


142 Antianemics
Iron Compounds
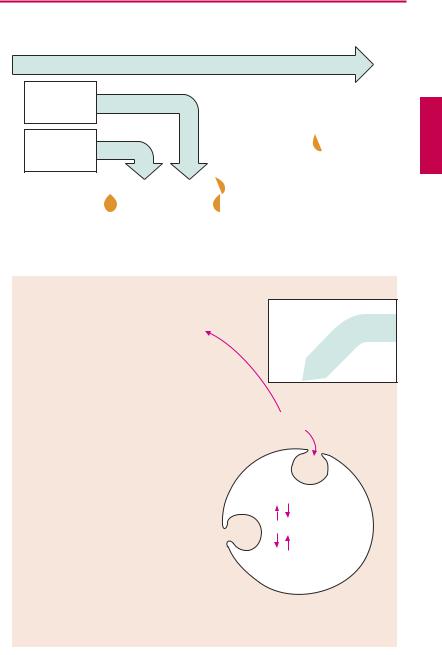
Not all iron ingested in food is equally absorbable. Trivalent Fe3+ is virtually not taken up from the neutral milieu of the small bowel, where the divalent Fe2+ is markedly better absorbed. Uptake is particularly ef cient in the form of heme (present in hemoglobin and myoglobin). Within the mucosal cells of the gut, iron is oxidized and either deposited as ferritin (see below) or passed on to the transport protein, transferrin. The amount absorbed does not exceed that needed to balance losses due to epithelial shedding from skin and mucosae or hemorrhage (socalled“mucosal block”). Inmenthisamount is ~ 1 mg/day, in women it is ~ 2 mg/day (because of menstrual blood loss); it corresponds to about 10% of the dietary intake. The transferrin–iron complex undergoes endocytotic uptake into erythrocyte precursors to be utilized for hemoglobin synthesis. About 70% of the total body store of iron (~ 5 g) is contained within erythrocytes. When these are degraded by macrophages of the mononuclear phagocyte system, iron is liberated from hemoglobin. Fe3+can be stored as ferritin (= protein apoferritin + Fe3+) or be returned to erythropoiesis sites via transferrin.
A frequent cause of iron deficiency is chronic blood loss due to gastric/intestinal ulcers or tumors. One liter of blood contains 500 mg of iron in healthy condition. Despite a significant increase in absorption rate, absorption isunable to keep up with lossesand the body store of iron falls. Iron deficiency results in impaired synthesis of hemoglobin and anemia.
The treatment of choice (after the cause of bleeding has been found and eliminated) consists in the oral administration of Fe2+- compounds, e.g., ferrous sulfate (daily dose 100 mg of iron, equivalent to 300 mg of FeSO4, divided into multiple doses). Replenishing of iron stores may take several months. Oral administration, however, is ad-
vantageous in that it is impossible to overload the body with iron through an intact mucosa because of its demand-regulated absorption (mucosal block).
Adverse effects. The frequent gastrointestinal complaints (epigastric pain, diarrhea, constipation) necessitate intake ofiron preparations with or after meals, although absorption is higher from the empty stomach.
Interactions. Antacids inhibit iron absorption. Combination with ascorbic acid (vitamin C) to protect Fe2+ from oxidation to Fe3+ is theoretically sound but practically is not needed.
Parenteral administration of Fe3+ salts is indicated only when adequate oral replacement is not possible. There is a risk of overdosage, with iron deposition in tissues (hemosiderosis). The binding capacity of transferrin is limited and free Fe3+ is toxic. Therefore, Fe3+complexes are employed that can donate Fe3+ directly to transferrin or can be phagocytosed by macrophages, enabling iron to be incorporated into the ferritin store. Possible adverse effects are: with i.m. injection, persistent pain at the injection site and skin discoloration; with i.v. injection, flushing, hypotension, anaphylactic shock.
