


106 Drugs Acting on the Parasympathetic Nervous System
Parasympathomimetics
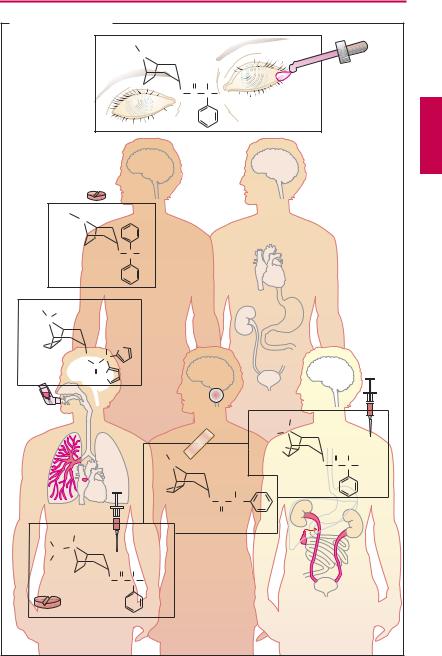
Acetylcholine (ACh) is too rapidly hydrolyzed and inactivated by acetylcholinesterase (AChE) to be of any therapeutic use; however, its action can be replicated by other substances, namely, direct or indirect parasympathomimetics.
Direct parasympathomimetics. The choline ester of carbamic acid, carbachol, activates M-cholinoceptors, but is not hydrolyzed by AChE. Carbachol can thus be effectively employed for local application to the eye (glaucoma) and systemic administration (bowel atonia, bladder atonia). The alkaloids pilocarpine (from Pilocarpus jaborandi) and arecoline (from Areca catechu; betel nut) also act as direct parasympathomimetics. As tertiary amines, they moreover exert central effects. The central effect of muscarine-like substances consists in an enlivening, mild stimulation that is probably the effect desired in betel chewing, a widespread habit in South Asia. Of this group, only pilocarpine enjoys therapeutic use, which is almost exclusively by local application to the eye in glaucoma (p.346).
Indirect parasympathomimetics inhibit local AChE and raise the concentration of ACh at receptors of cholinergic synapses. This action is evident at all synapses where ACh is the mediator. Chemically, these agents include esters of carbamic acid (carbamates such as physostigmine, neostigmine) and of phosphoric acid (organophosphates such as paraoxon = E600, and nitrostigmine = parathion = E605, its prodrug).
Members of both groups react like ACh with AChE. The esters are hydrolyzed upon formation of a complex with the enzyme. The rate-limiting step in ACh hydrolysis is deacetylation of the enzyme, which takes only milliseconds, thus permitting a high turnover rate and activity of AChE. Decarbaminoylation following hydrolysis of a carbamate takes hours to days, the enzyme re-
maining inhibited as long as it is carbaminoylated. Cleavage of the phosphate residue, i.e., dephosphorylation, is practically impossible; enzyme inhibition is irreversible.
Uses. The quaternary carbamate neostigmine is employed as an indirect parasympathomimetic in postoperative atonia of the bowel or bladder. Applied topically to the eye, neostigmine is used in the treatment of glaucoma. Furthermore, it is needed to overcome the relative ACh-deficiency at the motor end plate in myasthenia gravis or to reverse the neuromuscular blockade (p.184) caused by nondepolarizing muscle relaxants (decurarization before discontinuation of anaesthesia). Pyridostigmine has a similar use. The tertiary carbamate physostigmine can be used as an antidote in poisoning with parasympatholytic drugs, because it has access to AChE in the brain. Carbamates and organophosphates also serve as insecticides. Although they possess high acute toxicity in humans, they are more rapidly degraded than is DDT following their release into the environment.
In the early stages of Alzheimer disease, administration of centrally acting AChE inhibitors can bring about transient improvement in cognitive function or slow down deterioration in some patients. Suitable drugs include rivastigmine, donezepil, and galantamine, which require slowly increasing dosage. Peripheral side effects (inhibition of ACh breakdown) limit therapy. Donezepil and galantamine are not esters of carbamic acid and act by a different molecular action. Galantamine is also thought to promote the action of ACh at nicotinic cholinoceptors by an allosteric mechanism.

