

- •Preface to the 3rd edition
- •General Pharmacology
- •Systems Pharmacology
- •Therapy of Selected Diseases
- •Subject Index
- •Abbreviations
- •General Pharmacology
- •History of Pharmacology
- •Drug and Active Principle
- •The Aims of Isolating Active Principles
- •European Plants as Sources of Effective Medicines
- •Drug Development
- •Congeneric Drugs and Name Diversity
- •Oral Dosage Forms
- •Drug Administration by Inhalation
- •Dermatological Agents
- •From Application to Distribution in the Body
- •Potential Targets of Drug Action
- •External Barriers of the Body
- •Blood–Tissue Barriers
- •Membrane Permeation
- •Binding to Plasma Proteins
- •The Liver as an Excretory Organ
- •Biotransformation of Drugs
- •Drug Metabolism by Cytochrome P450
- •The Kidney as an Excretory Organ
- •Presystemic Elimination
- •Drug Concentration in the Body as a Function of Time—First Order (Exponential) Rate Processes
- •Time Course of Drug Concentration in Plasma
- •Time Course of Drug Plasma Levels during Repeated Dosing (A)
- •Time Course of Drug Plasma Levels during Irregular Intake (B)
- •Accumulation: Dose, Dose Interval, and Plasma Level Fluctuation (A)
- •Dose–Response Relationship
- •Concentration–Effect Curves (B)
- •Concentration–Binding Curves
- •Types of Binding Forces
- •Agonists—Antagonists
- •Other Forms of Antagonism
- •Enantioselectivity of Drug Action
- •Receptor Types
- •Undesirable Drug Effects, Side Effects
- •Drug Allergy
- •Cutaneous Reactions
- •Drug Toxicity in Pregnancy and Lactation
- •Pharmacogenetics
- •Placebo (A)
- •Systems Pharmacology
- •Sympathetic Nervous System
- •Structure of the Sympathetic Nervous System
- •Adrenergic Synapse
- •Adrenoceptor Subtypes and Catecholamine Actions
- •Smooth Muscle Effects
- •Cardiostimulation
- •Metabolic Effects
- •Structure–Activity Relationships of Sympathomimetics
- •Indirect Sympathomimetics
- •Types of
- •Antiadrenergics
- •Parasympathetic Nervous System
- •Cholinergic Synapse
- •Parasympathomimetics
- •Parasympatholytics
- •Actions of Nicotine
- •Localization of Nicotinic ACh Receptors
- •Effects of Nicotine on Body Function
- •Aids for Smoking Cessation
- •Consequences of Tobacco Smoking
- •Dopamine
- •Histamine Effects and Their Pharmacological Properties
- •Serotonin
- •Vasodilators—Overview
- •Organic Nitrates
- •Calcium Antagonists
- •ACE Inhibitors
- •Drugs Used to Influence Smooth Muscle Organs
- •Cardiac Drugs
- •Cardiac Glycosides
- •Antiarrhythmic Drugs
- •Iron Compounds
- •Prophylaxis and Therapy of Thromboses
- •Possibilities for Interference (B)
- •Heparin (A)
- •Hirudin and Derivatives (B)
- •Fibrinolytics
- •Intra-arterial Thrombus Formation (A)
- •Formation, Activation, and Aggregation of Platelets (B)
- •Inhibitors of Platelet Aggregation (A)
- •Presystemic Effect of ASA
- •Plasma Volume Expanders
- •Lipid-lowering Agents
- •Diuretics—An Overview
- •NaCl Reabsorption in the Kidney (A)
- •Aquaporins (AQP)
- •Osmotic Diuretics (B)
- •Diuretics of the Sulfonamide Type
- •Potassium-sparing Diuretics (A)
- •Vasopressin and Derivatives (B)
- •Drugs for Gastric and Duodenal Ulcers
- •Laxatives
- •Antidiarrheal Agents
- •Drugs Affecting Motor Function
- •Muscle Relaxants
- •Nondepolarizing Muscle Relaxants
- •Depolarizing Muscle Relaxants
- •Antiparkinsonian Drugs
- •Antiepileptics
- •Pain Mechanisms and Pathways
- •Eicosanoids
- •Antipyretic Analgesics
- •Nonsteroidal Anti-inflammatory Drugs (NSAIDs)
- •Cyclooxygenase (COX) Inhibitors
- •Local Anesthetics
- •Opioid Analgesics—Morphine Type
- •General Anesthesia and General Anesthetic Drugs
- •Inhalational Anesthetics
- •Injectable Anesthetics
- •Sedatives, Hypnotics
- •Benzodiazepines
- •Pharmacokinetics of Benzodiazepines
- •Therapy of Depressive Illness
- •Mania
- •Therapy of Schizophrenia
- •Psychotomimetics (Psychedelics, Hallucinogens)
- •Hypothalamic and Hypophyseal Hormones