Luellmann, Color Atlas of Pharmacology © 2005 Thieme
All rights reserved. Usage subject to terms and conditions of license.
|
|
Iron Compounds |
143 |
|
A. Iron: possible routes of administration and fate in the organism |
|
|
||
|
Fe(III) salts nonabsorbable |
|
|
|
Oral |
|
|
|
|
intake |
Fe(II) salts |
|
|
|
|
Heme-Fe |
|
|
|
|
|
Fe(III) |
|
|
Absorption |
|
Fe(III) |
|
|
Duodenum |
|
|
|
|
|
|
|
|
|
upper jejunum |
|
|
|
|
|
|
Ferritin |
|
|
|
|
Parenteral |
|
|
Transport |
|
administration |
|
|
Fe(III) |
Fe(III) |
|
|
|
Plasma |
|
|
||
|
|
|
|
|
|
Transferrin |
|
|
|
|
|
i.v. |
i.m. |
|
Uptake into |
Hemoglobin |
|
|
|
erythroblast |
|
Fe(III) complexes |
|
|
|
|
|
|
|
bone marrow |
|
|
|
|
|
|
Fe(III) |
|
|
Erythrocyte |
|
Ferritin |
|
|
|
|
|
|
|
blood |
|
|
|
|
|
|
Hemosiderin |
|
|
|
|
= aggregated |
|
|
|
|
ferritin |
|
|
Loss through |
|
Uptake into macrophages |
|
|
bleeding |
|
|
||
|
spleen, liver, bone marrow |
|
||
|
|
|
||
Luellmann, Color Atlas of Pharmacology © 2005 Thieme
All rights reserved. Usage subject to terms and conditions of license.

144 Antithrombotics
Prophylaxis and Therapy of Thromboses
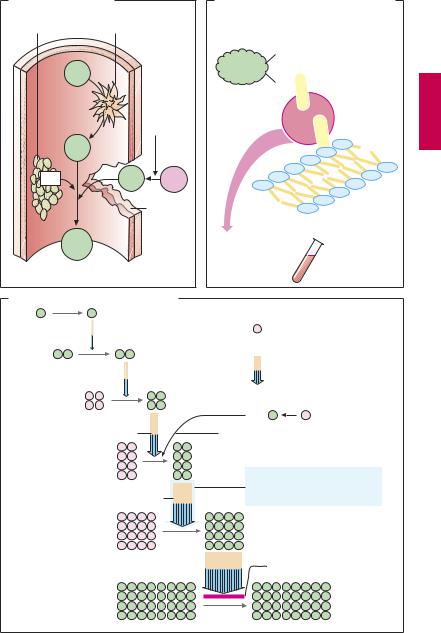
Upon vascular injury, the coagulation system is activated: thrombocytes and fibrin molecules coalesce into a “plug” that seals the defect and halts bleeding (hemostasis). Unnecessary formation of an intravascular clot—a thrombosis—can be life-threatening. If the clot forms on an atheromatous plaque in a coronary artery, myocardial infarction is imminent; a thrombus in a deep leg vein can be dislodged and carried into a lung artery and can cause pulmonary embolism.
Drugs that decrease the coagulability of blood, such as coumarins and heparin (A) are employed for the prophylaxis of thromboses. In addition, attempts are directed, by means of acetylsalicylic acid, at inhibiting the aggregation of blood platelets, which are prominently involved in intra-ar- terial thrombogenesis (p.152). For the therapy of thrombosis, drugs are used that dissolve the fibrin meshwork—fibrinolytics (p.150).
An overview of the coagulation cascade and sites of action for coumarins and heparin is shown in (A). There are two ways to initiate the cascade (B): (1) conversion of factor XII into its active form (XIIa, intrinsic system) at intravascular sites denuded of endothelium; (2) conversion of factor VII into VIIa (extrinsic system) under the influence of a tissue-derived lipoprotein (tissue thromboplastin). Both mechanisms converge via factor X into a common final pathway.
