Scoring Systems |
84 |
|
|
Jigeeshu V. Divatia |
|
A 60-year-old male patient with cirrhosis of the liver and portal hypertension was admitted to the hospital with pneumonia. He developed septic shock and became encephalopathic and anuric. The family wanted to know the chances of survival. Can a scoring system be used to predict the chances of survival?
The annual mortality in the ICU patients of hospital A is 5% and of hospital B is 15%. Can it be concluded that the ICU patients of hospital B are poorly managed compared to that of hospital A?
Performance measures of ICU care are usually subjective and difficult to compare. An objective measure of the structure, processes, and outcome by prognosticating in a cohort of ICU patients makes it more meaningful and easier to compare. This also helps on rational allocation of resources. A severity scoring system also helps in controlling risk factors in intervention and control groups in clinical trials.
Step 1: Understand the type of scoring systems used in ICU population
•General risk-prognostication scores (severity of illness scores)
–Acute physiology and chronic health evaluation (APACHE II, III, and IV)
–Simplified acute physiology score (SAPS II and III)
–Mortality prediction model (MPM II0 and MPM II24)
•Disease and organ-specific risk-prognostication scores
–Ranson’s score for acute pancreatitis
–RIFLE and AKIN classification for acute kidney injury
–Trauma scores
–Glasgow coma score
J.V. Divatia, M.D., F.I.S.C.C.M. (*)
Department of Anaesthesiology, Critical Care and Pain, Tata Memorial Hospital, Mumbai, India
e-mail: jdivatia@yahoo.com
R. Chawla and S. Todi (eds.), ICU Protocols: A stepwise approach, |
675 |
DOI 10.1007/978-81-322-0535-7_84, © Springer India 2012 |
|
676 |
J.V. Divatia |
|
|
–KILLIP—heart failure
–CURB—pneumonia
–CAM-ICU—delirium
•Organ dysfunction score—sequential organ failure assessment (SOFA)
•Nursing workload measurement—therapeutic intensity scoring systems (TISS)
•Population-specific—pediatrics—APGAR score
•Postoperative—PRISM
Step 2: Understand general ICU scoring systems
•All scoring systems are developed from large databases of ICU patients.
•Statistical modeling is used to determine the variables that are likely to impact survival.
•A summary score is derived from these variables, and the predicted mortality is calculated using predictive equations.
•The performance of the scoring system depends on the size and case mix of patients in the reference database and the methodology used to assign weights to different elements of the scoring system.
•APACHE II and SAPS II scoring systems were derived from datasets of patients in North American and European ICUs in the mid-1980s and early 1990s.
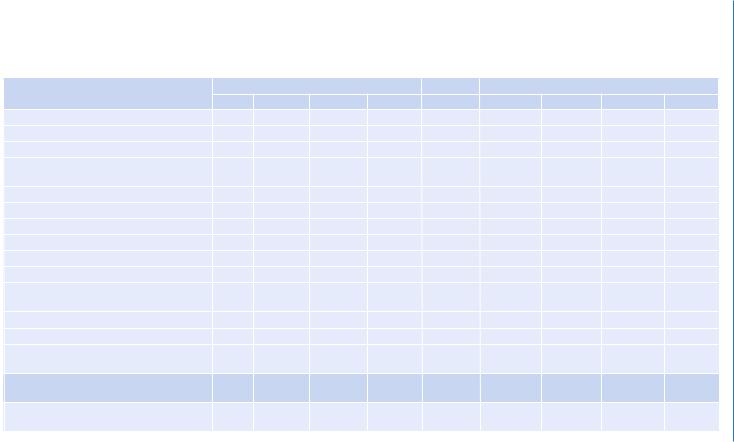
•The APACHE II scoring system assigns points to age, acute physiological observations based on the worst values in the first 24 h after admission for 12 variables, and specified preexisting chronic diseases. It also requires selection of a single diagnostic category for each patient. The predicted mortality is based on the APACHE II score and the diagnostic category (Table 84.1).
•The SAPS scoring system does not require ICU admission diagnosis for calculating the score.
•Both APACHE II and SAPS II did not account for lead-time bias (i.e., the time lag between the onset of critical illness and admission to the ICU).
