

62 ANORECTAL MANOMETRY
ANGIOPLASTY. See CORONARY ANGIOPLASTY AND GUIDE-
WIRE DIAGNOSTICS.
ANORECTAL MANOMETRY
ASHOK K. TUTEJA
University of Utah
Salt Lake City, Utah
GEORGE E. WAHLEN
Veterans Affairs Medical Center
and the University of Utah
Salt Lake City, Utah
SATISH S.C. RAO
University of Iowa College of
Medicine
Iowa City, Iowa
INTRODUCTION
The most commonly performed test is the evoluation of anorectal function. These tests can provide useful information regarding the pathophysiology of disorders that affect defecation, continence, or anorectal pain. Anorectal manometry quantifies anal sphincter tone and assesses anorectal sensory response, recto anal reflexes, and rectal compliance. Sensory testing is usually performed along with anorectal manometry and is generally considered a part of the manometry.
The functional anatomy of the anorectum, the equipment, and the technique used for performing anorectal manometry and the parameters for measuring and interpreting the test are discribed in this article. The indications for anorectal manometry are shown in Table 1.
FUNCTIONAL ANATOMY AND PHYSIOLOGY OF THE ANORECTUM
The neuromuscular integrity of the rectum, anus, and the pelvic floor musculature help to maintain normal fecal continence and evacuation. The rectum is an S-shaped muscular tube, which serves as a reservoir and as a pump for emptying stool. The anus is a 2–4 cm long muscular cylinder, which at rest forms an angle with the axis of the rectum of 908. During voluntary squeeze the angle becomes more acute, 708, and during defecation, the
Table 1. Indications for Anorectal Manometry
Fecal Incontinence
Chronic idiopathic constipation
Diagnosis of Hirschsprung’s disease and/or follow up Megarectum
Pelvic floor dyssynergia Rectocele
Solitary rectal ulcer Rectal prolapse Functional anorectal pain
Neurological diagnostic investigations Biofeedback training
Preand Postsurgery (pouch)
angle becomes more obtuse, 110–1308 (1,2). The puborectalis muscle, one of the pelvic floor muscles, is responsible for these changes. The anal canal is surrounded by specialized muscles that form the anal sphincters [internal anal sphincter (IAS) and the external anal sphincter (EAS)]. The IAS is 0.5 cm thick and is an expansion of circular smooth muscle layer of the colon. It is an involuntary muscle innervated by fibers of the autonomic nervous system. The EAS is composed of striated muscle, is 0.6– 1 cm thick, and is under voluntary control (3). The anus is normally closed by the tonic activity of the IAS. This barrier is reinforced during voluntary squeeze by the EAS. The IAS contributes 70–85% of the resting anal pressure. The IAS does not completely seal the anal canal and requires the endo-anal cushions to interlock and seal the canal. The anal mucosal folds, together with the expansive anal vascular cushions, provide a tight seal. These barriers are further augmented by the puborectalis muscle, which forms a flap-like valve that creates a forward pull and reinforces the anorectal angle to prevent fecal incontinence (3,4). The rectum and the IAS are innervated by the autonomic nervous system. The EAS and the anoderm are supplied by somatic nerves. The mucosa of the rectum and proximal anal canal is lack of somatic sensory innervation. The pudendal nerve, arising from second, third, and fourth sacral nerves is the principal somatic nerve and innervates the EAS, the puborectalis muscle, and the anal mucosa (5).
EQUIPMENT FOR ANORECTAL MANOMETRY
The manometric system has two major components: the manometric probe and the pressure recording apparatus. Several types of probes and pressure recorders are available. Each system has distinct advantages and disadvantages. The most commonly used probes and recording devices are reviewed here (6).
Water-Perfused Catheter
This catheter has multiple canals through which water is perfused slowly using a pneumohydraulic pump (Arndorfer, Milwaukee, WI; MUI Scientific Ltd., Toronto, Canada). The infusion rate is 0.5 mL canal 1 min 1. In the catheter with helicoidal configuration the side holes of the canals are arranged radially and spaced 1, 2, 3, 4, 5, and 8 cm from the ‘‘0’’ reference point. A compliant balloon is tied to one end of the probe, which has a 200 mL capacity. The catheter is placed inside the anorectum, but the pressure transducers are located outside the body and across the flow of water. Resistance generated to the flow of water by luminal contractile activity is quantified as intraluminal pressure. The transducers located on the perfusion pump and the perfusion ports must be at the same level during calibration and when performing the study. The maintenance of the water perfused system requires relatively skilled personnel and air bubbles in the water tubing can affect the pressure recordings. The probe and the recording system are inexpensive and versatile. The closely spaced pressure sensors along the probe can record rectal and anal canal pressures and discriminate between EAS and IAS activity (7).

