. Locally applied (nasal drops), vasoconstricting α-sympatho- mimetics decongest the nasal mucosa and dry up secretions, clearing the nasal passage. Long-term use may cause damage to nasal mucous membranes (p. 94).
Sore throat, swallowing problems. Demulcent lozenges containing surface anesthetics such as lidocaine (caveat: benzocaine and tetracaine contain an allergenic p-ami- nophenyl group; p. 207) may provide shortterm relief; however, the risk of allergic reactions should be kept in mind.
Cough. Since coughing serves to expel excess tracheobronchial secretions, suppression of this physiological reflex is justified only when coughing is dangerous (after surgery) or unproductive because of absent secretions. Codeine and noscapine (p. 210) suppress cough by a central action. A different, though incompletely understood, mechanism of action is evident in antitussives such as clobutinol, which do not derive from opium. The available clinical studies concerning the benefits of antitussives in common colds do not present a convincing picture.
Mucous airway obstruction. Expectorants are meant to promote clearing of bronchial mucus by a liquefying action that involves either cleavage of mucous substances (mucolytics) or stimulation of production of watery mucus (e.g., hot beverages). Whether mucolytics are indicated in the common cold and whether expectorants such as bromohexine or ambroxole effectively lower viscosity of bronchial secretions may be questioned. In clinical studies of chronic obstructive bronchitis (but not common cold infections), N-acetylcysteine was shown to have clinical effectiveness, as evidenced by a lowered incidence of exacerbations during chronic intake.
Fever. Antipyretic analgesics (acetylsalicylic acid, acetaminophen, p.198) are indicated only when there is high fever. Fever is a natural response and useful in monitoring the clinical course of an infection.
Muscle aches and pains, headache. Antipyretic analgesics are effective in relieving these symptoms.
Luellmann, Color Atlas of Pharmacology © 2005 Thieme
All rights reserved. Usage subject to terms and conditions of license.
A. Drugs used in common cold
Local use of |
Acetylsalicylic acid |
Soreness |
|
α -sympathomimetics |
|
Headache |
(nasal drops or spray) |
Acetaminophen |
|
|
Fever |
|
|
|
|
|
Mucosal decongestion
Nose breathing facilitated
Caution: habituation
H1-Antihistamines
Caution: sedation
Viral infection
Causal therapy impossible
Surface anesthetics
Caution:
risk of sensitization
Antitussive: |
|
|
CH3 |
|
|
|
|
|
|
N |
Codeine |
O |
|
|
H3CO |
OH |
|
|
Mucolytics |
|
|
O |
|
|
|
|
|
NH |
C CH3 |
|
HS CH2 |
C |
COOH |
Acetylcysteine |
H |
|
|
|
Give |
Br |
|
|
warm fluids |
|
NH2 |
|
Elderberry |
|
|
CH3 |
Br |
CH2 |
N |
tea |
|
|
|
Bromhexine
Sniffles, runny nose
Common cold
Flu
Sore throat
Cough
Airway congestion
Accumulation in airways of mucus, inadequate expulsion by cough
Luellmann, Color Atlas of Pharmacology © 2005 Thieme
All rights reserved. Usage subject to terms and conditions of license.
338 Therapy of Selected Diseases
Atopy and Antiallergic Therapy
Atopy denotesa hereditary predisposition for IgE-mediated allergic reactions. Clinical pictures include allergic rhinoconjunctivitis (“hay fever”), bronchial asthma, atopic dermatitis (neurodermatitis, atopic eczema) and urticaria.Evidently,differentiationofT-helper (TH) lymphocytes toward the TH2 phenotype is the common denominator. Therapeutic interventions are aimed at different levels to influence pathophysiological events (A).
1. Specific immune therapy (“hyposensitization”) with intracutaneous antigen injections is intended to shift TH cells in the direction of TH1.
2. Inactivation of IgE can be achieved by means of the monoclonal antibody, omalizumab. This is directed against the Fc portion of IgE and prevents its binding to mast cells.
3. Stabilization of mast cells. Cromolyn prevents IgE-mediated release of mast cell mediators, although only after chronic treatment. It is applied locally to conjunctiva, nasal mucosa, the bronchial tree (inhalation), and intestinal mucosa (absorption is almost nil with oral intake). Indications: prophylaxis of hay-fever, allergic asthma, and food allergies. Nedocromil acts similarly.
4. Blockade of histamine receptors. Allergic reactions are predominantly mediated by H1 receptors. H1-antihistaminics (p.118) are mostly used orally. Their therapeutic effect is often disappointing. Indications: allergic rhinitis (hay fever).
