


98 Drugs Acting on the Sympathetic Nervous System
Types of β-Blockers
The basic structure shared by most β-sym- patholytics (p.11) is the side chain of β-sym- pathomimetics (cf. isoproterenol with the β- blockers propranolol, pindolol, atenolol). As a rule, this basic structure is linked to an aromatic nucleus by a methylene and oxygen bridge. The side chain C-atom bearing the hydroxyl group forms the chiral center. With some exceptions (e.g., timolol, penbutolol), all β-sympatholytics exist as racemates (p.62).
Compared with the dextrorotatory form, the levorotatory enantiomer possesses a greater than 100-fold higher af nity for the β-receptor, and is, therefore, practically alone in contributing to the β-blocking effect of the racemate. The side chain and substituents on the amino group critically affect affinity for β-receptors, whereas the aromatic nucleus determines whether the compound possesses intrinsic sympathomimetic activity (ISA), that is, acts as a partial agonist or partial antagonist. A partial agonism or antagonism is present when the intrinsic activity of a drug is so small that, even with full occupancy of all available receptors, the effect obtained is only a fraction of that elicited by a full agonist. In the presence of a partialagonist (e.g., pindolol), the abilityofa full agonist (e.g., isoprenaline) to elicit a maximal effect would be attenuated, because binding of the full agonist is impeded. Partialagoniststhusalsoactantagonistically, although they maintain a certain degree of receptor stimulation. It remains an open question whether ISA confers a therapeutic advantage on a β-blocker. At any rate, patients with congestive heart failure should be treated with β-blockers devoid of ISA.
As cationic amphiphilic drugs, β-blockers can exert a membrane-stabilizing effect, as evidenced by the ability of the more lipophilic congeners to inhibit Na+ channel function and impulse conduction in cardiac tissues. At the usual therapeutic dosage, the
high concentration required for these effects will not be reached.
Some β-sympatholytics possess higher affinity for cardiac β1-receptors than for β2- receptors and thus display cardioselectivity (e.g., metoprolol, acebutolol, atenolol, bisoprolol, β1 : β2 selectivity 20–50-fold). None of these blockers is suf ciently selective to permit use in patients with bronchial asthma or diabetes mellitus (p.96).
The chemical structure of β-blockers also determines their pharmacokinetic properties. Except for hydrophilic representatives (atenolol), β-sympatholytics are completely absorbed from the intestines and subsequently undergo presystemic elimination to a major extent (A).
All the above differences are of little clinical importance. The abundance of commercially available congeners would thus appear all the more curious (B). Propranolol was the first β-blocker to be introduced into therapy in 1965. Thirty years later, about 20 different congeners were marketed in different countries (analogue preparations). This questionable development is unfortunately typical of any drug group that combines therapeutic with commercial success, in addition to having a relatively fixed active structure. Variation of the molecule will create a new patentable chemical, not necessarilya drug with a novel action. Moreover, a drug no longer protected by patent is offered as a generic by different manufacturers under dozens of different proprietary names. Propranolol alone has been marketed in 2003 by 12 manufacturers in Germany under nine different names. In the USA, the drug is at present offered by ~ 40 manufacturers, mostly under its generic designation, and in Canada by six manufacturers, mostly under a hyphenated brand name containing its INN with a prefix.
Luellmann, Color Atlas of Pharmacology © 2005 Thieme
All rights reserved. Usage subject to terms and conditions of license.
Types of β-Blockers |
99 |
A. Types of β -sympatholytics |
|
|
|
|
|
|
|
|
|
|
|
|||
Isoproterenol |
|
|
Pindolol |
H |
|
Propranolol |
|
