

Transfusion Practices and Complications |
61 |
|
|
Nayana Amin and Vijaya Patil |
|
A 54-year-old male patient with carcinoma of the rectum was admitted to the ICU with profuse bleeding per rectum for the previous 12 h. He was hypotensive and tachycardic. His hemoglobin (Hb) was 6.0 g/dL, platelet count was 150 × 103/ mm3, international normalized ratio (INR) was 1.8, and activated partial thromboplastin time (APTT) was 30 s. He was transfused with three units of packed red blood cell.
Blood transfusion is a common practice in the ICU with an estimate of 40% patients having transfusion. It is generally safe but occasionally may lead to minor or lifethreatening consequences if attention to details and protocols is not met during transfusion.
Step 1: Resuscitate
•Secure two large-bore (14G/16G) IV cannulae.
•Send blood for grouping, cross-matching, complete blood count (CBC), coagulation profile, and other appropriate investigations.
•Proper coordination with blood bank is mandatory in these situations for early and proper acquisition of blood products.
Step 2: Transfuse packed RBCs or blood components (Tables 61.1 and 61.2)
•If the patient is bleeding profusely and hemodynamically unstable, use groupspecific uncross-matched blood or O Rh-negative packed cells while waiting for cross-matched blood.
N. Amin, M.D. • V. Patil, M.D. (*)
Department of Anaesthesia, Critical Care and Pain, Tata Memorial Hospital, Mumbai, India
e-mail: vijayappatil@yahoo.com
R. Chawla and S. Todi (eds.), ICU Protocols: A stepwise approach, |
479 |
DOI 10.1007/978-81-322-0535-7_61, © Springer India 2012 |
|
480
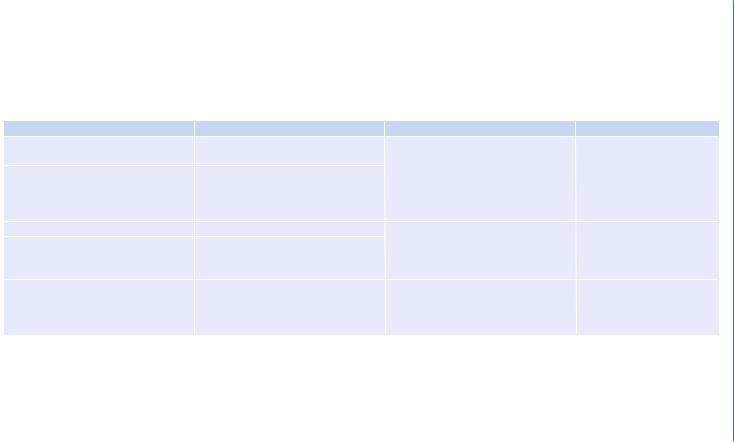
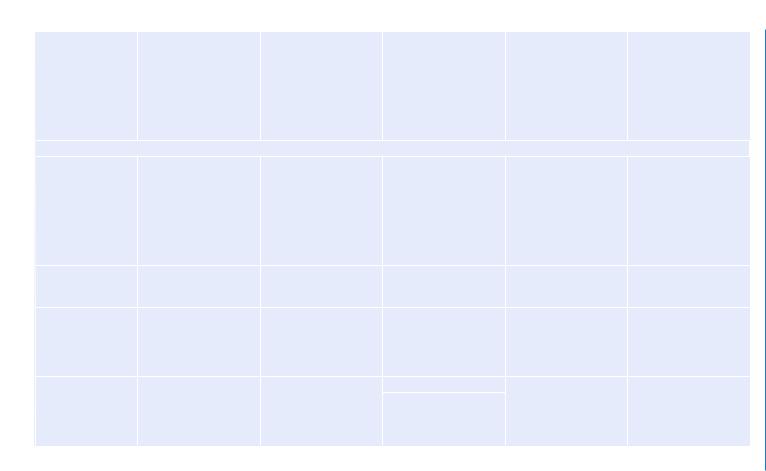
Table 61.1 Alternative red blood cell products |
|
|
|
Technique |
Purpose |
Indications |
Comments |
Leukoreduction |
Minimize the risk of cytomegalovirus |
High-risk immunocompromised |
Does not prevent TA-GVHD |
|
transmission |
patients, patients needing multiple |
(transfusion-associated graft |
Separate type of filters to allow for |
Febrile nonhemolytic transfusion |
transfusions, patients who have had |
vs. host disease) |
RBC and platelet passage only, ideally |
reactions (FNHTR) and |
FNHTR |
|
should be used during collection but |
alloimmunization |
|
|
may be used during transfusion |
|
|
|
Washed RBCs |
Prevent allergic reaction |
Recurrent severe allergic reactions in |
Not equivalent to leukoreduc- |
RBCs washed with saline to remove |
Reduce risk of hyperkalemia |
spite of premedication, IgA-deficient |
tion, 15–20% loss of RBCs |
>98% of plasma proteins, antibodies, |
|
patients, patients at risk of |
|
leukocytes, and electrolytes |
|
hyperkalemia |
|
Gamma irradiation to inactivate |
Prevents TA-GVHD |
Premature infants, patients with |
Does not reduce infectious |
leukocytes |
|
malignancy, recipients of allogenic |
risks or FNHTR |
|
|
hemopoietic transplants, transfusion to |
|
|
|
blood relatives |
|
Patil .V and Amin .N

484 |
N. Amin and V. Patil |
|
|
•In the presence of active bleeding, transfuse blood rapidly over 30 min (if available, use the rapid infusion pump, which can give fluids at a faster rate).
