

Renal Replacement Therapy |
45 |
|
|
Sunil Prakash and Arghya Majumdar |
|
A 50-year-old diabetic and hypertensive male patient was admitted with acute pancreatitis requiring ventilatory support. Despite aggressive volume resuscitation, he had a mean arterial pressure (MAP) of 60 mmHg on multiple vasopressors. An echo showed global hypokinesia. His intra-abdominal pressure was 20 mmHg. He was catheterized but had 100 mL of urine output in the past 12 h. Serum urea was 150 mg/dL, creatinine was 3.5 mg/dL, and potassium was 6.5 mEq/L.
Acute kidney injury is a common occurrence in the ICU and often requires renal replacement therapy (RRT). ICU physicians should be aware of the different modalities of renal replacement therapy (RRT) with their advantages and disadvantages.
Step 1: Initiate resuscitation and decide on RRT
•Along with resuscitation measures with ventilatory and hemodynamic support, early RRT should be considered in patients with acute kidney injury.
•Optimal timing of starting RRT remains controversial, and a joint decision between the nephrologist and the intensivist should be taken.
•The usual indications of commencing RRT are the following:
–Volume overload/pulmonary edema
–Refractory hyperkalemia (>6.5 mEq/L)
–Severe metabolic acidosis (pH <7.1)
–Anuria
S. Prakash, M.D., D.M. (*)
Department of Nephrology, Artemis Health Institute, Gurgaon, India e-mail: prakashsunil70@hotmail.com
A. Majumdar, M.D., M.R.C.P.
Department of Nephrology, AMRI Hospitals, Kolkata, India
R. Chawla and S. Todi (eds.), ICU Protocols: A stepwise approach, |
361 |
DOI 10.1007/978-81-322-0535-7_45, © Springer India 2012 |
|
362 |
S. Prakash and A. Majumdar |
|
|
–Uremic encephalopathy
–Uremic pericarditis
Step 2: Decide on appropriate modality of RRT (Table 45.1)
•Continuous RRT (CRRT)—this modality of RRT may be preferable in the following situations:
–Hemodynamically instability patients on multiple vasopressor therapy
–Unable to maintain MAP of more than 70 mmHg
–Need of large volume infusions (e.g., total parenteral nutrition [TPN])
–Raised intracranial pressure (ICP)
•Sustained low efficiency dialysis (SLED) may be preferable in some situations:
–If the patient is able to maintain MAP of more than 70 mmHg on low-dose vasopressors, this may be a reasonable option.
•Intermittent hemodialysis (IHD):
–If the patient is hemodynamically stable
–No significant volume overload
Table 45.1 Different modalities of RRT |
|
|
Modality |
Mechanism |
Methodology |
Hemodialysis (HD) |
Diffusion |
Here, the solute passively diffuses down its |
|
|
concentration gradient from one fluid |
|
|
compartment (either blood or dialysate) into |
|
|
the other. The dialysate is made to flow in a |
|
|
direction which is opposite to blood flow |
|
|
(countercurrent flow) through the hollow |
|
|
fiber dialyzer, to maintain a continuous |
|
|
concentration gradient between the two |
|
|
compartments and therefore maximize solute |
|
|
removal. Diffusion-based dialysis mostly |
|
|
removes small molecular weight solutes of |
|
|
less than 1 kD (kilodalton) |
Hemofiltration (HF) |
Convection |
Hydrostatic pressure gradient is used to induce |
|
|
the filtration (or convection) of plasma water |
|
|
across the membrane of the hemofilter. The |
|
|
frictional forces between water and solutes |
|
|
(called “solvent drag”) result in the convective |
|
|
transport of small and middle molecular weight |
|
|
solutes (less than 5,000 D) in the same |
|
|
direction as water |
Hemodiafiltration |
Diffusion and |
This modality offers the maximum solute |
(HDF) |
convection |
removal as it combines convection with |
|
|
diffusion for achieving this |
Ultrafiltration (SCUF) |
Hydrostatic pressure |
Slow continuous removal of fluid alone, by |
|
|
steady hydrostatic pressure |
Peritoneal dialysis |
Diffusion, convection, |
Solute removal is accomplished by diffusion, |
(PD) |
and osmosis |
and most of the ultrafiltration is by osmosis |
The extracorporeal blood purification procedures are usually performed by a veno-venous circuit, and the modalities are accordingly referred to as CVVHD, CVVH, or CVVHDF
45 Renal Replacement Therapy |
363 |
|
|
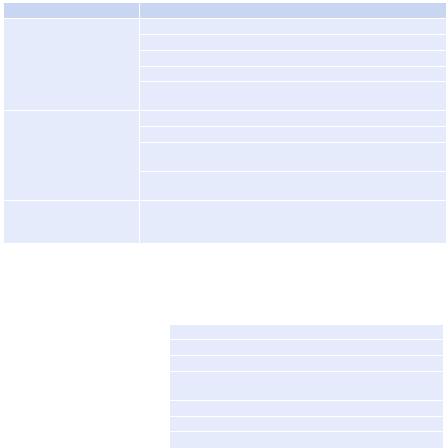
Fig. 45.1 Algorithm for choosing modalities of RRT
•Besides the medical indications, the selection of a particular modality of RRT is based on infrastructure, available resources, affordability, availability of appropriate fluids, hemofilters, and preference of the physician.
