


Antibiotic Stewardship |
49 |
|
|
Subhash Todi and Rajesh Chawla |
|
A 70-year-old male patient had been admitted to the ICU with left-sided hemiparesis for 4 days. He was catheterized on admission and intubated for airway protection. He had spiked a fever of 102°F with chills and became drowsy. A broad-spectrum antibiotic was started empirically after sending blood cultures.
Judicious antibiotic prescription along with infection control is the cornerstone for preventing emergence of drug-resistant organisms in the ICU. Appropriate (right choice) and adequate (right time, right dose) antibiotic coverage improves outcome in infected patients.
Step 1: Formulate a plan for antibiotic selection
•Antibiotics in the ICU are given either empirically for presumed infection with culture report pending, or prophylactically mainly perioperative or definitively when infection is documented with positive culture results.
•Reason for antibiotic selection should be clearly documented in the antibiotic order form, which should be audited periodically for correctness.
•Appropriate antibiotics should be chosen depending on local epidemiology and resistance pattern.
S. Todi, M.D., M.R.C.P. (*)
Critical Care & Emergency, A.M.R.I. Hospital, Kolkata, West Bengal, India e-mail: drsubhashtodi@gmail.com
R. Chawla, M.D., F.C.C.M.
Department of Respiratory, Critical Care & Sleep Medicine, Indraprastha Apollo Hospitals, New Delhi, New Delhi, India
e-mail: drchawla@hotmail.com
R. Chawla and S. Todi (eds.), ICU Protocols: A stepwise approach, |
389 |
DOI 10.1007/978-81-322-0535-7_49, © Springer India 2012 |
|
390 |
S. Todi and R. Chawla |
|
|
Step 2: Send appropriate cultures
•This should ideally be done prior to starting antibiotics.
•Blood, urine, sputum, and endotracheal secretion should be promptly transported to the microbiology laboratory and expeditiously processed.
Step 3: Start antibiotics early
•Every hour delay in starting effective antibiotics from the onset of septic shock increases the risk of death from sepsis by 6–10%.
•Antibiotics should be started within 1 h of recognition of septic shock as “Time is tissue.”
Step 4: Choose empirical antibiotics appropriately
•Empirical antibiotics should be chosen carefully as initial wrong choice increases mortality, even if the antibiotic is changed appropriately after culture results are obtained.
•Initial antibiotic choice should be based on the patient’s history, underlying disease or clinical syndrome, susceptibility pattern of the pathogen in the community and hospital, and previous colonization pattern.
•Recently used antibiotic class should generally be avoided.
•Choose broad-spectrum antibiotics that have activity against most likely bacterial pathogens.
Step 5: Stratify the risk of infection with drug-resistant organisms (Table 49.1)
•The patient should be assessed for risk of infection with multidrug-resistant bacteria.
•If one or more risk factors are present, antibiotic choice should be broadened to cover these organisms.
Table 49.1 Risk factors for drug-resistant bacteria
Antimicrobial therapy in preceding 90 days
Current hospitalization of 5 days or more
High frequency of antibiotic resistance in the community or in the specific hospital unit
Immunosuppressive disease and/or therapy
Hospitalization for 2 days or more in preceding 90 days
Residence in the nursing home or extended care facility
Chronic dialysis within 30 days
Home infusion therapy (including antibiotic)
Home wound care
Having a family member with a recent history of infection with multidrug-resistant pathogens
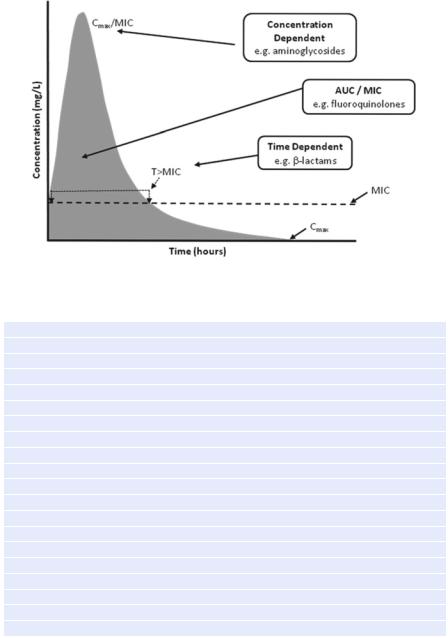
Step 6: Follow pharmacokinetic and pharmacodynamic principles while prescribing antibiotics (Fig. 49.1)
•Give adequate intravenous dose (Table 49.2).
