


72 Heat Stroke and Hypothermia |
577 |
|
|
•Hypotension: To sustain organ perfusion, maintain mean arterial pressure of more than 65 mmHg by fluid administration, consider vasopressors, and monitor central venous pressure.
•Seizures should be controlled by IV benzodiazepines and barbiturates.
•Multiorgan failure: Give supportive therapy until organ function recovers. Stepwise management of hyperthermia is shown in Fig. 72.1.
Step 7: Prevention
•Hyperthermia, caused by physical exertion or hot environment, can be prevented by taking frequent rest breaks and staying hydrated.
•Genetic testing for known mutations of the SKM ryanodine receptor in conjunction with in vitro muscle contracture test can be used to evaluate individual susceptibility in patients from families with a history of malignant hyperthermia.
72.2Hypothermia
An 82-year-old man, a known case of Alzheimer’s disease and hypothyroidism, was found unresponsive on his backyard lawns. He had been taking aspirin, olanzapine, and levothyroxine for the past 3 years. Examination revealed femoral pulse 35/min, blood pressure (BP) unrecordable, Glasgow Coma Scale 3, and temperature 28°C.
Step 1: Initiate resuscitation
Initiate resuscitation as mentioned in Chap. 78:
•The management should start with removal of wet clothing if any and replacing it with warm, dry sheet.
•In severe hypothermia, if indicated, the patient is intubated gently and ventilated with warmed humidified O2 while closely monitoring cardiac rhythm.
•One should be prepared to treat ventricular fibrillation with DC shock (200 J) and cardiopulmonary resuscitation.
•Start IV line and infuse normal saline at 43°C.
Step 2: Diagnose types and severity of hypothermia
Primary
•Normal thermoregulation
•Overwhelming cold exposure
578 |
J. Dureja and H. Singh |
|
|
Table 72.1 Severity of hypothermia |
|
Mild (34–36°C) |
Shivering, amnesia/dysarthria, loss of coordination, tachycardia, |
|
tachypnea, normal BP |
Moderate (30–34°C) |
Absent shivering, bradycardia/atrial fibrillation, ↓ BP, ↓ respiratory |
|
rate, and stupor |
Severe (<30°C) |
Coma, absent corneal and oculocephalic reflexes, ↓↓ BP, ventricular |
|
fibrillation, apnea, areflexia, dilated and fixed pupils, flat EEG, |
|
asystole |
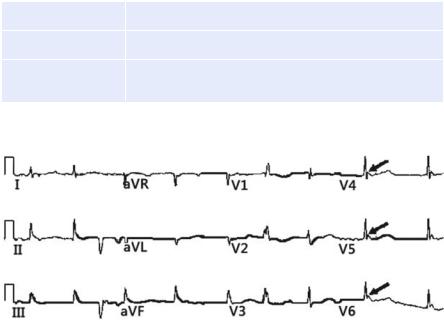
Fig. 72.2 Osborn (J) waves (Marked with arrows)
Secondary
•Abnormal thermogenesis
•Multiple causes (hypothyroidism, burns, hypothalamic abnormalities, sepsis) Hypothermia is defined as temperature less than 36°C.
Severity of hypothermia with presentation is described in Table 72.1.
•ECG may show Osborn (J) waves especially when temperature is less than 33°C (Fig. 72.2).
•It is a positive deflection, and its amplitude is proportional to the degree of hypothermia, usually seen in leads V3–V6 at junction of QRS and ST segment.
Step 3: Manage hypothermia
The patient should be warmed by the following rewarming methods: passive, active external, and active internal.
•Passive rewarming: It allows endogenous heat production to increase the core temperature, but heat conserving mechanisms must be intact (e.g., shivering, metabolic rate, and sympathetic nervous system).
580 |
J. Dureja and H. Singh |
|
|
•Remove wet cloths (to prevent conductive and convective heat loss)
•Maintain horizontal position
•Protect against heat loss and wind chill (use blanket and insulating material)
•Avoid rough movement, shaking and excessive activity (to prevent arrhythmias) Monitor core temperature and cardiac activity
Assess responsiveness breathing and pulse
|
|
|
Pulse and breathing present |
|
|
Pulse or breathing absent |
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
• |
Start CPR |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
• |
Give one shock |
|
||||||
|
|
Measure core temperature |
|
|
|
|
|
|
• |
Secure the airway |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
• Ventilate with warm humid O2 |
|
|||||||
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
34–36°C (93.2–96.8°F) |
|
|
|
|
|
• |
(42–46°C) |
|
|||||||||
|
|
|
|
|
|
|
Establish IV access |
|
|||||||||||
|
|
Mild hypothermia |
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
• Infuse warm NS 43°C (109°F) |
|
|||||||||||
|
|
Do passive rewarming and |
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
active external rewarming |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Measure core temperature |
|
|||||
30–34°C (86–93.2° F) |
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||
Moderate hypothermia |
|
|
|
|
|
|
|
|
|
|
|
||||||||
Do passive rewarming and active |
|
|
|
|
|
|
|
|
|
|
|
||||||||
external rewarming of truncal areas only |
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
<30°C |
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
<30°C (86.0° F) |
|
|
|
|
|
|
|
|
|
|
|
||||||||
Severe hypothermia |
|
|
|
|
|
|
|
|
|
|
|
||||||||
• |
Active internal warming |
|
|
|
|
|
|
|
|
|
|
|
|||||||
• Infuse warm IV fluids at 43°C |
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
Continue CPR |
|
|
|
||||||||||||
|
|
(109°F) |
|
|
|
|
Withhold IV drugs |
|
|||||||||||
• Warm humid O2 at 42–46°C (108– |
|
|
|
|
1 shock for VF/VT |
|
|||||||||||||
|
|
115°F) |
|
|
|
|
Active internal warming |
|
|||||||||||
• Peritoneal lavage with KCl-free |
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||
• |
|
fluid |
|
|
|
|
|
|
|
|
|
|
|
||||||
Extracorporeal rewarming |
|
|
|
|
|
|
|
|
|
>30°C |
|||||||||
• |
Esophageal rewarming tubes |
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
Step4 |
|
|
|
|
Continue CPR |
||||||||||
|
|
|
|
Continue internal rewarming until |
|
Give IV medications as indicated but |
|||||||||||||
|
|
|
|
Core temperature >35°C (95°F) OR |
|
space at long interval than standard |
|||||||||||||
|
|
|
|
Return of spontaneous circulation OR |
|
Repeat shock for VF/VT as the core |
|||||||||||||
|
|
|
|
Resuscitative efforts cease |
|
|
|
|
temperature rises |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Rewarm as moderate hypothermia |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fig. 72.3 Stepwise management of hypothermia