- •Thyroid Hormone Therapy
- •Glucocorticoid Therapy
- •Follicular Growth and Ovulation, Estrogen and Progestin Production
- •Oral Contraceptives
- •Antiestrogen and Antiprogestin Active Principles
- •Aromatase Inhibitors
- •Insulin Formulations
- •Treatment of Insulin-dependent Diabetes Mellitus
- •Treatment of Maturity-Onset (Type II) Diabetes Mellitus
- •Oral Antidiabetics
- •Drugs for Maintaining Calcium Homeostasis
- •Drugs for Treating Bacterial Infections
- •Inhibitors of Cell Wall Synthesis
- •Inhibitors of Tetrahydrofolate Synthesis
- •Inhibitors of DNA Function
- •Inhibitors of Protein Synthesis
- •Drugs for Treating Mycobacterial Infections
- •Drugs Used in the Treatment of Fungal Infections
- •Chemotherapy of Viral Infections
- •Drugs for the Treatment of AIDS
- •Drugs for Treating Endoparasitic and Ectoparasitic Infestations
- •Antimalarials
- •Other Tropical Diseases
- •Chemotherapy of Malignant Tumors
- •Targeting of Antineoplastic Drug Action (A)
- •Mechanisms of Resistance to Cytostatics (B)
- •Inhibition of Immune Responses
- •Antidotes and Treatment of Poisonings
- •Therapy of Selected Diseases
- •Hypertension
- •Angina Pectoris
- •Antianginal Drugs
- •Acute Coronary Syndrome— Myocardial Infarction
- •Congestive Heart Failure
- •Hypotension
- •Gout
- •Obesity—Sequelae and Therapeutic Approaches
- •Osteoporosis
- •Rheumatoid Arthritis
- •Migraine
- •Common Cold
- •Bronchial Asthma
- •Emesis
- •Alcohol Abuse
- •Local Treatment of Glaucoma
- •Further Reading
- •Further Reading
- •Picture Credits
- •Drug Indexes
344 Therapy of Selected Diseases
Alcohol Abuse
Since prehistoric times, ethanol-containing beverages have enjoyed widespread use as a recreational luxury. What applies to any medicinal substance also holds for alcohol: the dose alone makes the poison (see p. 2). Excessive, long-term consumption of alcoholic drinks, or alcohol abuse, is harmful to the affected individual. Alcoholism must be considered a grave disorder that plays a major role in terms of numbers alone; for instance, in Germany 1 000 000 people are affected by this self-inflicted illness.
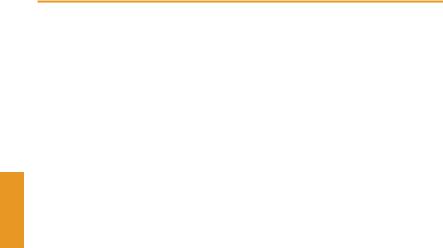
Ethanol is miscible with water and is well lipid-soluble, enabling it to penetrate easily through all barriers in the organism; the blood–brain barrier and the placental barrier are no obstacles. In liver cells, alcohol is broken down to acetic acid via acetaldehyde (A). Ethyl alcohol is never ingested as a chemically pure substance but in the form of an alcoholic beverage that contains flavoring agents and higher alcohols, depending on its origin. The effect desired by the consumer takes place in the brain: ethanol acts as a stimulant, it disinhibits, and it enhances sociability, as long as the beverage is enjoyed in moderate quantities. After higher doses, self-critical faculties are lost and motor function is impaired–the familiar picture of the drunk. Still higher doses induce a comatose state (caution: hypothermia and respiratory paralysis). The complex effects on the CNS cannot be ascribed to a simple mechanism of action. An inhibitory effect on the NMDA subtype of glutamate receptor appears to predominate.
In chronic alcohol abuse, mainly two organs are damaged:
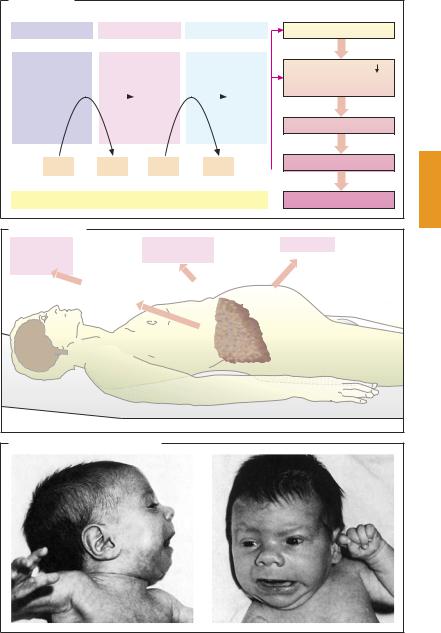
1.In the liver, hepatocytes may initially undergo fatty degeneration, this process being reversible. With continued exposure, liver cells die and are replaced by connective tissue newly formed from myofibroblasts: liver cirrhosis. Hepatic blood flow is greatly reduced; the organ becomes unable to fulfill its detoxification
function (danger of hepatic coma). Collateral circulation routes develop (bleeding from esophageal varicose veins) with production of ascites. Alcoholic liver cirrhosis is a severe, mostly progressive disease that permits only symptomatic therapy (B).