•Give antibiotics that penetrate in adequate concentrations into the presumed source of sepsis.
49 Antibiotic Stewardship |
391 |
|
|
Fig. 49.1 Pharmacokinetic and pharmacodynamic principles
Table 49.2 Appropriate doses of common antibiotics (Refer to Appendix 1)
Antipseudomonal cephalosporin
Cefepime, 1–2 g every 8–12 h
Ceftazidime, 2 g every 8 h
Carbapenems
Imipenem, 500 mg every 6 h or 1 g every 8 h
Meropenem, 1 g every 8 h
Doripenem, 500 mg every 8 h
Ertapenem, 1 g once daily
b-Lactam/b-lactamase inhibitor
Piperacillin–tazobactam, 4.5 g every 6 h
Aminoglycosides
Gentamicin, 7 mg/kg/day
Tobramycin, 7 mg/kg/day
Amikacin, 20 mg/kg/day
Antipseudomonal quinolones
Levofloxacin, 750 mg/day
Ciprofloxacin, 400 mg every 8 h
Vancomycin, 15 mg/kg every 12 h
Linezolid, 600 mg every 12 h
Colistin: 1–2 million units every 8 h
Dosages are based on normal renal and hepatic function
Peak drug levels for gentamicin and tobramycin should be 8–10 mcg/mL and trough levels less than 2 mcg/mL
Peak drug levels for amikacin should be 25–30 mcg/mL and trough levels should be less than 4–8 mcg/mL
Trough levels for vancomycin should be 15–20 mcg/mL
392 |
S. Todi and R. Chawla |
|
|
•Time-dependent antibiotics like b-lactams (maximum bacterial inhibition depends on time above minimum inhibitory concentration) should be given as a continuous infusion.
•Dose-dependent antibiotics like aminoglycoside (maximum bacterial inhibition depends on peak antibiotic concentration) should be given as a once-daily bolus dose.
•Adjust the dose of antibiotics depending on renal and hepatic dysfunction.
Step 7: Assess the patient daily and de-escalate antibiotics once culture results are obtained
•Clinical response should be assessed frequently, and if the patient is responding favorably, antibiotics should be de-escalated to a narrower spectrum, and unnecessary antibiotics should be stopped if culture results permit.
•Decisions to continue, narrow, or stop antimicrobial therapy must be made on the basis of clinician judgment and laboratory information like decrease in leukocytosis, decreasing C reactive protein, and a low procalcitonin level.
Step 8: Consider the combination of antibiotics in specific situations
•The combination of antibiotics (two appropriate antibiotics against the same organism) is indicated in difficult to treat multidrug-resistant pathogens like Acinetobacter and Pseudomonas sp. Combination therapy is also indicated for neutropenic patient with severe sepsis and selected patients with severe Pseudomonas infection with respiratory failure and shock. Similarly, a combination of beta-lactam and macrolide is recommended for pneumococcal bacteremia.
Step 9: Decide on duration of antibiotic therapy
•Duration of therapy should typically be 7–10 days.
•Longer courses may be appropriate in patients who have a slow clinical response, undrainable foci of infection, or immunologic deficiencies including neutropenia.
•If culture result is negative and there is a favorable clinical response, most antibiotics can be stopped in 5 days.
•In Pseudomonas and Acinetobacter infection, severe sepsis should be treated for 2 weeks.
Step 10: Implement antibiotic stewardship program
•Constitute an antibiotic stewardship team along with the microbiologist, infection control nurse, infectious disease consultant, and clinical pharmacist.
•Educating ICU staff the principles of antibiotic stewardship is of prime importance.
•Proper utilization of local antibiogram should be done.
•Utilize optimally the information obtained from the microbiology laboratory.
•Work in close collaboration with microbiologists and other physicians involved in antibiotic prescribing.