Solid-State Probe
This system has pressure sensors (microtransducers) that are mounted on the probe. This allows more accurate measurement by placing the pressure sensors directly at the source of pressure activity. The transducers are true strain gauge, that is, they consist of a pressure sensitive diaphragm with semiconductor strain gauges that are mounted on its inner surface. Currently, this is the most accurate catheter system for performing manometery (8). It is user friendly, offers higher fidelity, and is free of limitations imposed by the perfused system. However, it is expensive.
Amplifier–Recorder
The pressure signals that are obtained from the transducer are amplified and recorded on computerized small size amplifiers and recorders (e.g., Polygraph-Medronics/ Functional Diagnostics, Minneapolis, MN; Insight, Sandhill Scientific Ltd. Littleton, CO; 7-MPR, Gaeltec, Isle of Sky, UK, and others). They are small, compact, and not only serve as amplifiers and recorders, but also facilitate analysis of data and provide convenient storage for future retrieval of data or for generating a database. No one system is ideal, although each has its strengths and weakness.
STUDY PROTOCOL
General Instructions for Patients Undergoing Anorectal Manometry
In order to maximize uniformity, the manometry should be accomplished with the rectum emptied of feces. The preparation cannot be indispensable for incontinent patients. Constipated patients must be examined several hours after a 500 mL tap water enema or a single Fleets phospho-soda enema. Patients may continue with their routine medications, but the medications should be documented to facilitate interpretation of the data. Patients may eat or drink normally up to the time of the test. Upon arrival at the motility laboratory, the patient may be asked to change into a hospital gown.
The duration of the test is 1 h. The manometry catheter is inserted into the rectum while patients lie on their left side. Patients will feel movement of the catheter and distension of the balloon. After the test, patients can drive home and resume their usual work and diet. It is a safe procedure. There should be little, if any, discomfort during manometry. No anesthetic is used. Absolute contraindication to manometry is recent surgery of the rectum and anal canal, relative contraindication is a poorly compliant patient and rectum loaded with stool.
Patient Position and Digital Examination
It is recommended that the patient is placed in the left lateral position with knees and hips bent to 908. After explaining the procedure, a digital rectal examination is performed using a lubricated gloved finger. The presence of tenderness, stool, or blood on the finger glove should be noted.
ANORECTAL MANOMETRY |
63 |
Probe Placement
Next, the lubricated manometry probe is gently inserted into the rectum and oriented such that the most distal sensor (1 cmlevel) is located posteriorly at 1 cm from anal verge. The markings on the shaft of the probe should aid this orientation.
Run-in Time
After probe placement, a rest (run-in) period should be allowed ( 5 min) to give the subject time to relax and allow the sphincter tone to return to basal levels.
Resting Anal Pressure
Currently, two methods are available for assessing this function (9). Station pull-through: In this technique, the most distal sensor of a multiport catheter assembly is placed 5 cm above the anal margin. At every 30 s intervals, the catheter is withdrawn by 0.5 cm either manually or with a probe withdrawal device (10). As the sensors straddle the high pressure zone, there is a step up of pressure. The length and the highest pressure of the anal sphincter is then measured. Because pull-through excites anal contraction and the individual is conscious of these movements, the recorded pressure is high (10). For the same reason, a rapid pull through is not an accurate method and is not advisable for measuring anal sphincter function. Stationary method: Uses radially arranged multiport catheter, at least three sensors, 1 cm apart that is placed in the anal sphincter zone, that is, 0–3 cm from the anal verge (11). After allowing the tracings to stabilize, the highest sphincter pressure that is observed at any level in the anal canal is taken as the maximum resting sphincter pressure. Resting pressures can be expressed as the average obtained from each transducer or as a range to identify asymmetry of anal canal pressures (12).
Normal anal canal pressures vary according to sex, age, and techniques used (10). Normal values for anorectal manometry are shown in Table 2. There are normal variations in external sphincter pressures both radially and longitudinally (12,14). Anterior quadrant pressures are lower in the orad part of anal canal while posterior quadrant pressures are lower in the distal part of the anal canal. In the mid-anal canal, pressures are equal in all four quadrants. Manometry also enables routine calculation
Table 2. Suggested List of Tests/Maneuver Based on Indication (s)a
|
Indications for maneuver |
|
|
|
|
Test |
Incontinence |
Constipation |
|
|
|
Resting pressure |
Yes |
Yes |
Squeeze pressure/duration |
Yes |
No |
Cough reflex |
Yes |
No |
Attempted defecation |
No |
Yes |
RAIR |
No |
Yes |
Rectal sensation |
Yes |
Yes |
Rectal compliance |
Optional |
Optional |
aFrom Ref. 13 with permission.