2.The functional capacity of the brain is impaired. Irreversible damage may manifest in a measurable fallout of neuronal cell bodies. Often delirium tremens develops (usually triggered by alcohol withdrawal), whichcanbemanagedwithintensivetherapy (clomethiazole, haloperidol, among others). In addition, alcoholic hallucinations and Wernicke–Korsakow syndrome
occur. All of these are desolate states.
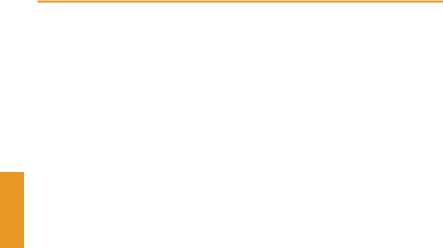
It must be pointed out specifically that alcohol abuse during pregnancy leads to (em- bryo–fetal alcohol syndrome (malformations, persistent intellectual deficits). This intrauterine intoxication is relatively common: one case per 1000 births (C).
Chronic alcohol abuse is an expression of true dependence. Thus, therapy of this addiction is dif cult and frequently without success. There is no pharmacotherapeutic silver bullet (the NMDA receptor antagonist acamprosate may be worth trying). Above all, psychotherapeutic care, a change in milieu, and supportive treatment with benzodiazepines are important.
Luellmann, Color Atlas of Pharmacology © 2005 Thieme
All rights reserved. Usage subject to terms and conditions of license.
Alcohol Abuse |
345 |
A. Alcoholism |
|
|
Ethanol |
Acetaldehyde |
Acetic acid |
H3C |
H3C |
H3C |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
H2COH |
|
HC=O |
|
COOH |
|
||||||
|
|
NAD+ |
NADH |
|
|
NAD+ |
NADH |
|
|
||
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
Main catabolic pathway of ethanol in liver cell
Quotient NADH/NAD+
Fatty acid oxidation Fatty acid synthesis Triglyceride synthesis
Triglyceride synthesis
Fatty liver
Cell necroses
Cirrhosis
B. Liver cirrhosis |
|
|
Hepatic |
Esophageal and |
Ascites |
encepha- |
gastric varices |
|
lopathy |
|
|
Insufficient |
|
Portal |
presystemic |
|
hypertension |
elimination |
|
|
of NH3 |
|
|
|
|
Liver cirrhosis |
C. Embryo-fetal alcohol syndrome
Luellmann, Color Atlas of Pharmacology © 2005 Thieme
All rights reserved. Usage subject to terms and conditions of license.
346 Therapy of Selected Diseases
Local Treatment of Glaucoma
Currently, glaucoma therapy remains focused on mechanisms designed to decrease intraocular pressure (IOP) and this approach is considered effective also in normal tension glaucoma.
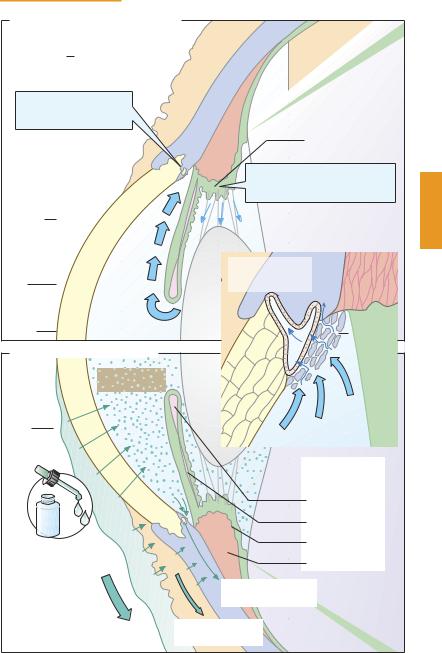
Normal values of IOP lie between 15 and 20 mmHg, that is, above the venous pressure. IOP reflects the ratio of production and outflow of aqueous humor. Aqueous humor is secreted by the epithelial cells of the ciliary body and, following passage through the trabecular meshwork, is drained via the canal of Schlemm (blue arrows in A). This route is taken by 85–90% of aqueous humor; a smaller portion enters the uveoscleral vessels and, thus, the venous system. In the socalled open-angle glaucoma, passage of aqueous humor through the trabecular meshwork is impeded so that drainage through Schlemm’s canal becomes inef - cient. The much rarer primary angle-closure glaucoma features a narrowed iridocorneal angle or a tight contact between iris and lens (‘pupillary block’). Secondarily, blockade by the iris of the trabecular meshwork may be due to various causes (e. g., synechiae). Topographical relationships in the chamber angle are shown enlarged in the red box.