Step 3: Understand different modalities of RRT (Table 45.1)
1.CRRT (Figs. 45.1, 45.2, and 45.3 and Tables 45.2 and 45.3)
•CRRT more closely mimics normal kidney function, by gradually processing the blood and slowly removing excess fluid, uremic toxins, and electrolytes, 24 h a day and thereby improving hemodynamic stability.
•CRRT can provide up to 24–30 L of fluid exchange each day compared to 3–6 L per dialysis session for IHD. This greater fluid elimination can prevent fluid overload.
•CRRT improves the nutritional status of critically ill patients by allowing infusion of necessary volume of parenteral nutrition (2–3 L).
•It is the preferred therapy in septic shock.
•CRRT is gentler than IHD as electrolyte concentrations are slowly and continuously corrected, thereby preventing osmotic shift and variations in intracranial pressure.
•However, CRRT has failed to show unequivocal survival advantage though it may portend a better renal recovery.
•Maintain adequate anticoagulation during CRRT:
–Normally, 1,000–2,000 units of heparin are given as a bolus followed by a continuous infusion of 300–500 units per hour. Therapy is monitored every 6 h with the aim of maintaining the APTT 1.5–2 times control.
–Saline infusions sometimes suffice if the patient has already a bleeding diathesis.

364 |
S. Prakash and A. Majumdar |
|
|
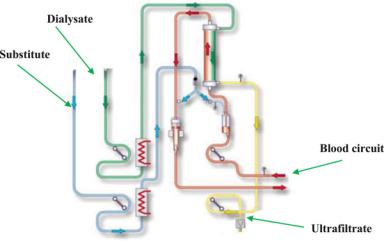
Fig. 45.2 CVVHDF
Indications of RRT
Volume |
|
|
Rising urea, |
Uremic |
|
Acidosis |
Hyperkalemia |
symptoms |
|||
creatinine |
|||||
overload |
(encephalopathy) |
||||
|
|
||||
|
|
|
Hemodynamically |
Mildhemodynamic |
Hemodynamically |
Unstable |
instability |
Stable |
CRRT |
SLED |
IHD |
|
Fig. 45.3 The dialysis circuit
45 Renal Replacement Therapy |
365 |
|
|
|
|
Table 45.2 CRRT advantages |
|
|
Advantage |
Methodology |
|
Hemodynamic stability |
Avoids hypotension, which is seen in ultrafiltration |
|
|
Avoids major swings in intravascular volume |
|
|
Allows slow and continuous tissue refilling |
|
|
Maintains steady cardiac filling pressures |
|
|
Avoids swings in intracranial pressures (beneficial in patients |
|
|
with raised ICP) |
|
Easy to replenish and |
Ultrafiltration is continuous and gentle |
|
regulate fluid volume |
Can adjust ultrafiltration rate according to hourly MAP status |
|
|
Can vary ultrafiltrate according to hourly variation in rate of |
|
|
infusates |
|
|
Can accurately adjust it to the intravascular blood volume or |
|
|
stroke volume variation when such monitors are being used |
|
Customize replacement |
According to the metabolic parameters, replacement fluid |
|
solutions |
composition may be altered like high lactate, calcium, high/low |
|
|
potassium, high/low sodium |
|
CVVHD will probably be more effective than CVVH in the highly catabolic patient with a large solute load. CVVHDF with its convective removal of larger solutes is preferred in the patient with septic shock in whom the removal of inflammatory mediators is desirable. CVVHDF combines the convective solute removal of CVVH with the diffusive solute removal of CVVHD
Table 45.3 CRRT disadvantages
Lack of rapid solute and fluid removal
Glomerular filtration rate equivalent of 15–20 mL/min
Limited role in drug overdose setting
During filter clotting, entire system shuts down and the patient loses a lot of blood
Necessitates continuous anticoagulation
Limits mobility for various investigations
Requirement of ultrapure fluids and high-flux dialyzers
–Citrate anticoagulation may be used with custom-made, calcium-free dialysate. Frequent calcium monitoring and calcium infusion may be required.
–Bivalirudin and argatroban may be considered as an anticoagulant in cases of heparin-induced thrombocytopenia requiring RRT.
–Regional anticoagulation can be achieved with heparin and protamine.
–Prostacyclin infusions are an option, but may cause hypotension.
•Continuous RRT must be provided with an effluent flow rate (the sum of hemofiltration rate and dialysate flow rate) of at least 20 mL/kg/h.
•There is improved survival at effluent flow rates of 35 mL/kg/h but not much with 45 mL/kg/h (57% and 58%, respectively) as compared to an effluent flow rate of 20 mL/kg/h (41%) in patients with septic shock.
2.SLED
•SLED is not a continuous therapy and achieves lower solute clearances that are maintained for longer period.