64 ANORECTAL MANOMETRY
of anal canal length. Overall pressures are higher in men and younger persons and men have longer anal canals than women. But there is considerable overlap in values and disagreement among various studies about the effect of age and gender on anal canal pressures (10–12,15). Furthermore, subjects with values outside the normal range may not have clinical symptoms and patients with clinical symptoms may exhibit normal values (16).
Squeeze Sphincter Pressure
This pressure can be measured with either the station pull-through or the alternative technique. In the station pull-through technique; after placing the multiport assembly as describe above, at each level the subject is asked to squeeze and to maintain the squeeze for as long as possible (at least 30 s). Alternatively, with a multiport catheter is place, the subject is instructed to squeeze on three separate occasions, with a minutes’ rest between each squeeze to allow for recovery from fatigue. The average of the three highest sphincter pressures recorded at any level in the anal canal is taken as the maximum anal squeeze pressure (13). The duration of maximum sustained squeeze should also be determined and is defined as the time interval in seconds during which the subject can maintain a squeeze pressure at or above 50% of the maximum pressure.
Weak squeeze pressures may be a sign of external sphincter damage, neurological damage of the motor pathways, or a poorly compliant patient. Squeeze pressures should be evaluated together with response to cough reflex (16).
Response to Increases in Intraabdominal Pressure
An increase in intraabdominal pressure brought about by asking the subject to blow up a party balloon or by coughing is associated with a reflex increase in the activity of the EAS (11); also called the cough reflex. This reflex response causes the anal sphincter pressure to rise above that of the rectal pressure so that continence is maintained. The response may be triggered by receptors in the pelvic floor and mediated through a spinal reflex arc. In patients with complete supra conal spinal cord lesions, this reflex response is present, but the voluntary squeeze may be absent whereas in patients with lesions of the cauda equina or of the sacral plexus, both the reflex response and the voluntary squeeze are absent.
Rectoanal Pressure Changes During Attempted Defecation
In this maneuver, the subject is asked to bear down, and simulate the act of defecation. The side holes of catheter are located within the anal canal and the rectal balloon is kept inflated. The normal response consists of an increase in rectal pressure coordinated with a relaxation of the intraanal pressure. Alternatively, there may be a paradoxical increase in anal canal pressures, or absent relaxation or incomplete relaxation of the anal sphincter (Fig. 1) (17). It must be appreciated that laboratory conditions may induce artifactual changes, which is a learned response and is under voluntary control.
Anorectal |
Levator ani muscle |
|
angle |
||
|
||
|
Pubis |
Puborectalis
shelf Internal sphincter muscle
Coccyx |
External |
|
|
|
sphincter |
|
muscle |
Posterior |
Anterior |
Figure 1. Structures of the anorectum: Reprinted from Ref. 17 with permission from American Gastroenterological Association.
Rectoanal Inhibitory Reflex
This consists of reflex relaxation of the IAS in response to rectal distension. The catheter is positioned with its side holes within the anal canal. Volumes of air are rapidly inflated in the rectal balloon and removed. The inflated time is 10 mL s. The reflux is evoked with 10, 20, 40, 60, 80, 140, and 200 mL. As the volume of rectal distension is increased, the amplitude and duration of IAS relaxation increases (7). The absolute or relative amplitude of the IAS relaxation depends on the preexisting tone of the IAS and the magnitude of its contribution to the basal anal tone. This reflex may facilitate sampling of rectal contents by the sensory receptors in the upper anal canal and may also help to discriminate flatus, from liquid or solid stools. This reflex is regulated by the intrinsic myenteric plexus. In patients with Hirschsprung’s disease and in those with a history of rectal resection and coloor ileo-anal anastomosis, this reflex is absent. However, in patients with spinal cord injury and in patients with transaction of the hypogastric nerves or lesions of the sacral spinal cord, it is present (18).
Sensory Testing
Rectal Sensory Function. In this technique, the rectal sensory threshold for three common sensations (first detectable sensation, the sensation of urgency to defecate, and the sensation of pain or maximum tolerable volume) is assessed. This can be assessed either by the intermittent rectal distension or by the ramp inflation method.
