

Antianginal Drugs |
319 |
A. Effects of nitrates
p |
Diastole |
Systole |
p |
|
Vol |
|
Vol |
|
|
|
Resistance |
Venous |
|
|
vessels |
|
|
|
|
capacitance |
Preload |
Nitrate |
Afterload |
vessels |
|
|
|
|
|
tolerance |
O2-demand |
|
|
|
|
|
O2-supply |
|
|
|
|
Vasorelaxation |
Relaxation of |
|
|
coronary spasm |
|
|
|
|
Nitrates, e.g., nitroglycerin (GTN), isosorbide dinitrate (ISDN)
B. Effects of Ca-antagonists |
C. Effects of β -blockers |
|
p |
|
Rest |
Ca- |
|
|
|
|
|
|
antagonists |
|
|
|
Sympathetic |
|
Relaxation |
system |
|
|
|
|
of |
|
|
resistance |
|
|
vessels |
β -Blocker |
|
|
|
Afterload |
|
Rate |
|
|
|
|
|
Contraction |
|
|
velocity |
|
Relaxation of |
|
O2-demand |
coronary spasm |
Exercise |
|
||
D. Clinical uses of antianginal drugs |
|
|
|
Angina pectoris |
|
Coronary sclerosis |
|
|
|
|
Coronary spasm |
||
|
|
|
|
|
|
|
|
Therapy of attack |
|
|
|
|
|
||
|
GTN, |
ISDN |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
Nifedipine |
|
|
|
|
|
|
|
|
|
|
|
Anginal prophylaxis |
|
|
|||||
Long-acting nitrates |
|
||||||
|
|
|
|
|
|
||
|
β− Blockers |
|
|
Ca-antagonists |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
Myocardial Infarction |
321 |
||
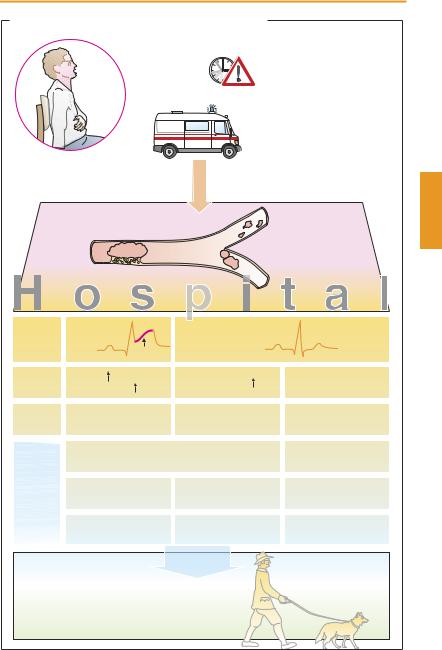
A. Myocardial infarction: pharmacotherapeutic approaches |
|
|
|||||
|
|
Acute symptoms: |
Acute care measures |
|
|||
|
|
severe pain |
|
– Nitroglycerin (reduction of |
|
||
|
|
sense of impending |
preand afterload) |
|
|||
|
|
doom |
|
– Acetylsalicylic acid |
|
||
|
Patient |
fear of dying |
|
(if needed i.v.) |
|
||
|
|
|
|
|
(inhibition of platelet |
|
|
|
|
|
|
|
aggregation) |
|
|
|
|
|
|
|
– Morphine (analgesia, sedation) |
||
|
|
|
|
|
– Oxygen via nasal tube |
|
|
|
|
|
|
|
Hospitalization |
|
|
|
|
|
|
|
with minimal delay |
|
|
Acute coronary syndrome |
Plaque rupture |
|
|
|
|||
Angina pectoris > 20 min |
|
|
|
||||
|
|
Distal |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
thrombus |
|
|
|
Thrombus |
|
|
|
|
|
|
ECG |
ST-elevation |
T |
No ST-elevation |
|
|
||
|
|
S |
|
|
|
|
|
Laboratory |
CK-MB |
|
|
Troponin-I, -T |
|
– |
|
|
Troponin-I, -T |
|
|
|
|||
|
|
|
|
|
|
||
Diagnosis |
Myocardial infarction |
Myocardial infarction |
Unstable |
|
|||
|
(“STEMI”) |
|
|
(“NSTEMI”) |
|
angina pectoris |
|
Therapy |
General: O2, acetylsalicylic acid, |
|
Acetylsalicylic acid, |
|
|||
|
heparin, nitrates, β -blocker, morphine |
|
clopidrogel |
|
|||
|
PTCA (Stent) |
|
PTCA (Stent) |
|
Cardiac |
|
|
|
GPIIb/IIIa-Antagonist |
GPIIb/IIIa-Antagonist |
catheterization |
|
|||
|
or |
|
|
|
|
|
|
|
fibrinolysis |
|
|
|
|
|
|
|
or |
|
|
|
|
|
|
|
bypass surgery |
|
|
|
|
|
|
Secondary prevention |
|
|
Discharge |
|
|
|
|
|
|
possibly: |
|
|
|
|
|
– Acetylsalicylic acid |
– Clopidrogel |
|
|
|
|
||
– β -Blocker |
– Phenprocoumon |
|
|
|
|||
– ACE inhibitor |
– Statins |
|
|
|
|
||