


148 Antithrombotics
Heparin (A)
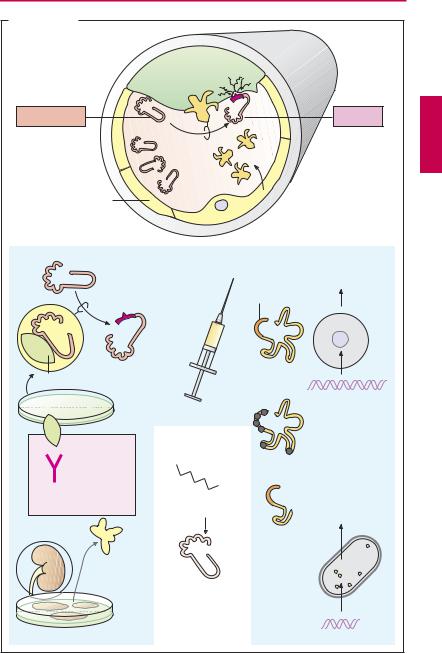
Occurrence and structure. Heparin can be obtained from porcine gut, where it is present (together with histamine) in storage vesicles of mast cells. Heparin molecules are chains of amino sugars bearing –COO– and –SO3– groups. Chain length is not constant and anticoagulant ef cacy varies with chain length. The potency of a preparation is standardized in international units of activity (IU) by bioassay and comparison with a reference preparation. The molecular weight (MW)for unfractionatedheparinrangesfrom 4000 to 40 000, with a peak around 15 000. Low-molecular-weight fractionated heparin can be produced by cleavage of native heparin; molecular size is less heterogeneous, with a mean MW of 5000 (e.g., certoparin, dalteparin, enoxaparin).The synthetic fondaparinux (MW 1728) resembles the basic pentasaccharide subunit of heparin, essential for activity. The numerous negative charges are significant in several respects: (1) they contribute to complex formation with antithrombin III that underlies the anticoagulant effect; (2) they permit binding of heparin to its antidote, protamine (a polycationic protein from salmon sperm); (3) they confer poor membrane penetrability, necessitating administration of heparin by injection.
Mechanism of action. Antithrombin III (AT III) is a circulating glycoprotein capable of inhibiting activated clotting factors by occupation andirreversibleblockade ofthe active center. Heparin acts to inhibit clotting by accelerating formation of this complex more than 1000-fold. Activated clotting factors have differing requirements for optimal chain length of heparin. For instance, to inactivate thrombin, the heparin molecule must simultaneously contact the factor and AT III. With factor Xa, however, contact between heparin and AT III is suf cient for speeding up inactivation.
Indications. Heparin is used for the prophylaxis and therapy of thrombosis. For the former, low dosages, given subcutaneously, are suf cient. Unfractionated heparin must be injected about three time daily, fractionated heparins and fondaparinux can be administered once daily. For treatment of thrombosis, heparin must be infused intravenously in an increased daily dose.
Adverse effects. When bleeding is induced by heparin, the heparin action can be instantly reversed by protamine. Against fractionated heparins and fondaparinux, protamine is less or not effective. Heparin-in- duced thrombocytopenia type II (HIT II) is a dangerous complication. It results from formation of antibodies that precipitate with bound heparin on platelets. The platelets aggregate and give rise to vascular occlusions. Because of the thrombocytopenia, hemorrhages may occur. Fondaparinux is also contraindicated in HIT II.
The drug danaparoid consists mostly of the heparinoid heparan sulfate. Its chains are composed of a part of the heparin molecule (indicated by blue color underlay). Its effect is mediated by AT III.
Hirudin and Derivatives (B)
The polypeptide hirudin from the saliva of the European medicinal leech inhibits clotting of the leech’s blood meal by blockade of the active center of thrombin. This action is independent of AT III and thus also occurs in patients with AT III deficiency. Lepirudin and desrudin are yeast-derivedrecombinant analogues. They can be used in patients with HIT II.
Ximelagatran is a modified thrombin antagonist suitable for oral use.