Atenolol |
O |
|
||||
OH |
|
|
|
|
|
|
|
|
|
CH2 |
C |
NH2 |
||
|
|
|
|
N |
|
|
|
|
|
|
||||
HO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
O |
|
|
|
|
O |
|
|
|
|
|
|
HC CH2 |
+ |
|
|
|
|
|
CH2 |
|
|
O |
|
|
||
NH2 |
CH2 |
|
|
|
+ |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
CH2 |
|
|
|||
OH |
HC |
CH3 |
HC |
CH2 |
+ |
|
HC |
CH2 |
NH2 |
|
+ |
|||
|
|
|
NH2 |
OH |
|
HC |
CH3 |
HC CH2 |
||||||
|
CH3 |
OH |
|
|
HC |
CH3 |
|
NH2 |
||||||
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
CH3 |
OH |
|
HC CH3 |
||||
|
|
|
|
|
|
CH3 |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
CH3 |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
β -Receptor |
|
|
β |
-Receptor |
|
|
β -Receptor |
|
|
||||
Agonist |
|
|
|
|
partial |
|
Antagonist |
Antagonist |
||||||
|
Effect |
|
|
Agonist |
|
|
|
No effect |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
||||
Sodium channel |
|
|
|
|
|
|
|
|
|
|
blockade |
|||
|
|
Na+ |
|
|
Na+ |
|
|
|
Na+ |
|
|
|
||
“membrane |
|
|
|
|
|
|
|
|
|
|
stabilizing” |
|||
β 1 |
|
β 1 |
|
|
β 1 |
|
β 1 |
|
|
β 1 |
|
|
β 2 |
|
Cardio- |
β |
2 |
|
|
β 2 |
|
β 2 |
|
|
β 2 |
selectivity |
|||
|
|
|
100% |
|
|
|
|
|
|
|
|
|
|
|
Presystemic |
|
50% |
|
|
|
|
|
|
|
|
elimination |
|||
B. Avalanche-like increase in commercially available β -sympatholytics
1965 |
1970 |
|
|
Year introduced |
Tertatolol |
Nebivolol |
|
|
|
|
|
|
|
|
Carvedilol |
|
|
|
|
|
|
|
|
Esmolol |
|
|
|
|
|
|
|
|
Bopindolol |
|
|
|
|
|
|
|
|
Bisoprolol |
|
|
|
|
|
|
|
|
Celiprolol |
|
|
|
|
|
|
|
Betaxolol |
|
|
|
|
|
|
|
|
Befunolol |
|
|
|
|
|
|
|
|
Carteolol |
|
|
|
|
|
|
|
Mepindolol |
|
|
|
|
|
|
|
|
Penbutolol |
|
|
|
|
|
|
|
|
Carazolol |
|
|
|
|
|
|
|
|
Nadolol |
|
|
|
|
|
|
|
|
Acebutolol |
|
|
|
|
|
|
|
|
Bunitrolol* |
|
|
|
|
|
|
|
|
Atenolol |
|
|
|
|
|
|
|
|
Metipranol |
|
|
|
|
|
|
|
Metoprolol |
|
|
|
|
|
|
|
|
Timolol |
|
|
|
|
|
|
|
Sotalol |
|
|
|
|
||
|
|
Talinolol |
|
|
|
|
||
|
|
Oxprenolol |
*No longer available commercially |
As of 2000 |
|
|||
|
|
Pindolol |
|
|
||||
|
|
|
|
|
|
|
|
|
|
Bupranolol* |
|
|
|
|
|
|
|
|
Alprenolol |
|
|
|
|
|
|
|
Propranolol |
1975 |
|
1980 |
1985 |
1990 |
1995 |
2000 |
|
Luellmann, Color Atlas of Pharmacology © 2005 Thieme
All rights reserved. Usage subject to terms and conditions of license.

100 Drugs Acting on the Sympathetic Nervous System
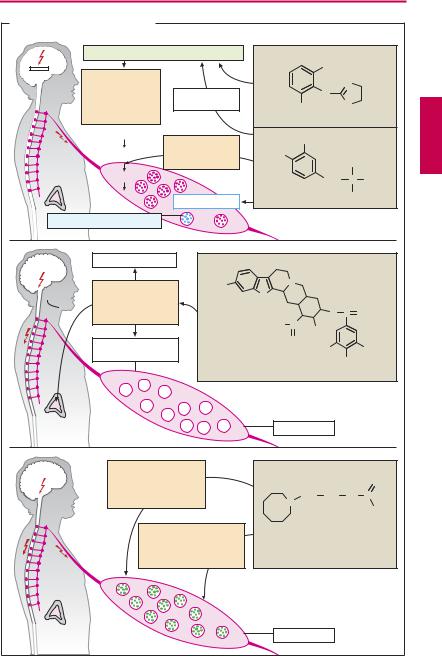
Antiadrenergics
Antiadrenergics are drugs capable of lowering transmitter output from sympathetic neurons, i.e., the “sympathetic tone.” Their action is hypotensive (indication: hypertension, p.314); however, being poorly tolerated, they enjoy only limited therapeutic use.
Clonidine is an α2-agonist whose high lipophilicity (dichlorophenyl ring) permits rapid penetration through the blood–brain barrier. The activation of postsynaptic α2-re- ceptors dampens the activity of vasomotor neurons in the medulla oblongata, resulting in a resetting of systemic arterial pressure at a lower level. In addition, activation of presynaptic α2-receptors in the periphery (pp.86, 94) leads to a decreased release of both norepinephrine (NE) and acetylcholine. Beside its main use as an antihypertensive, clonidine is also employed to manage withdrawal reactions in subjects being treated for opioid addiction.
Side effects. Lassitude, dry mouth; rebound hypertension after abrupt cessation of clonidine therapy.
Methyldopa (dopa = dihydroxyphenylal- anine), being an amino acid, is transported across the blood–brain barrier, decarboxylated in the brain to α-methyldopamine, and then hydroxylated to α-methyl-NE. The decarboxylation of methyldopa competes for a portion of the available enzymatic activity so that the rate of conversion of L-dopa to NE (via dopamine) is decreased. The false transmitter α-methyl-NE can be stored; however, unlike the endogenous mediator, it has a higher af nity for α2- than for α1-receptors and therefore produces effects similar to those of clonidine. The same events take place in peripheral adrenergic neurons.