Intermittent Rectal Distension. This technique is performed by inflating a balloon in the rectum using a handheld syringe. After each inflation, the balloon is deflated completely and after a rest period it is reinflated to the next volume (19).
Ramp Inflation. In this method, the rectum is progressively distended without deflation. This is performed by continuously inflating the balloon at a constant rate with a peristaltic pump or a syringe using increasing volumes of air or fluid or in a stepwise fashion, with a 1 min interval between each incremental inflation of 10–30 cm3. It is known that the type of inflation (phasic vs. continuous) and the speed of continuous inflation affect the threshold
|
100 |
|
SQUEEZE |
REST |
|
80 |
|
||
|
|
|
|
|
p1 |
60 |
|
|
|
40 |
|
|
|
|
mmHg |
|
|
|
|
|
20 |
|
|
|
|
0 |
|
|
|
|
100 |
|
|
|
|
80 |
|
|
|
p5 |
60 |
|
|
|
mmHg |
40 |
Anal 2 cm |
|
|
|
20 |
|
|
|
|
|
|
|
|
|
0 |
|
|
|
|
100 |
|
|
|
|
80 |
|
|
|
p6 |
60 |
|
|
|
|
|
|
|
|
mmHg |
40 |
Anal 1 cm |
|
|
|
20 |
|
|
|
|
|
|
|
|
|
0 |
|
|
|
|
|
13:29:30 |
13:30:00 |
13:30:30 |
volume required for healthy control subjects to perceive distension (20). Also the size and shape of the balloon will affect the threshold volume. Some of this variability can be reduced by using a high compliance balloon and a continuous-infusion pump or a barostat (21).
The maximum tolerable volume or pain threshold may be reduced in patients with a noncompliant rectum (e.g., proctitis) abdominoperineal pull-through, and rectal ischemia (9). Pain threshold also may be reduced in patients with irritable bowel syndrome (22). Higher sensory threshold is seen in autonomic neuropathy, congenital neurogenic anorectal malformations (spinal bifida, Hirschprung’s disease, meningocele) and with somatic alteration in rectal reservoir (megarectum, descending perineum syndrome) (20,23). Rectal sensory threshold is altered by change in rectal wall compliance and sensory data should be interpreted along with measurement of rectal compliance (24).
Anal Sensation. At present, assessment of anal canal sensation is not of established value for the diagnosis and treatment of patients with constipation or fecal incontinence (9).
Rectal Compliance
The capacity and distensibility of the rectum are reflected by its compliance. It is a measure of the rectal reservoir function and is defined as the change in rectal volume per unit change in rectal pressure (11). The rectal compliance can be measured by the balloon distension method or more accurately by using a computerized barostat. The higher the compliance, the lower the resistance to distension and vice versa. Low rectal compliance is also seen in patients with acute ulcerative colitis, radiation proctitis, and low spinal cord lesions (20). High compliance is seen in patients with megarectum. Decreased rectal compliance can result in decreased rectal capacity, fecal urgency, and may contribute to fecal incontinence (25).
MANOMETRIC FEATURES OF FECAL INCONTINENCE AND CONSTIPATION
Fecal Incontinence
Anorectal manometry can provide useful information regarding the pathophysiology and management of fecal
ANORECTAL MANOMETRY |
65 |
13:3 |
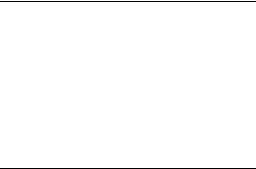
Figure 2. Normal squeeze profile. |
incontinence (26). Anal sphincter pressures may be decreased in patients with fecal incontinence; either circumferentially or in one quadrant of the anal canal (Fig. 2). Manometry can also determine if compensatory squeeze pressure can be activated. A reduced resting pressure correlate with predominant weakness of IAS and decreased squeeze pressures correlate with EAS defects (27). Two large studies have reported that maximum squeeze pressure has the greatest sensitivity and specificity in discriminating fecal incontinence from continent and healthy controls (28,29). The ability of the EAS to contract reflexly can also be assessed during abrupt increases of intraabdominal pressure (e.g., when coughing). This reflex response causes the anal sphincter pressure to rise above that of the intrarectal pressure to preserve continence. This reflex response is absent in patients with lesions of the cauda equina or the sacral plexus (18,30). On sensory testing, both hyperand hyposensitivity can be seen. Assessment of rectal sensation is useful in patients with fecal incontinence associated with neurogenic problems, such as diabetes mellitus (decrease in rectal sensations) or multiple sclerosis (increase in rectal sensation) (31). In some patients, rectal sensory thresholds may be altered because of changes in the compliance of the rectal wall. Patients with megarectum have decreased rectal sensation; and can present with fecal incontinence. Patients with incontinence often have lower rectal compliance (i.e., chronic rectal inschemia, proctitis).