•APACHE III was developed as a further refinement of APACHE II, but its mortality prediction equations are not in the public domain.
•The APACHE IV system (2006) is based on 110,558 patients in 104 North American intensive care and coronary care units between 2003 and 2004.
•SAPS III, published in 2005, was based on 16,784 patients aged 16 years or more from all continents. Three subscores—namely, patient characteristics before admission (5 variables), circumstances of admission (5 variables), and acute physiology (10 variables)—are summed up to produce the SAPS III score. A diagnostic category is essential for estimating mortality.
•Both APACHE IV and SAPS III account for lead-time bias, but have not been tested and validated as extensively as APACHE II and SAPS II.
•MPM II0, published in 1985, was the first general severity model to assess risk of death based on parameters assessed at ICU admission. Prediction models for assessment at admission and after 24 h (MPM II24) were developed originally. The models consist mainly of dichotomous variables.
678 |
J.V. Divatia |
|
|
Step 3: Understand organ failure scoring system
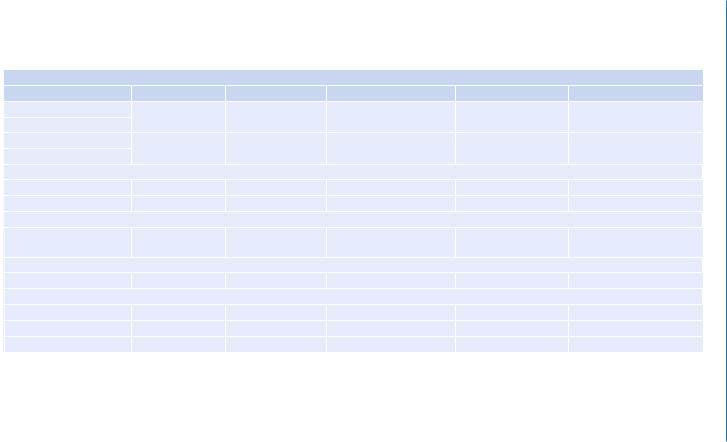
•The SOFA score is a descriptive score that uses routinely collected data for the calculation of a score of 0–4 for each organ, the higher number meaning more severe failure (Table 84.2).
•Daily scoring enables monitoring of the progress of organ dysfunction or failure.
•There are no equations to estimate mortality. However, high initial SOFA scores and worsening of SOFA scores over time correlate with increased mortality.
•The logistic organ dysfunction system (LODS) was developed for the evaluation of organ dysfunction on the first day of the ICU.
•It provides probability of hospital mortality, distinguishing it from merely descriptive models such as SOFA.
Step 4: Evaluate the scoring system
•The ability of the model to distinguish between patients who survive and patients who do not survive is termed discrimination.
•The area under the receiver operating characteristic curve (AUC) is used to give a graphical and numerical estimate of discrimination. If AUC is 0.5, it means the system is only as good as flipping a coin, and if AUC is 1, this indicates excellent discrimination.
•Calibration of a system examines the difference between the observed and expected deaths in patients grouped into different severity of illness.
•This can be evaluated graphically as well as by goodness-of-fit statistics using the Hosmer-Lemeshow test. If the p value is more than 0.05, the model provides a good fit for the data.
•The standardized mortality ratio (SMR=actual mortality/predicted mortality) also takes into account severity of illness and evaluates risk-adjusted ICU performance.
Step 5: Understand limitations of the scoring system
•None of the scoring systems are accurate enough to make predictions in individual patients and hence cannot be used to predict outcomes of individual patients.
•Most systems require data to be collected in the first 24 h after ICU admission; hence, the severity score cannot be used to decide whether to admit a patient to the ICU.
•Erroneous conclusions can be drawn if data are not collected correctly according to the original database and definitions of the scoring system.
•The score cannot be applied to patients excluded from the original database (e.g., patients younger than 16 or 18 years and patients with burns).
•Missing data and interobserver variability can affect accuracy.
•These scores may not be accurate in geographical regions, and case mix significantly different from that in the original database.
•All the scoring systems can only predict the behavior of a group of patients that matches the patients in the original database population.
•The commonly used APACHE II and SAPS II do not account for lead-time bias.