Heparin 149
A. Heparins: origin, structure, and mechanism of action
CH2 OSO3– |
COO– |
CH2 OSO3– |
|
|
CH2 OSO3– |
||||
O |
|
|
O |
O |
|
COO |
–O |
O |
|
OH |
|
OH |
O |
– |
|
O |
OH |
|
|
O |
OSO3 |
O |
OH |
O |
|||||
O |
|
|
|
|
|
|
|||
HN |
C |
CH3 |
OH |
HN |
SO3– |
|
OSO3– |
HN |
SO3– |
|
O |
|
|
|
|
|
|
|
|
Mast cell |
Pentasaccharide basic unit |
Antidote protamine
Activated clotting factor
Inactivation
Antithrombin III
Standard heparin |
Low-MW heparin |
unfractionated |
fractionated |
mean |
mean MW ~5000 |
MW ~15 000 |
|
~3x daily s.c. |
~once daily s.c. |
|
Acceleration |
|
of inactivation |
IIa |
Xa |
Thrombin |
|
Standard heparin |
Low-MW heparin |
required |
sufficient |
Heparin-induced thrombocytopenia type II |
|
|
Platelet |
Antibody |
aggregation |
Heparin |
|
|
Thrombo- |
Platelet |
embolism |
|
|
B. Hirudin and derivatives |
|
|
|
Leucine |
Isoleucine: |
Lepirudin |
|
H2N |
|
IIa |
Direct |
|
Thrombin |
||
|
|
selective |
|
|
|
|
inhibition |
Hirudin |
|
|
|
Hirudo medicinalis |
|
|
|

150 Antithrombotics
Fibrinolytics
The fibrin meshwork of a blood clot can be cleaved by plasmin. As a protease, plasmin can break down not only fibrin but also fibrinogen and other proteins. Plasmin derives from an inactive precursor, plasminogen, present in blood. Under physiological conditions, specificity of action for fibrin is achieved because, among other things, activation takes place on the fibrin clot.
The tissue plasminogen activator (t-PA) is released into the blood from endothelial cells when blood flow stagnates. Next to its catalytic center, this protease possesses other functional domains, including docking sites for fibrin. During contact with fibrin, plasminogen–plasmin conversion rate is several-fold higher than in streaming blood. Plasminogen also contains a binding domain for fibrin.
Plasminogen activators available for therapeutic use are designated as fibrinolytics; they are infused intravenously in myocardial infarction, stroke, deep leg vein thrombosis, pulmonary embolism, and other thrombotic vascular occlusions. The earlier treatment is started after thrombus formation, the better is the chance of achieving patency of the occluded vessel.
The desired effect carries with it the risk of bleeding as the most important adverse effect, because, apart from the intravascular fibrin clot forming the thrombus, other fibrin coagula sealing defects in the vascular wall are dissolved as well. Moreover, use of fibrinolytics entails the risk that fibrinogen and other clotting factors circulating in blood will undergo cleavage (“systemic lytic state”).
Streptokinase is the oldest available fibrinolytic. By itself it lacks enzymatic activity; only after binding to a plasminogen molecule is a complex formed that activates plasminogen. Streptokinase is produced by streptococcal bacteria. Streptokinase antibodies may be present as a result of previous streptococcal infections and may lead to incompatibility reactions.
Urokinase is an endogenous plasminogen activator that occurs in different organs. Urokinase used therapeutically is obtained from human cultured kidney cells. Circulating antibodies are not expected. The substance is more expensive than streptokinase and also does not depend on fibrin in its action.
Alteplase is a recombinant tissue plasminogen activator (rt-PA). As a result of its production in eukaryotic Chinese hamster ovary (CHO) cells, carbohydrate residues are present as in the native substance. At the therapeutically used dosage, alteplase loses its “fibrin dependence” and thus also activates circulating plasminogen. In fresh myocardial infarctions, alteplase appears to produce better results than does streptokinase.
Tenecteplase is a variant of alteplase that has been altered by six point mutations, resulting in a significant prolongation of its plasma half-life (tenecteplase t½ = 20 minutes; alteplase t½ = 3–4 minutes). Tenecteplase is dosed according to body weight and given by intravenous bolus injection.
Reteplase is a deletion variant of t-PA that lacks both fibrin-binding domains and oligosaccharide side chains (manufactured in prokaryotic E. coli). It is eliminated more slowly than alteplase. Whereas alteplase is given by infusion, reteplase can be administered in two bolus injections spaced 30 minutes apart
Plasmin inhibitors. ε-Aminocaproic acid as well as tranexamic acid and p-aminomethyl- benzoic acid (PAMBA) are plasmin inhibitors that can be useful in bleeding complications. They exert an inhibitory effect by occupying the fibrin binding site of plasminogen or plasmin.
Fibrinolytics 151
A. Fibrinolytics
Plasminogen
Endothelium
Streptokinase
Streptococci
Antibodies from prior infections
Fevers, chills, inactivation
Urokinase
Human kidney cell culture
Fibrin
|
|
|
|
oly |
si |
|
|
|
n |
||
|
|
i |
|
s |
|
|
|
r |
|
|
|
F |
i |
b |
|
|
|
|
|
|
|
|
|
t-PA
Plasmin
t-PA: tissue plasminogen activator
Plasminogen activators
Alteplase = recombinant t-PA
Active center
CHO cells
cDNA
Plasmin inhibitor
H2N
COOH
ε -Aminocaproic acid
Blockade of plasminogen/plasmin binding site on fibrin
Tenecteplase = t-PA with 6 amino acid mutations
Reteplase = nonglycosylated variant of t-PA
E. coli
Truncated cDNA