Adverse effects. Fatigue, orthostatic hypotension, extrapyramidal Parkinson-like symptoms (p.188), cutaneous reactions, hepaticdamage,immune-hemolyticanemia.
Reserpine, an alkaloid from the climbing shrub Rauwolfia serpentina (native to the
Indian subcontinent), abolishes the vesicular storage of biogenic amines (NE, dopamine [DA], serotonin [5-HT]) by inhibiting the (nonselective) vesicular monoamine transporter located in the membrane of storage vesicles. Since the monoamines are not taken up into vesicles, they become subject to catabolism by MAO; the amount of NE released per nerve impulse is decreased. To a lesser degree, release of epinephrine from the adrenal medulla is also impaired. At higher doses, there is irreversible damage to storage vesicles (“pharmacological sympathectomy”), days to weeks being required for their re-synthesis. Reserpine readily enters the brain, where it also impairsvesicular storage of biogenic amines.
Adverse effects. Disorders of extrapyramidal motor function with development of pseudo-parkinsonism (p.188), sedation, depression, stuffy nose, impaired libido, impotence; and increased appetite.
Guanethidine possesses high af nity for the axolemmal and vesicular amine transporters. It is stored instead of NE, but is unable to mimic functions of the latter. In addition, it stabilizes the axonal membrane, thereby impeding the propagation of impulses into the sympathetic nerve terminals. Storage and release of epinephrine from the adrenal medulla are not affected, owing to the absence of a reuptake process. The drug does not cross the blood–brain barrier.
Adverse effects. Cardiovascular crises are a possible risk: emotional stress of the patient may cause sympathoadrenal activation with epinephrine release from the adrenal medulla. The resulting rise in blood pressure can be all the more marked as persistent depression of sympathetic nerve activity induces supersensitivity of effector organs to circulating catecholamines.
Luellmann, Color Atlas of Pharmacology © 2005 Thieme
All rights reserved. Usage subject to terms and conditions of license.
|
|
|
|
Antiadrenergics |
101 |
||
A. Inhibitors of sympathetic tone |
|
|
|
|
|
||
|
|
Stimulation of central α 2-receptors |
|
|
|
|
|
|
|
Suppression |
|
|
Cl |
|
|
|
|
|
|
|
N |
|
|
|
|
of sympathetic |
|
|
|
|
|
|
|
α -Methyl-NA |
|
N |
|
|
|
|
|
impulses in |
|
|
|
||
|
|
vasomotor |
in brain |
Cl |
H |
N |
|
|
|
center |
|
Clonidine |
|
H |
|
|
|
|
|
|
|
||
|
|
Tyrosine |
Inhibition |
OH |
|
|
|
|
|
|
|
|
|
||
|
|
DOPA |
of DOPA- |
HO |
|
|
|
|
|
|
decarboxylase |
|
|
CH3 |
|
|
|
Dopamine |
|
|
CH2 |
α |
NH2 |
|
|
|
|
|
C |
||
|
|
NA |
α -Methyl-NA |
α -Methyldopa |
|
COOH |
|
|
|
|
|
|
|
||
|
False transmitter |
|
|
|
|
|
|
NA |
|
CNS |
|
|
|
|
|
5HT |
|
|
|
|
|
|
|
DA |
|
|
N |
|
|
|
|
|
|
H3CO |
|
|
|
||
|
|
Inhibition of |
|
|
|
||
|
|
N |
|
|
|
||
|
|
|
|
|
|
||
|
|
biogenic amine |
|
|
|
|
|
|
|
|
H |
|
|
|
|
|
|
storage |
|
|
O |
C |
O |
|
|
|
|
H3CO C |
|
|
|
|
|
|
|
OCH3 |
|
|
|
|
|
Peripheral |
|
O |
|
|
|
|
|
|
H3CO |
|
OCH3 |
||
|
|
sympathetic activity |
|
||||
|
|
|
|
OCH3 |
|||
|
|
|
|
|
|
||
|
|
|
Reserpine |
|
|
|
|
No epinephrine from |
|
Varicosity |
|
|
|||
adrenal medulla |
|
|
|
|
|||
|
|
|
|
|
|
||
|
|
Inhibition of impulse |
|
|
|
|
|
|
|
propagation in |
|
|
|
NH |
|
|
|
peripheral sympathetic |
CH2 |
CH2 |
NH |
C |
|
|
|
nerves |
|
||||
|
|
|
|
N |
|
|
NH2 |
|
|
|
|
|
|
|
|
|
|
|
Active uptake and |
|
|
|
|
|
|
|
storage instead of |
|
|
|
|
|
|
|
norepinephrine; |
|
|
|
|
|
|
|
not a transmitter |
Guanethidine |
|
|
|
Release from adrenal medulla |
|
Varicosity |
|
|
|||
unaffected |
|
|
|
|
|||
|
|
|
|
|
|
||
Luellmann, Color Atlas of Pharmacology © 2005 Thieme
All rights reserved. Usage subject to terms and conditions of license.