Because of the wide range of normal values in anorectal physiologic testing, no single test can predict fecal incontinence. However, a combination of the tests with clinical evaluation is helpful in assessment of patients with fecal incontinence (32). Anorectal manometry is also useful in evaluating the responses to biofeedback training as well as assessing objective improvement following drug therapy or surgery.
Constipation
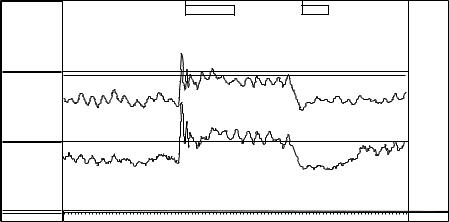
Anorectal manometry is useful in the diagnosis of dyssynergic defecation. Manometry helps to detect abnormalities during attempted defecation. Normally, when subjects bear down or attempt to defecate, there is a rise in rectal pressure, which is synchronized with a relaxation of the EAS (Fig. 3). The inability to perform this coordinated
66 ANORECTAL MANOMETRY
Figure 3. Strain maneuver: A normal coordinated response of the anorectum during attempted defecation shows a rise in rectal pressure associated with a decrease in anal sphincter pressure.
|
100 |
|
BEAR DOWN |
REST |
|
90 |
|
||
|
|
|
|
|
|
80 |
|
|
|
|
70 |
|
|
|
p1 |
60 |
Rectum |
|
|
50 |
|
|
|
|
mmHg |
|
|
|
|
40 |
|
|
|
|
|
|
|
|
|
|
30 |
|
|
|
|
20 |
|
|
|
|
10 |
|
|
|
|
0 |
|
|
|
|
100 |
|
|
|
|
90 |
Anal canal |
|
|
|
80 |
|
|
|
|
|
|
|
|
|
70 |
|
|
|
p4 |
60 |
|
|
|
50 |
|
|
|
|
mmHg |
|
|
|
|
40 |
|
|
|
|
|
|
|
|
|
|
30 |
|
|
|
|
20 |
|
|
|
|
10 |
|
|
|
|
0 |
13:49:00 |
13:49:30 |
13:50:30 |
|
|
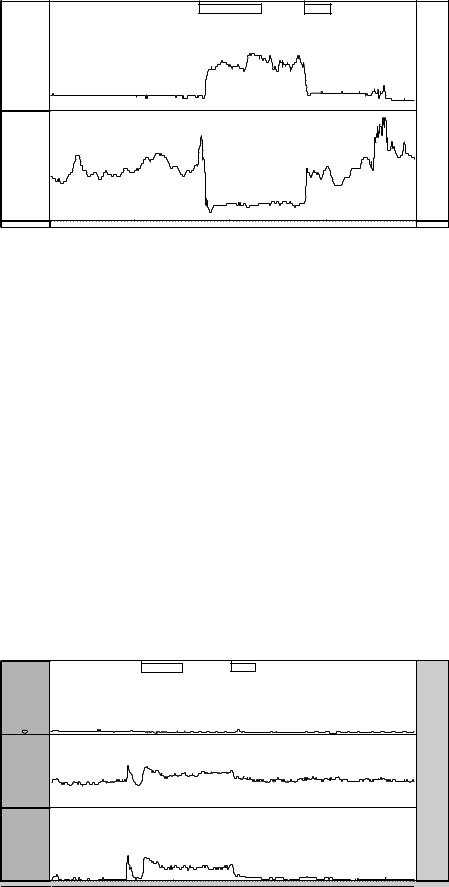
movement represents the chief pathophysiologic abnormality in patients with dyssynergic defecation (17). This inability may be due to impaired rectal contraction, paradoxical anal contraction, impaired anal relaxation, or a combination of these mechanisms (Fig. 4) (Fig. 5). Anorectal manometry also helps to exclude the possibility of Hirschsprung’s disease. The absence of the rectoanal inhibitory reflex accompanied by a normal intrarectal pressure increase during distension of the intrarectal balloon is evidence of denervation of the intrinsic plexus at the recto-anal level. Megarectum can cause a falsely negative reflex. In this condition, there is hypotonia of the rectal wall due to a deficiency of visceroelastic properties of the rectum and high degrees of rectal distension are necessary to produce the reflex. In addition to the motor abnormalities, sensory dysfunction may be present. The rectal sensations are reduced in patients with megarectum. The first sensation and the threshold for a desire to defecate may be higher in 60% of patients with dyssynergic defecation (33). The threshold for urge to defecate may be absent on elevated in patients with chronic constipation. Maximum tolerable volume can also be elevated (34). But is not clear whether these findings are the cause or secondary to constipation. When rectal sensation is impaired, neuromuscular conditioning using biofeedback technique can be effective in improving the dysfunction.