|
|
|
|
|
|
|
Parasympathomimetics |
|
107 |
||||
A. Direct and indirect parasympathomimetics |
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
O |
|
|
|
O |
|
|
|
|
CH3 |
|
|
|
H CO |
C |
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
H N |
C |
O |
CH |
CH |
+N |
CH |
|
|
|
|
|
|
|
2 |
|
|
2 |
2 |
|
|
3 |
|
|
|
|
N |
CH3 |
Carbachol |
|
|
|
CH3 |
|
|
Arecoline |
|
|||||
|
|
|
Direct parasympatho- |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
mimetics |
|
Arecoline= |
|
|
|
|
|
O |
|
|
|
|
CH3 |
|
|
|
|
|
||
|
|
|
|
|
|
|
ingredient of |
|
|
||||
H3C C O CH2 |
CH2 |
+ |
N CH3 |
|
betel nut: |
|
|
|
|||||
|
|
betel |
|
|
|
||||||||
Acetylcholine |
|
|
CH3 |
|
|
|
|
|
|||||
|
|
|
|
chewing |
|
|
|
||||||
|
|
|
|
|
|
|
AChE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
H3C |
|
|
|
|
|
|
|
|
|
|
|
ACh |
|
N |
CH CH3 |
|
|
||
|
|
|
|
|
|
|
organ |
|
|
|
|||
|
|
|
|
|
|
|
H3C |
|
|
CH3 |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Effector |
|
|
O |
C |
N |
|
|
|
|
|
|
|
|
Rivastigmine |
O |
CH2 |
CH3 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CH3 |
|
|
H |
|
|
|
|
|
|
|
|
|
|
O |
C |
N |
|
|
|
|
|
|
|
|
|
N |
|
||||
|
|
|
|
|
|
|
|
|
|
O |
CH3 |
||
|
|
|
|
|
|
|
H3C |
|
N |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
H3C |
Physostigmine |
|
||
|
|
|
|
|
|
|
AChE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
H3C |
O |
|
H3C |
|
|
Inhibitors of |
|
OC2H5 |
|
|
|
||
|
CH3 |
acetylcholinesterase |
|
|
|
|
|
|
|||||
|
|
|
|
+ |
O |
P |
O |
|
NO2 |
|
|||
N |
C |
O |
|
N |
|
|
(AChE) |
|
|
||||
H C |
|
|
|
|
CH |
Indirect |
|
OC2H5 |
|
|
|
||
3 |
Neostigmine |
|
|
3 |
|
|
Paraoxon (E 600) |
|
|||||
|
|
|
|
parasympathomimetics |
|
|
|
||||||
Acetylcholine |
|
|
|
|
|
Nitrostigmine = |
|
|
|||||
|
|
|
|
Acetyl |
Parathion = |
|
|
|
|||||
|
|
+ |
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
E 605 |
|
|
|
|
||
|
AChE |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
ms |
|
|
|
|
|
|
|
|
Choline |
|
|
|
Deacetylation |
|
|
|
|
|
|
|
Neostigmine |
|
|
|
|
Carbaminoyl |
|
|
|
|
|
|
||
|
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AChE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hours |
|
|
|
|
|
|
|
|
|
|
|
|
|
Decarbaminoylation |
|
|
|
|
|
|
Paraoxon |
|
|
|
|
Phosphoryl |
|
|
|
|
|
|
||
|
|
+ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AChE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Dephosphorylation impossible |
|
|
|
|||

108 Drugs Acting on the Parasympathetic Nervous System
Parasympatholytics
Excitation of the parasympathetic division causes release of acetylcholine at neuroeffector junctions in different target organs. The major effects are summarized in (A) (blue arrows). Some of these effects have therapeutic applications, as indicated by the clinical uses of parasympathomimetics (p.106).
Substances acting antagonistically at the M-cholinoceptor are designated parasympatholytics (prototype: the alkaloid atropine; actions marked red in the panels). Therapeutic use of these agents is complicated by their low organ selectivity. Possibilities for a targeted action include:
Local application
Selection of drugs with favorable membrane penetrability
Administration of drugs possessing receptor subtype selectivity.
Parasympatholytics are employed for the following purposes:
1. Inhibition of glandular secretion.
Bronchial secretion. Premedication with atropine before inhalation anesthesia prevents a possible hypersecretion of bronchial mucus, which cannot be expectorated by coughing during anesthesia.
Gastric secretion. Atropine displays about equally high af nity for all muscarinic cholinoceptor subtypes and thus lacks organ specificity. Pirenzepine has preferential af nity for the M1 subtype and was used to inhibit production of HCl in the gastric mucosa, because vagally mediated stimulation of acid production involves M1 receptors. This approach has proved inadequate because the required dosage of pirenzepine produced too many atropine-like side effects. Also, more effective pharmacological means are available to lower HCl production in a graded fashion (H2-antihistaminics, proton pump inhibitors).
2.Relaxation of smooth musculature. As a rule, administration of a parasympatholytic agent by inhalation is quite effective in chronic obstructive pulmonary disease. Ipratropium has a relatively short lasting effect; four aerosol puffs usually being required per day. The newly introduced substance tiotropium needs to be applied only once daily because of its “adhesiveness.”Tiotropium is effective in chronic obstructive lung disease; however, it is not indicated in the treatment of bronchial asthma.