For topical therapy of open-angle glaucoma, the following groups of drugs can be used: for reducing production of aqueous humor, β-blockers (e. g., timolol), α2-agonists (clonidine, brimonidine), and inhibitors of carbonic anhydrase (dorzolamide, brinzolamide).
For promoting drainage through the trabecular meshwork, parasympathomimetics (e. g., pilocarpine) are effective, and through the uveoscleral route, prostaglandin derivatives. Pilocarpine excites the ciliary muscle and the pupillary sphincter. The contraction of both muscles widens the geometrical arrangement of trabeculae, resulting in improved drainage of aqueous humor. Uveoscleral drainage is augmented by the prostaglandin derivatives lanatoprost and bimato-
prost. Both substances can be used for topical monotherapy or combined with other active principles. A peculiar side effect is notable: dark pigmentation of iris and eyelashes.
The therapy of angle-closure glaucoma involves chiefly reduction of aqueous humor production (osmotic agents, β-blockers) and surgical procedures.
The topical application of pharmaceuticals in the form of eye-drops is hampered by a pharmacokinetic problem. The drug must penetrate from the ocular surface (cornea and conjunctiva) to its target sites, namely, the smooth muscle of the ciliary body or the iris, the secretory epithelium of the ciliary body, or the uveoscleral vessels (B). The applied drug concentration is diluted by lacrimal fluid and drains via the tear duct to the nasal mucosa, where the drug may be absorbed. During permeation through the cornea, transport through blood vessels takes place. The drug concentration reaching the anterior chamber is diluted by aqueous humor and, finally, drug molecules are also transported away via Schlemm’s canal. In order to reach the required concentrations at the target site (10–8 to 10–6 M, depending on the substance), the concentration needed in the eye drops is ~ 10–2 M (equivalent to ~ 0.5 mg per droplet, depending on molecular weight). The amount of drug contained in a single drop is large enough to elicit a general reaction with systemic use. Even when applied properly, eye drops can therefore evoke side effects in the cardiovascular system or the bronchial space. This possibility leads to corresponding contraindications. Thus, in patients with severe congestive heart failure, bradycardia, or obstructive lung disease, eye drops containing β-block- ers must be avoided at all times.
Luellmann, Color Atlas of Pharmacology © 2005 Thieme
All rights reserved. Usage subject to terms and conditions of license.
A. Local pharmacotherapy of glaucoma
Conjunctiva
Increased drainage
Pilocarpine
Prostaglandin derivatives
Schlemm’s canal
Cornea
Iris
Local Treatment of Glaucoma |
347 |
Sclera
M. ciliaris
Proc. ciliaris
Inhibitors of aqueous humor production: β -Blocker, CAH-inhibitors, α 2-agonist
|
Aqueous humor |
Schlemm’s canal |
Sclera M. ciliaris |
(drainage into |
|
venous system) |
|
Lens |
|
|
|
Trabecular |
|
|
|
|
labyrinth |
B. Diffusion barriers for eye drops |
|
|
||
|
Concentration: |
|
|
|
|
~ |
10-7M |
|
|
|
|
|
|
|
Tear |
|
|
Cornea |
Iris |
|
|
|
|
|
film |
|
|
|
|
|
|
|
Aqueous humor |
|
|
|
|
|
Potential target |
|
|
|
|
organs: |
|
|
|
|
M. sphincter pup. |
|
|
|
|
M. dilatator pup. |
Eye drops |
|
|
Ciliary epithelium |
|
|
|
|
||
Concentration: |
|
|
M. ciliaris |
|
~ |
10-2M |
|
|
|
|
|
|
|
|
|
|
|
Removal through |
|
|
|
|
Schlemm’s canal |
|
|
|
to nasal |
Removal through |
|
|
|
mucosa |
blood vessels |
|
Luellmann, Color Atlas of Pharmacology © 2005 Thieme
All rights reserved. Usage subject to terms and conditions of license.

Luellmann, Color Atlas of Pharmacology © 2005 Thieme
All rights reserved. Usage subject to terms and conditions of license.