Select Appropriate Test/Maneuver
Because anorectal manometry consists of several maneuvers, it is important to determine whether a patient needs all of the maneuvers or only a selection from the array of tests described below. The patient’s symptoms and the reason for referral are helpful in choosing the appropriate list. A suggested list is given in Table 3.
Prolonged Anorectal Manometry. It is now feasible to perform anorectal manometry for prolonged periods of time outside the laboratory setting. With the use of this technique, it is possible to measure physiologic functions of the anal sphincter while the person is mobile and free (35). This technique shows promise as an investigational procedure, but its clinical applicability has not been established.
Clinical Utility and Problems with Anorectal Manometry.
A systematic and careful appraisal of anorectal function can provide valuable information that can guide treatment of patients with anorectal disorders. Prospective studies have shown that manometric tests of anorectal function provide not only an objective diagnosis, but also a better understanding of the underlying pathophysiology. In
Figure 4. Weak resting and squeeze anal sphincter pressure in a patient with fecal incontinence.
|
100 |
SQUEEZE |
REST |
|
90 |
||
|
80 |
|
|
|
70 |
|
|
p1 |
60 |
Rectum |
|
50 |
|
||
mmHg |
|
||
|
40 |
|
|
|
30 |
|
|
|
20 |
|
|
|
10 |
|
|
|
0 |
|
|
|
100 |
|
|
|
90 |
|
Anal 2 cm |
|
80 |
|
|
|
70 |
|
|
p5 |
60 |
|
|
50 |
|
|
|
mmHg |
|
|
|
40 |
|
|
|
|
|
|
|
|
30 |
|
|
|
20 |
|
|
|
10 |
|
|
|
0 |
|
|
|
100 |
|
|
|
90 |
|
|
|
80 |
|
Anal 1 cm |
|
70 |
|
|
p6 |
60 |
|
|
50 |
|
|
|
mmHg |
|
|
|
40 |
|
|
|
|
|
|
|
|
30 |
|
|
|
20 |
|
|
|
10 |
|
|
|
0 |
|
|
|
|
8:36:00 |
8:37:00 |
ANORECTAL MANOMETRY |
67 |
addition, it provides new information that could influence the management and outcome of patients with disorder of defecation (36,37).
Anorectal manometry has gained wide acceptance as a useful method to objectively assess the physiology of defecation. However, there are some problems with anorectal physiologic testing. There is a lack of uniformity with regards to the anorectal manometry equipments, methods of performance, and interpretation of the tests. A multiplicity of catheter designs exists, including water-perfused catheters, microtransducers, and microballoons. The techniques of manometric measurement are variable. The catheter can be left at one position (stationary technique), it can be manually moved from one position to another (manual pull through technique), or it can be automatically delivered from one position to another (automatic pullthrough technique). If the automated technique is selected, pressure can be recorded while the catheter is at rest or in motion. Pressure can be recorded in centimeters of H2O, millimeters of mercury (mmHg), or kilopascals (kPa). There is also a relative lack of normative data stratified for age and gender. A more uniform method of performing
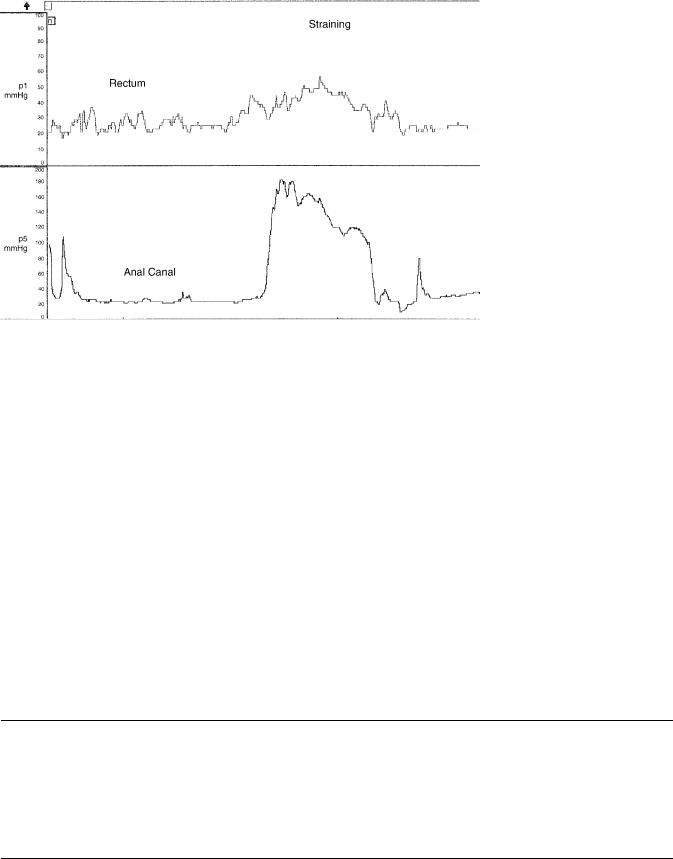
Figure 5. Dyssynergic defecation. During strain maneuver there is rise in intrarectal pressure together with a paradoxical rise in anal sphincter pressure.