Spasmolysis by N-butylscopolamine in biliary or renal colic (p.130). Because of its quaternarynitrogenatom,thisdrug doesnot enter the brain and requires parenteral administration. Its spasmolytic action is especially marked because of additional ganglionic blocking and direct muscle-relaxant actions.
Lowering of pupillary sphincter tonus and pupillary dilation by local administration of homatropine or tropicamide (mydriatics) allows observation of the ocular fundus. For diagnostic uses, only short-term pupillary dilation is needed. The effect of both agents subsides quickly in comparison with that of atropine (duration of several days).
3.Cardioacceleration. Ipratropium is used in bradycardia and AV-block, respectively, to raise heart rate and to facilitate cardiac impulse conduction. As a quaternary substance, it does not penetrate into the brain, which greatly reduces the risk of CNS disturbances (see below). However, it is also poorly absorbed from the gut (absorption rate < 30%). To achieve adequate levels in the blood, it must be given in significantly higher dosage than needed parenterally.
Atropine may be given to prevent cardiac arrest resulting from vagal reflex activation, incidental to anaesthetic induction, gastric lavage, or endoscopic procedures.
|
|
|
|
Parasympatholytics |
109 |
|
A. Effects of parasympathetic stimulation and blockade |
|
|
|
|||
|
|
Deadly |
|
|
|
|
|
|
nightshade |
|
|
|
|
N. oculo- |
|
Atropa |
|
|
|
|
|
belladonna |
|
|
|
|
|
motorius |
|
|
|
|
|
|
N. facialis |
|
H3C |
|
|
|
|
N. glosso- |
|
|
|
|
|
|
|
N |
|
|
|
|
|
pharyngeus |
|
|
|
|
|
|
N. vagus |
|
|
|
|
|
|
|
|
|
|
|
CH2OH |
|
|
|
Atropine |
O |
C |
CH |
|
|
|
|
|
|
|
|
|
|
Acetylcholine |
|
O |
|
|
|
|
|
|
|
|
|
Nn. sacrales |
|
|
Muscarinic acetylcholine receptor |
|
||
|
|
|
|
|||
SchlemmÕs |
|
|
|
|
|
|
canal wide |
+ |
|
|
|
|
|
Ciliary muscle |
|
|
+ |
|
|
|
contracted |
|
|
|
Salivary secretion |
|
|
+ |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
+ |
Gastric |
|
Pupil narrow |
|
|
|
|
|
|
|
|
|
|
acid |
|
|
Pupil wide |
|
|
|
+ |
|
|
|
|
|
|
Pancreatic juice |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
production |
|
Photophobia |
|
|
|
+ |
Bowel peristalsis |
|
|
|
|
|
|
||
Near vision impossible |
|
|
+ |
|
|
|
Drainage of aqueous |
|
|
|
Bladder tone |
|
|
|
|
|
|
|
||
humor impaired |
|
|
|
|
|
|
|
|
|
|
|
|
|
Rate |
- |
|
|
|
|
|
|
|
|
|
Restlessness |
|
|
AV conduction |
|
|
|
|
|
|
|
|
|
|
Irritability |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hallucinations |
|
|
|
+ |
|
|
Antiparkinsonian |
|
Rate |
|
|
|
effect |
|
|
|
|
|
|
|
||
AV conduction |
|
|
|
|
Antiemetic effect |
|
Increased blood flow |
|
|
|
|
Dry mouth |
|
for increasing |
|
Bronchial secretion |
|
|
|
|
|
|
|
|
|
||
heat dissipation |
|
Bronchoconstriction |
|
|
Acid production |
|
|
|
|
|
|
decreased |
|
Evaporative heat |
|
|
|
|
Pancreatic |
|
loss |
|
|
|
|
secretory activity |
|
|
|
|
|
|
decreased |
|
ÒFlushed |
|
|
|
|
Bowel peristalsis |
|
|
|
|
|
decreased |
|
|
dry skinÒ |
|
Bronchial secretion |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
Bladder tone |
|
|
|
|
decreased |
|
|
|
|
|
|
Bronchodilation |
|
|
decreased |
|
+ |
Sympathetic |
|
|
|
|
|
|
|
nerves |
|
|
|
|
Sweat production |
|
|
|
|
|
|

110 Drugs Acting on the Parasympathetic Nervous System
4. CNS damping effects. Scopolamine is effective in the prophylaxis of kinetosis (motion sickness, sea sickness, see p.342); it is mostly applied by a transdermal patch. Scopolamine (pKa = 7.2) penetrates the blood– brain barrier faster than does atropine (pKa = 9), because at physiological pH a larger proportion is present in the neutral, membranepermeant form.
In psychotic excitement (agitation), sedation can be achieved with scopolamine. Unlike atropine, scopolamine exerts a calming and amnesiogenic action that can also be used to advantage in anesthetic premedication.
