

|
Osteoporosis |
331 |
A. Bone: normal state and osteoporosis |
|
|
Normal state |
Osteoporosis |
|
Organic bone matrix |
Bone mineral: hydroxyapatite |
|
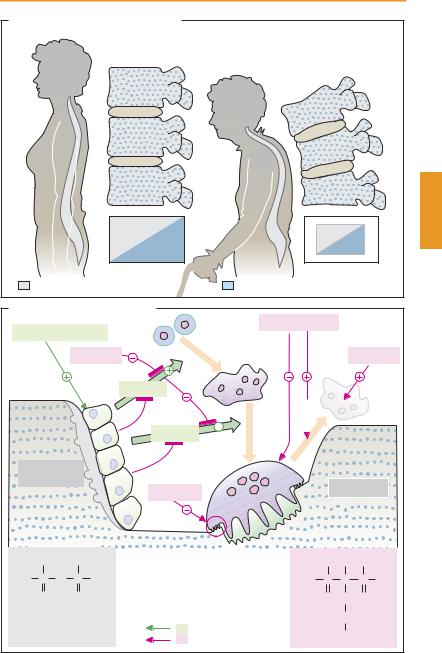
B. Regulation of bone remodeling |
|
|
|
|
|
|||||
|
|
|
|
|
Progenitor |
Biphosphonates |
|
|
|
|
Parathyroid hormone |
cells |
|
|
|
|
|
||||
|
|
|
Estrogens |
Fusion |
|
|
|
Estrogens |
||
|
|
|
|
|
|
|
||||
|
|
|
|
|
RANKL |
|
|
|
Apoptosis |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
OPG |
|
|
|
|
|
|
|
|
|
|
RANKL |
|
|
|
|
|
|
|
|
|
|
Activation |
|
|
|
|
|
(Pre)Osteo- |
|
|
OPG |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|||
blasts |
|
|
|
|
|
|
Osteoclasts |
|||
|
|
|
|
|
Calcitonin |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
OH |
|
OH |
|
RANK = receptor activating NF-Κ |
-B |
OH OH OH |
|
||
|
|
|
|
|
|
|
|
|
||
HO |
P |
O |
P |
OH |
RANKL = RANK-Ligand |
HO |
P |
C |
P |
OH |
|
O |
|
O |
|
OPG = Osteoprotegerin |
|
O |
CH2 O |
|
|
Pyrophosphate |
|
Bone resorption |
|
|
(CH2)2 |
|
||||
|
Stimulation |
Alendronate |
|
|
||||||
|
|
|
|
|
Inhibition |
|
|
NH2 |
|
|
|
|
|
|
Rheumatoid Arthritis |
|
|
333 |
|||
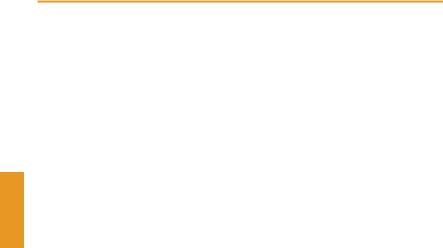
A. Rheumatoid Arthritis |
|
|
|
|
|
|
|
|||
|
Genetic predisposition |
|
|
|
|
|
|
|
||
|
|
|
Environmental factors |
|
|
|
|
|
|
|
|
|
|
Precipitating |
Infection |
|
|
|
|
|
|
|
|
|
causes |
Trauma |
|
|
|
|
|
|
|
|
|
Immune system: reactive against autologous joint tissue |
|
|
|
|
|
||
Sulfasalazine |
|
? |
Prostaglandin |
|
|
|
|
|
||
|
synthesis |
|
|
|
|
|
|
|||
|
|
|
|
|
|
COX inhibitors |
||||
IL-1 receptor |
|
|
Cox-2 |
|
|
|
|
|
|
|
Anakinra |
|
|
Cytokines, etc. |
|
|
NH2 |
|
|
|
|
|
|
|
|
|
N |
CH2 N |
CH3 |
|||
|
|
|
IL-1, TNFα |
|
N |
|
||||
N |
Cl |
|
Infliximab |
H2N |
N |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
Methotrexate |
|
|
||||
|
|
|
|
|
|
|
||||
NH |
|
|
|
Etanercept |
|
|
H |
C |
|
|
|
|
C2H5 |
|
|
|
N |
O |
|||
H3C CH CH2 CH2 CH2 N |
|
HOOC |
(CH2)2 |
CH |
COOH |
|||||
Chloroquine |
|
|
C2H5 |
|
ÐMethotrexate |
|||||
|
|
|
|
|
||||||
Gold, |
|
? |
Macrophages |
Lymphocytes |
(purine |
|
|
|
||
|
synthesis |
) |
|
|||||||
chloroquine |
|
|||||||||
|
|
|
ÐLeflunomide |
|
||||||
|
|
|
|
|
|
|||||
|
|
|
|
|
|
(pyrimidine |
|
|||
|
|
|
|
|
|
synthesis |
) |
|
||
|
|
|
|
|
ÐCiclosporin |
|
||||
|
|
|
Antigen (unknown) |
|
|
(IL-2 synthesis |
||||
|
|
|
|
|
|
in T-helper cells ) |
||||
D-Penicillamine |
|
? |
|
|
|
|
|
|
|
|
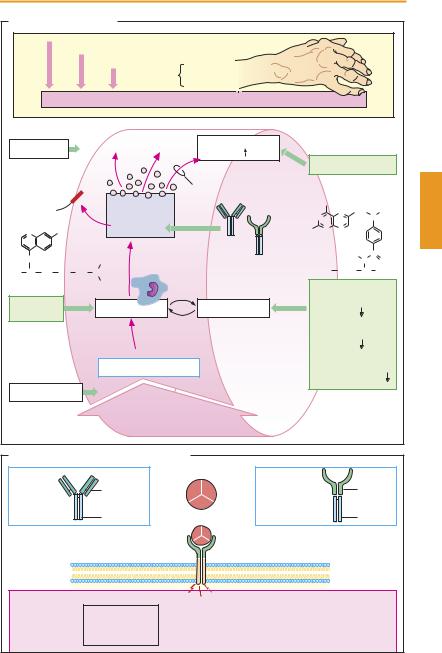
B. Tumor necrosis factor α and inhibitors |
|
|
|
|
|
|
||||
|
|
|
Homotrimer |
|
|
|
|
TNF α |
|
|
|
|
|
Murine |
|
|
|
|
|
|
|
Infliximab |
|
|
portion (Fab) |
TNF α |
Etanercept |
|
|
|
receptor- |
|
|
|
|
|
|
|
parts |
||||
(chimeric |
|
|
Human |
|
(fusion protein) |
|
|
|
||
|
|
|
|
|
|
|
|
|||
IgG antibody) |
|
|
|
|
|
|
|
|
||
|
portion (Fc) |
|
|
|
|
|
Fc portion |
|||
|
|
|
|
|
|
|
|
|||
|
|
|
|
TNF α |
|
|
|
|
|
|
|
|
|
|
receptor |
|
|
|
|
|
|
|
|
|
Activation |
|
|
|
|
|
|
|
|
|
Vessels: |
|
|
|
|
|
|
Tumor cells |
|
Ð Proliferation |
|
Macrophages: |
|
Synovial membrane: |
|
Bone: |
|
|
Ð Activation |
|
Ð Proliferation |
|
|||
Ð Lysis |
|
Ð Adhesion of |
|
|
|
Ð Resorption |
||
|
|
Ð Chemotaxis |
|
Ð Pannus formation |
|
|||
|
|
blood cells |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|