these tests and interpreting the results is needed to facilitate a wider use of this technecology for the assessment of patients with anorectal disorders. Recently, experts from the American and European Motility Society have described a consensus document, where minimum standards for performing ARM have been described (13). By adopting such standards it is possible to standardize the technique globally that should help diagnosis and interpretation.
Medical Terms:
Compliance: |
It is defined as the capacity of the |
|
organ to stretch (expand) in |
|
response to an imposed force. |
Defecation: |
The discharge of feces from the |
|
rectum. |
Distal: |
Situated away from the center |
|
of the body, or from the point |
|
of origin, in contrast to prox- |
|
imal. |
Table 3. Normal Manometric Data During Anorectal Manometrya,b
|
All (n ¼ 45) |
Male (N ¼ 18) |
Female (N ¼ 22) |
||
Length of anal sphincter, cm |
3.7 (3.6–3.8) |
4.0 (3.8–4.2) |
3.6 (3.4–3.8) |
||
Maximum anal rest pressure, mmHg |
67 |
(59–74) |
71 (52–90) |
64 |
(53–75) |
Sustained squeeze pressure, mmHg |
138 (124–152) |
163 (126–200) |
117 (100–134) |
||
Squeeze duration, s |
28 |
(25–31) |
32 (26–38) |
24 |
(20–28) |
% increase in anal sphincter pressure during squeeze |
126 |
(89–163) |
158 (114–202) |
103 |
(70–136) |
Rectal pressure when squeezing, mmHg |
19 |
(14–23) |
24 (15–33) |
16 |
(11–21) |
Anal pressure during party balloon inflation, mmHg |
127 (113–141) |
154 (138–170) |
106 |
(89–123) |
|
Rectal pressure during party balloon inflation, mmHg |
63 |
(54–72) |
66 (51–81) |
62 |
(51–73) |
aMean 95% cl.
bFrom Ref. 11 with permission.
68 |
ANORECTAL MANOMETRY |
|
|
Dyssynergia: |
When an act is not performed |
|
|
smoothly or accurately because |
|
|
of lack of harmonious associa- |
|
|
tion of its various components; |
|
|
when there is lack of coordi- |
|
|
nation or dyssynergia of the |
|
|
abdominal and pelvic floor |
|
|
muscles that are involved in |
|
|
defecation it is called dyssy- |
|
|
nergic defecation |
|
ENS: |
Abbreviation for enteric nervous |
|
|
system. |
|
Endoanal Cushion: Within the anus. Anal mucosal |
|
|
|
folds together with anal vas- |
|
|
cular cushion. |
|
High pressure zone: Intense compression area. |
|
|
Intrinsic Plexus: |
A network or inter-joining of ner- |
|
|
ves and blood vessels or of lym- |
|
|
phatic vessels belonging entirely |
|
|
to a part. |
|
Myenteric Plexus: A plexus of unmyelinated fibers |
|
|
|
and postganglionic autonomic |
|
|
cell bodies lying in the muscular |
|
|
coat of the esophagus, stomach, |
|
|
and intestines; it communicates |
|
|
with the subserous and submu- |
|
|
cous plexuses, all subdivisions |
|
|
of the enteric plexus. |
|
Orad: |
In a direction toward the mouth. |
|
Phasic: |
In stages, in reference to rectal |
|
|
balloon distension for sensory |
|
|
testing. |
|
Proctalgia: |
Pain in the anus, or in the rectum. |
|
Proximal: |
Nearest the trunk or the point of |
|
|
origin, in contrast to distal. |
|
Supraconal: |
Above a condyle. |
|
Tone: |
Normal tension or resistance to |
|
|
stretch. |
BIBLIOGRAPHY
Cited References
1.Strohbehn K. Normal pelvic floor anatomy. Obstet Gynecol Clin N Am 1998;25:683–705.