Symptomatic treatment in parkinsonism for the purpose of restoring a dopaminer- gic-cholinergic balance in the corpus striatum. Antiparkinsonian agents, such as benztropine (p.188) readily penetrate the blood–brain barrier. At centrally equieffective dosages, their peripheral effects are less marked than those of atropine.
Contraindications for parasympatholytics.
Closed angle glaucoma. Since drainage of aqueous humor is impeded during relaxation of the pupillary sphincter, intraocular pressure rises.
Prostatic hyperplasia with impaired micturition: loss of parasympathetic control of the detrusor muscle exacerbates dif culties in voiding urine.
Atropine poisoning. Parasympatholytics have a wide therapeutic margin. Rarely lifethreatening, poisoning with atropine is characterized by the following peripheral and central effects.
Peripheral. Tachycardia; dry mouth; hyperthermia secondary to the inhibition of sweating. Although sweat glands are innervated by sympathetic fibers, these are cholinergic in nature. When sweat secretion is inhibited, the body loses the ability to dissipate metabolic heat by evaporation of sweat. There is a compensatory vasodilation in the skin, allowing increased heat ex-
change through increased cutaneous blood flow. Decreased peristaltic activity of the intestines leads to constipation.
Central. Motor restlessness, progressing to maniacal agitation, psychic disturbances, disorientation and hallucinations. It may be noted that scopolamine-containing herbal preparations (especially from Datura stramonium) served as hallucinogenic intoxicants in the Middle Ages. Accounts of witches’ rides to satanic gatherings and similar excesses are likely the products of CNS poisoning. Recently, Western youths have been reported to make “recreational” use of Angel’s Trumpet flowers (several Brugmansia species grown as ornamental shrubs). Plants of this genus are a source of scopolamine used by South American natives since pre-Columbian times.
Elderly subjects have an enhanced sensitivity, particularly toward the CNS toxic manifestations. In this context, the diversity of drugs producing atropine-like side effects should be borne in mind: e.g., tricyclic antidepressants, neuroleptics, antihistaminics, antiarrhythmics, antiparkinsonian agents.
Apart from symptomatic, general measures (gastric lavage, cooling with ice water), therapy of severe atropine intoxication includes the administration of the indirect parasympathomimetic physostigmine (p.106). The most common instances of “atropine”-intoxication are observed after ingestion of the berrylike fruits of belladonna (in children). A similar picture may be seen after intentional overdosage with tricyclic antidepressants in attempted suicide.
|
|
|
|
|
|
|
|
|
Parasympatholytics |
|
111 |
||||
A. Parasympatholytics |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
H3C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
O |
H |
|
|
|
|
|
|
|
|
|
|
|
|
|
O |
C |
C |
OH |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Homatropine |
|
|
|
|||
|
|
|
|
|
|
|
|
|
M1 |
M1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M3 |
M1 M1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M3 |
|
|
|
|
|
|
|
H3C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
O |
C |
H |
|
|
|
|
|
|
|
|
|
|
|
Benzatropine |
|
|
|
|
|
|
M2 |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
H3C |
CH3 |
|
|
|
|
|
|
|
|
M1 |
M1 |
|
|
|
|
Tiotropium |
|
|
|
|
|
M |
|
|
|
|
|||||
+ |
|
|
|
|
|
|
|
|
|
||||||
N |
|
|
|
|
|
|
|
|
M1 |
|
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
M1 |
|
|
|
|
O |
|
HO |
S |
|
|
|
|
|
|
|
M1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
O |
C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
O S |
|
|
|
|
|
|
M |
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CH3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
+N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
H9C4 |
|
|
|
|
|
|
|
|
|
|
|
H3C |
|
“Patch” |
O |
|
|
O |
H |
|
||
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
N |
|
|
|
|
|
|
O |
C |
C |
CH2OH |
|
|
|
|
|
|
|
|
|
|
N-Butyl- |
|
|
|
||
|
|
|
|
|
O |
|
|
|
CH2OH |
scopolamine |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Scopolamine |
O |
C |
CH |
|
|
|
|
|
|
|
|
|
|
|
|
0.2–2 mg |
|
|
O |
|
|
|
|
|
|
|
H3C |
CH3 |
|
ED |
|
|
|
|
|
|
|
|
|
|
|
|
+N |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
0.5–1 mg |
|
|
|
|
|
|
|
|
|
|
|||
|
CH |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
H3C |
|
|
O |
H |
|
|
|
|
|
|
|
|
|
|
|
|
|
O C C CH2OH |
|
|
|
|
|
|
|
|
|
|
|||
|
Ipratropium |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
ED 10 mg |
|
|
|
|
|
|
|
|
+ ganglioplegic |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
+ direct muscle relaxant |
||||