
extrapyramidal motor disturbances, Parkin-
|
Other Tropical Diseases |
son-like signs, coma, and death. Therapy: |
|||||
|
|
||||||
|
In addition to malaria, other tropical diseases |
Long-term suramine i.v. or pentamidine(less |
|||||
|
and their treatment will be considered for |
effective); |
arsenicals |
(e.g., |
melarsoprol, |
||
|
the following reasons. (1) Owing to the tre- |
highly toxic), when the CNS is involved. |
|||||
|
mendous growth in global travel, inhabitants |
T. cruzi is confined to Central and South |
|||||
|
of temperate climatic zones have become |
America and transmitted by blood-sucking |
|||||
|
exposed to the hazard of infection with trop- |
reduviid bugs. These parasites preferentially |
|||||
|
ical disease pathogens. (2) The spread of |
infiltrate the cardiac musculature, where |
|||||
|
some tropical diseases is of unimaginable |
they cause damage to muscle fibers and the |
|||||
|
dimensions, with humans victims number- |
specialized conducting tissue. Death results |
|||||
|
ing in the millions. The pharmacotherapeutic |
from cardiac failure. Therapy: unsatisfactory. |
|||||
|
|||||||
|
possibilitiesknown to date will be presented. |
|
|
|
|
|
|
|
|
Schistosomiasis |
(bilharziasis) |
(see |
also |
||
|
Amebiasis. The causative agent, Entamoeba |
p.292). The causative organisms are trema- |
|||||
|
histolytica, lives and multiplies in the colon |
todes with a complex life cycle that need |
|||||
|
(symptom: diarrhea), its cyst form residing |
(aquatic) snails as intermediate hosts. Free- |
|||||
|
also in the liver among other sites. In tropical |
swimming larval cercariae penetrate the in- |
|||||
|
regions, up to half the population can be |
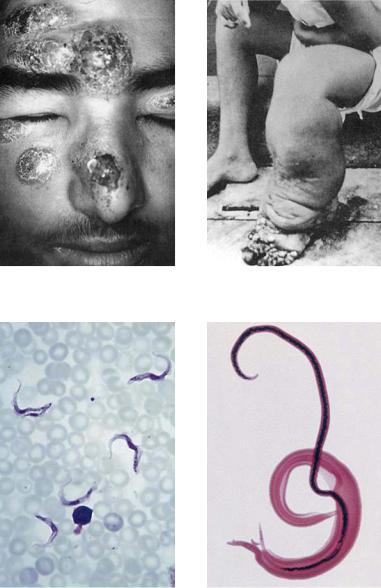
tact skin of humans. The adult worms (Schis- |
|||||
|
infested, transmission occurring by the fe- |
tosoma mansoni, D) livein thevenousvascu- |
|||||
|
cal–oral route. The most effective treatment |
lature. Occurrence: tropical countries rich in |
|||||
|
against both intestinal infestation and sys- |
aquatic habitats. About 200 million humans |
|||||
|
temic disease is administration of metroni- |
are af icted. Therapy: praziquantel, 10– |
|||||
|
dazole. If monotherapy fails, combination |
40 mg/kg,singledose,ishighlyeffectivewith |
|||||
|
therapy with chloroquine, emetine or tetra- |
minimal adverse effects. Substancesreleased |
|||||
|
cyclines may be indicated. |
from decaying worms may cause problems. |
|||||
|
Leishmaniasis. The causative agents are flag- |
Filariasis. In its microform, Wuchereria ban- |
|||||
|
ellated protozoa that are transmitted by |
crofti istransmittedbymosquitoes;theadult |
|||||
|
sand flies to humans. The parasites are taken |
parasites live in the lymph system and cause |
|||||
|
up into phagocytes, where they remain in |
inflammations and blockage of lymph drain- |
|||||
|
phagolysosomes and multiply until the cell |
age leading to elephantiasis in extreme cases |
|||||
|
dies and the parasites can infect new cells. |
(B). Therapy: diethylcarbamazepine for sev- |
|||||
|
Symptoms: A visceral form, known as kala- |
eral weeks; adverse reactions are chiefly due |
|||||
|
azar, and cutaneous or mucocutaneous |
to products from disintegrating worms. |
|||||
|
forms exist (A). An estimated 12 million hu- |
|
|
|
|
|
|
|
mans are affected. Therapy is dif cult; pen- |
Onchocerciasis (“River Blindness”). The |
|||||
|
tavalent antimonial compounds, such as sti- |
causative organism is Onchocerca volvulus, |
|||||
|
bogluconate, must be given for extended |
a filaria transmitted by black flies (genus |
|||||
|
periods. Adverse effects are pronounced. |
Simulium). The adult parasites (several cen- |
|||||
|
|
timeters long) form tangles and proliferating |
|||||
|
Trypanosomiasis. The pathogens, Trypano- |
nodules (onchocercomas) in the skin and |
|||||
|
soma brucei (sleeping sickness) and T. cruzi |
have a particular propensity for invading |
|||||
|
(Chagas disease), are flagellated protozoa. T. |
the eyeball, resulting in blindness. About 20 |
|||||
|
brucei (C) is transmitted by the tsetse fly, |
million people inhabiting banks of fast-flow- |
|||||
|
distributed in West and East Africa. An initial |
ing rivers are af |
icted with river blindness. |
||||
|
stage (swelling of lymph nodes, malaise, |
Therapy: |
ivermectin |
(0.15 mg/kg, |
single |
||
|
hepatosplenomegaly, among others) is fol- |
dose); adverse reactions are in part caused |
|||||
|
lowedLuellmann,by invasionColor ofAtlastheofCNSPharmacologywith lethargy,© 2005by disintegratingThieme |
worms. |
|
|
|||
|
All rights reserved. Usage subject to terms and conditions of license. |
|
|
||||