2.Whitehead WE, Schuster MM. Anorectal physiology and pathophysiology. Am J Gastroenterol 1987;82:487–497.
3.Matzel KE, Schmidt RA, Tanagho EA. Neuroanatomy of the striated muscular anal continence mechanism. Implications for the use of neurostimulation. Dis Colon Rectum 1990;33: 666–673.
4.Fernandez-Fraga X, Azpiroz F, Malagelada JR. Significance of pelvic floor muscles in anal incontinence. Gastroenterology 2002;123:1441–1450.
5.Gunterberg B, Kewenter J, Petersen I, Stener B. Anorectal function after major resections of the sacrum with bilateral or unilateral sacrifice of sacral nerves. Br J Surg 1976;63: 546–554.
6.Sun WM, Rao SS. Manometric assessment of anorectal function. Gastroenterol Clin N Am 2001;30:15–32.
7.Sun WM, Read NW. Anorectal function in normal human subjects: effect of gender. Int J Colorectal Disease 1989;4: 188–196.
8.Rao SSC. Book Chapter—Colon Transit and Anorectal Manometry. In: Rao SSC, editors. Gastrointestinal Motility: Tests and Problem-Orientated Approach. New York: Kluwer Academic/Plenum Publishers; 1999. pp 71–82.
9.Diamant NE, Kamm MA, Wald A, Whitehead WE. AGA technical review on anorectal testing techniques. Gastroenterology 1999;116:735–760.
10.McHugh SM, Diamant NE. Effect of age, gender, and parity on anal canal pressures. Contribution of impaired anal sphincter function to fecal incontinence. Dig Dis Sci 1987; 32:726–736.
11.Rao SS. Manometric tests of anorectal function in healthy adults. Am J Gastroenterol 1999;94:773–783.
12.Taylor BM, Beart RW, Jr., Phillips SF. Longitudinal and radial variations of pressure in the human anal sphincter. Gastroenterology 1984;86:693–697.
13.Rao SS. Minimum standards of anorectal manometry. Neurogastroenterol Motil 2002;14:553–559.
14.McHugh SM, Diamant NE. Anal canal pressure profile: a reappraisal as determined by rapid pullthrough technique. Gut 1987;28:1234–1241.
15.Pedersen IK, Christiansen J. A study of the physiological variation in anal manometry. Br J Surg 1989;76: 69–70.
16.Azpiroz F, Enck P, Whitehead WE. Anorectal functional testing: review of collective experience. Am J Gastroenterol 2002;97:232–240.
17.Rao SS. Dyssynergic defecation. Gastroenterol Clin N Am 2001;30:97–114.
18.MacDonagh R, et al. Anorectal function in patients with complete supraconal spinal cord lesions. Gut 1992;33:1532–1538.
19.Wald A. Colonic and anorectal motility testing in clinical practice. Am J Gastroenterol 1994;89:2109–2115.
20.Sun WM, et al. Sensory and motor responses to rectal distention vary according to rate and pattern of balloon inflation. Gastroenterology 1990;99:1008–1015.
21.Whitehead WE, Delvaux M. Standardization of barostat procedures for testing smooth muscle tone and sensory thresholds in the gastrointestinal tract. The Working Team of Glaxo-Wellcome Research, UK. Dig Dis Sci 1997;42: 223–241.
22.Mertz H, et al. Altered rectal perception is a biological marker of patients with irritable bowel syndrome. Gastroenterology 1995;109:40–52.
23.Sun WM, Read NW, Miner PB. Relation between rectal sensation and anal function in normal subjects and patients with faecal incontinence. Gut 1990;31:1056–1061.
24.Rao SS, et al. Anorectal sensitivity and responses to rectal distention in patients with ulcerative colitis. Gastroenterology 1987;93:1270–1275.
25.Salvioli B, et al. Rectal compliance, capacity, and rectoanal sensation in fecal incontinence. Am J Gastroenterol 2001;96: 2158–2168.
26.Tuteja AK, Rao SS. Review article: Recent trends in diagnosis and treatment of faecal incontinence. Aliment Pharmacol Ther 2004;19:829–840.