

290 |
|
|
|
|
|
|
|
|
|
|
|
|
R. Banerjee and D.N. Reddy |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Endoscopic therapy for |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
UGI bleeding |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Nonvariceal |
|
|
|
|
|
|
|
|
Variceal |
|
|
|||||
|
|
UGI bleeding |
|
|
|
|
|
|
|
|
UGI bleeding |
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Injection |
|
Mechanical |
|
Thermal |
|
|
Injection |
|
Mechanical |
|
|||||||
|
therapy |
|
therapy |
|
therapy |
|
|
therapy |
|
therapy |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sclerosant |
|
|
|
Glue |
|
|
|
|
|
Adrenalin injection |
|
|
|
|
|
esophageal varix |
|
|
fundal varix |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
1:10,000 to 1:20,000 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Endoscopic variceal
Hemostatic ligation clip
Heater |
|
Bipolar |
|
Argon plasma |
|
Coagrasper |
probe |
|
probe |
|
coagulation |
|
|
|
|
|
|
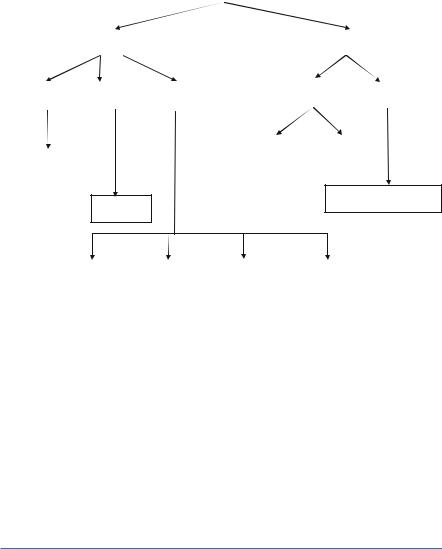
Fig. 35.1 Endoscopic therapy for UGI bleeding
B.For variceal bleeding
•Vasoactive drug treatment should be continued (terlipressin for 48 h, octreotide, or somatostatin each for 3 days).
•Antibiotic therapy should be commenced/continued.
•Balloon tamponade should be considered as a temporary salvage treatment for uncontrolled bleeding.
•Transjugular intrahepatic portosystemic stent shunting is recommended as the treatment of choice for uncontrolled variceal hemorrhage.
•An opinion of a hepatologist must be taken for further management of chronic liver disease.
Suggested Reading
1.Lim CH, Vani D, Shah SG, Everett SM, Rembacken BJ. The outcome of suspected upper gastrointestinal bleeding with 24-hour access to upper gastrointestinal endoscopy: a prospective cohort. Endoscopy. 2006;38(6):581–5.
This study shows that implementing the good practice guideline has a limited impact on overall mortality because of contributing factors that are beyond the control of clinicians.
2.Soares-Weiser K, Brezis M, Tur-Kaspa R, Leibovici L. Antibiotic prophylaxis for cirrhotic patients with gastrointestinal bleeding (Cochrane Review). In: The Cochrane Library, Issue 4, 2005. London: Wiley; 2005.
35 Upper Gastrointestinal Bleeding |
291 |
|
|
Antibiotic prophylaxis for cirrhotic inpatients with gastrointestinal bleeding is efficacious in reducing the number of deaths and bacterial infections, is well tolerated, and should be advocated.
3.Barkun A, Bardou M, Marshall JK. Consensus recommendations for managing patients with nonvariceal upper gastrointestinal bleeding. Ann Intern Med. 2003;139:843–57.
This study emphasizes the appropriate initial resuscitation of the patient and a multidisciplinary approach to clinical risk stratification that determines the need for early endoscopy. Patients with upper gastrointestinal bleeding should be tested for Helicobacter pylori infection and receive eradication therapy if infection is present.
4.Banares R, Albillos A, Rincon D, Alonso S, Gonzalez M, Ruizdel-Arbol L, et al. Endoscopic treatment versus endoscopic plus pharmacologic treatment for acute variceal bleeding: a metaanalysis. Hepatology. 2002;35(3):609.
In patients with AVB, pharmacologic agents improve the efficacy of endoscopic therapy to achieve initial control of bleeding and 5-day hemostasis, yet fail to affect mortality.
5.Blatchford O, Murray WR, Blatchford M. A risk score to predict need for treatment for uppergastrointestinal hemorrhage. Lancet. 2000;356:1318–21.
This score identifies patients who are at low or high risk needing treatment to manage their bleeding. This score should assist the clinical management of patients presenting with upper gastrointestinal hemorrhage, but requires external validation.
6.Rockall TA, Logan RF, Devlin HB, Northfield TC. Selection of patients for early discharge or outpatient care after acute upper gastrointestinal hemorrhage. Lancet. 1996;347:1138–40.
This risk score identifies a large proportion of patients with acute upper gastrointestinal hemorrhage who are at low risk of further bleeding or death. Early endoscopy and discharge of such patients could allow substantial resource savings.