•4 mL/Kg of packed RBCs (usually one unit) increases the hemoglobin by 1 g/dL and hematocrit by 3% in absence of active bleeding.
•Blood should be transfused within 4 h except in emergency. Rate of transfusion can be adjusted as per need, that is, rapidly in hypovolemic patients and slowly in stable patients; however, once issued from blood bank, blood transfusion should get over within 4 h to prevent growth of organisms. If blood cannot be transfused fully within this time, it is advisable to discard it.
•Transfuse blood and blood products through the filter adequate to prevent passage of small clots that may form in stored blood.
•The filter with a pore size of 170–200 mm is recommended for routine transfusions of RBCs, platelets, fresh frozen plasma (FFP), and cryoprecipitate.
•Filters with smaller pore size are more efficient, but they would increase resistance and filter out platelet aggregates, reducing efficiency of transfused platelets.
•Microaggregate filters with 20–40 mm size are recommended during cardiopulmonary bypass only.
•Filters can slow down the rate of blood transfusion. So the standard recommendation is to use a new set for every transfusion. In case of rapid transfusion if filter does not look clogged, change the set every two transfusions.
•Use fluid warmer to transfuse blood in massive blood loss. This helps to prevent hypothermia, which can contribute to the coagulopathy by causing reversible platelet dysfunction, altering coagulation kinetics, and enhancing fibrinolysis.
•Hypothermia also causes ventricular dysrhythmias and citrate toxicity due to reduced citrate metabolism.
•Do not use unconventional and uncontrolled methods such as keeping near heat source or immersing the bag in hot water bath.
Step 3: Correct coagulopathy (see Chap. 62)
•Correct high INR with FFP or low platelets with platelet transfusions only in an actively bleeding patient.
•Do not correct raised INR prophylactically in a nonbleeding patient unless a surgical intervention is contemplated.
•Other coagulopathic abnormalities need to be corrected.
•Antifibrinolytic agents may be used to minimize bleeding in situation like trauma.
•Correct hypothermia.
•Normalize calcium.
•Consider activated factor VII in some specific situations.
Step 4: Control the source of bleeding
•Investigate to find out the source of bleeding and consider options available for controlling the bleeding (interventional radiology or surgery).
•Urgent consultation is required if needed with these specialities.
61 Transfusion Practices and Complications |
485 |
|
|
Step 5: Assess the severity of bleeding
•Massive blood loss may be defined as:
–Loss of one blood volume within a 24-h period
–Loss of blood equivalent to 7% of in lean body weight in an adult (5 L) and 8–9% in a child
–Loss of 50% of blood volume within 3 h
–Loss of blood at a rate in excess of 150 mL/min
Step 6: Manage massive blood loss
•Institute continuous invasive pressure monitoring for fluid management if the patient continues to remain hypotensive due to ongoing bleeding.
•Serial CBC (Hb and platelets) and coagulation tests (prothrombin time, APTT, and fibrinogen), blood gas analysis, serum electrolytes (Na, K, Mg, ionized calcium), and serum lactate should be done.
•These should be repeated frequently in ongoing bleeding and after every component therapy.
•Transfusion of platelets, FFPs, and cryoprecipitate should be guided by laboratory results.
•FFP administration should begin after loss of one blood volume and platelets after loss of 1.5 times the blood volume.
•1:1:2 ratio should be maintained for packed RBCs, FFP, and random donor platelets to prevent dilutional coagulopathy and dilutional thrombocytopenia due to massive blood transfusion, which results in a vicious cycle of bleeding diathesis.
•Administer cryoprecipitate if fibrinogen is less than 100 mg/dL or there is a fear of volume overload by use of FFP.
•If patients with A or B blood group have received multiple units of O Rh-positive whole blood, then they can be switched back to their inherent group-specific blood only after subsequent testing by the blood bank indicates it is safe to do so.
Step 7: Identify and manage transfusion-induced complications (Table 61.3)
•Stop blood transfusion immediately if any acute hemolytic transfusion reaction is suspected.
•Hypotension may be due to acute ongoing hemorrhage, acute severe transfusion reaction, allergic reaction/anaphylaxis, or rarely due to septic shock (due to transfusion of blood with bacterial contamination).
•Check the identity of the recipient with the details on the bag and the cross-match form.
•Transfusion-associated circulatory overload (TACO) is circulatory overload following transfusion of blood or blood product.
•Transfusion-associated acute lung injury (TRALI) is defined as new acute lung injury (with hypoxemia and bilateral infiltrates on chest radiograph but no evidence of left atrial hypertension) occurring during or within 6 h after a transfusion, with a clear temporal relationship to the transfusion, and not explained by another acute lung injury (ALI) risk factor.