The clotting factors are protein molecules. “Activation” mostly means proteolysis (cleavage of protein fragments) and, with the exception of fibrin, conversion into proteinhydrolyzing enzymes (proteases). Some activated factors require the presence of phospholipids (PL) and Ca2+ for their proteolytic activity. Conceivably, Ca2+ ions cause the adhesion of factor to a phospholipid surface, as depicted in (B). Phospholipids are contained in platelet factor 3 (PF3), which is released from aggregated platelets, and in tissue
thromboplastin (A). The sequential activation of several enzymes allows the aforementioned reactions to “snowball” (symbolized in C by increasing number of particles), culminating in massive production of fibrin.
Ca2+-chelators (B) prevent the enzymatic activity of Ca2+-dependent factors; they contain COO– groups that bind Ca2+ ions (C): citrate and EDTA (ethylenediaminetetraacetic acid) form soluble complexes with Ca2+; oxalate precipitates Ca2+ as insoluble calcium oxalate. Chelation of Ca2+ cannot be used in vivo for therapeutic purposes because Ca2+ concentrations would have to be lowered to a level incompatible with life (hypocalcemic tetany). These compounds (sodium salts) are, therefore, used only for rendering blood incoagulable outside the body. This effect can be reversed at any time by addition of Ca2+ ions.
In vivo, the progression of the coagulation cascade can be inhibited as follows (C):
1.Coumarin derivatives decrease the blood concentrations of inactive factors II, VII, IX and X, by inhibiting their synthesis in the liver.
2.The complex consisting of heparin and antithrombin III neutralizes the protease activity of activated factors; unlike unfractionated heparin, low-molecular-weight heparin fragments or the “minimal molecular subunit of heparin,” fondaparinux, inhibit only activated factor Xa when complexed with antithrombin III.
3.Hirudin and its derivatives (bivalirudin, lepirudin) block the active center of thrombin.
Luellmann, Color Atlas of Pharmacology © 2005 Thieme
All rights reserved. Usage subject to terms and conditions of license.
Prophylaxis and Therapy of Thromboses |
145 |
A. Activation of clotting |
|
|
B. Inhibition of clotting by removal of Ca2+ |
|
Platelets |
Endothelial defect |
Clotting factor |
|
|
|
|
|
|
|
|
|
|
COO– |
|
XII |
|
|
COO– |
|
|
|
|
|
|
|
|
Tissue |
+ |
+ |
|
|
kinase |
Ca |
|
|
|
thrombo- |
|
|
XIIa |
|
|
|
– |
|
|
– |
– |
|
|
|
|
|
|
|
|
|
– |
|
PF3 |
VIIa |
VII |
– |
|
|
|
|
– |
|
|
|
Vessel |
|
Phospholipids, |
|
|
rupture |
|
|
|
|
|
e.g., PF3 |
|
|
|
|
|
|
Fibrin |
|
|
Ca2+ chelation |
|
|
|
|
Citrate |
only in vitro |
|
|
|
EDTA |
|
|
|
|
|
|
|
|
|
Oxalate |
|
C. Inhibition of clotting cascade in vivo |
|
|
||
XII |
XIIa |
|
|
|
|
|
Synthesis susceptible to |
|
|
|
inhibition by coumarins |
XI |
XIa |
|
Reaction susceptible to |
|
|
|
|
|
|
|
inhibition by heparin– |
|
|
|
antithrombin complex |
|
IX |
IXa |
|
|
|
VIIa |
VII |
|
VIII + Ca2+ + Pl |
Ca2+ + Pl (phospholipids) |
|
|
X |
Xa |
|
|
|
Susceptible to inhibition also |
|
|
|
by low-molecular-weight |
|
|
V + Ca2+ + Pl |
heparin and fondaparinux |
|
|
Prothrombin II |
IIa Thrombin |
|
|
|
|
Hirudin |
|
Fibrinogen I |
|
Ia Fibrin |
Luellmann, Color Atlas of Pharmacology © 2005 Thieme
All rights reserved. Usage subject to terms and conditions of license.