5. Blockade of leukotriene receptors. Montelukast is an antagonist at receptors for (cysteinyl) leukotriene. Leukotrienes evoke intense bronchoconstriction and promote allergic inflammation of the bronchial mucosa. Montelukast is used for oral prophylaxis of bronchial asthma. It is effective in analgesiainduced asthma (pp. 200, 340) and exercise-
6. Functional antagonists of mediators of allergy.
a α-Sympathomimetics, such as naphazoline, oxymetazoline, and tetrahydrozoline, are applied topically to the conjunctival and nasal mucosa to produce local vasoconstriction. Their use should be shortterm at most.
b Epinephrine, given i.v., is the most important drug in the management of anaphylactic shock: it constricts blood vessels, reduces capillary permeability, and dilates bronchi.
c β2-Sympathomimetics, such as terbutaline, fenoterol, and albuterol, are employed in bronchial asthma, mostly by inhalation, and parenterally in emergencies. Even after inhalation, effective amounts can reach the systemic circulation and cause side effects (e. g., palpitations, tremulousness, restlessness, hypokalemia). The duration of action of both salmeterol and formoterol, given by inhalation, is 12 hours. These long-acting β2-mimetics are included in the treatment of severe asthma. Given at nighttime, they can prevent attacks that preferentially occur in the early morning hours.
d Theophylline belongs to the methylxanthines. Its effects are attributed to both inhibition of phosphodiesterase (cAMP increase, p. 66) and antagonism at adenosine receptors. In bronchial asthma, theophylline can be given orally for prophylaxis or parenterally to control the attack. Manifestations of overdosage include ton- ic-clonic seizures and cardiac arrhythmias (blood level monitoring).
e Glucocorticoids (p.244) have significant antiallergic activity and probably interfere with different stages of the allergic response. Indications: hay fever, bronchial asthma (preferably local application of analogues with high presystemic elimination, e.g., beclomethasone dipropionate, budesonide, flunisolide, fluticasone propionate); and anaphylactic shock (i.v. in high dosage)—a probably nongenomic action of
inducedLuellmann,bronchospasmColor Atlas. of Pharmacology © 2005immediateThieme onset.
All rights reserved. Usage subject to terms and conditions of license.
|
|
|
|
Antiallergie Therapy |
|
339 |
A. Atopy and antiallergic therapy |
|
|
|
|
|
|
|
|
|
|
TH1 |
|
TH0 |
|
TH2 |
|
|
|
|
|
|
|
Skin |
|
IgE |
|
Atopy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Anti- |
Allergen |
|
|
|
Mast cell |
|
|
|
|
gen |
|
|
|
|
|
|
|
|
|
|
stabilization by |
|
|
|
|
|
|
|
|
|
Specific |
|
|
|
|
cromolyn |
|
|
|
|
immunotherapy |
|
|
|
|
|
OH |
|
|
|
|
IgE |
|
|
|
CH2 |
C |
CH2 |
|
|
|
Glucocorticoids |
|
|
|
|
O |
O |
H |
O |
O |
|
|
|
|
|
|
|
|
|
|
|
Mast cell |
|
|
|
|
|
|
|
|
Omalizumab |
|
-OOC |
O |
|
|
|
O |
COO- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Histamine |
|
Leukotrienes |
|
|
|
|
|
|
H1-Antihistaminics |
|
|
|
|
Antileukotriene, |
|
|
|
|
|
|
e.g., montelukast |
|
|
|
Histamine |
|
|
Leukotriene |
|
|
|
|
|
receptor |
|
|
receptor |
|
|
|
|
|
Reaction of target cells |
|
|
|
|
|
|
|
|
|
Vascular smooth muscle, permeability |
|
Bronchial musculature |
|
|
|
Vasodilation |
Edema |
|
|
|
|
Contraction |
|
|
|
|
|
|
|
|
Bronchial asthma |
|
α -Sympatho- Mucous membranes |
|
|
β |
2-Sympathomimetics: |
mimetics: |
of nose and eye: |
|
|
e. g., |
redness, swelling, |
|
|
e. g., terbutaline |
|
naphazoline |
secretion |
|
|
|
HO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CH3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CH |
|
CH2 |
N C |
CH3 |
Vaso- |
|
|
Broncho- |
|
|
|
|
|
H |
|
|
|
HO |
|
OH |
|
|
CH3 |
constriction |
|
|
dilation |
|
|
|
|
|
|
Skin: |
|
|
|
Theophylline |
|
|
|
|
|
|
|
|
|
wheal formation |
|
|
|
|
|
|
O |
H |
|
|
|
|
|
|
|
|
H3C |
|
|
|
|
|
|
|
|
|
|
|
|
N |
|
|
Circulation: |
|
|
|
|
|
N |
|
|
Epinephrine |
|
|
|
|
|
|
|
|
anaphylactic shock |
|
|
|
|
O |
|
N |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CH3 |
|
|
Luellmann, Color Atlas of Pharmacology © 2005 Thieme
All rights reserved. Usage subject to terms and conditions of license.