


92 Drugs Acting on the Sympathetic Nervous System
Indirect Sympathomimetics
Raising the concentration of norepinephrine in the synaptic space intensifies the stimulation of adrenoceptors. In principle, this can be achieved by:
Promoting the neuronal release of norepinephrine
Inhibiting processes operating to lower its intrasynaptic concentration, in particular neuronal reuptake with subsequent vesicular storage or breakdown by monoamine
oxidase (MAO)
Chemically altered derivatives differ from norepinephrine with regard to the relative af nity for these systems and affect these functions differentially.
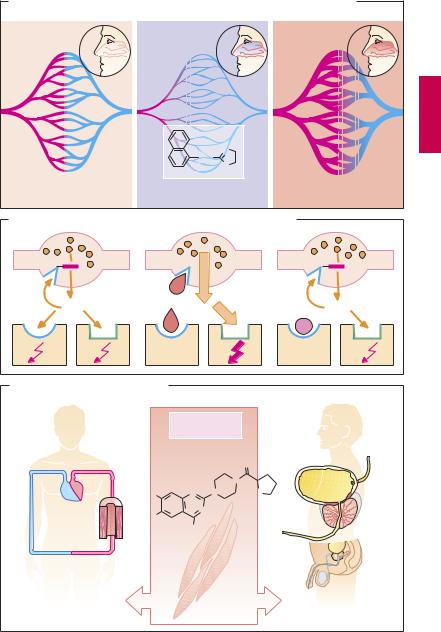
Inhibitors of MAO (A) block enzyme located in mitochondria, which serves to scavenge axoplasmic free norepinephrine (NE). Inhibition of the enzyme causes free NE concentrations to rise. Likewise, dopamine catabolism is impaired, making more of it available for NE synthesis. In the CNS, inhibition of MAO affects neuronal storage not only of NE but also of dopamine and serotonin. The functional sequelae of these changes include a general increase in psychomotor drive (thymeretic effect) and mood elevation (A). Moclobemide reversibly inhibits MAOA and is used as an antidepressant. The MAOB inhibitor selegiline (deprenyl) retards the catabolism of dopamine, an effect used in the treatment of Parkinsonism (p.188).
Indirect sympathomimetics (B) in the narrow sense comprise amphetamine-like substances and cocaine. Cocaine blocks the norepinephrine transporter (NAT), besides acting as a local anesthetic. Amphetamine is taken up into varicosities via NAT, and from there into storage vesicles (via the vesicular monoamine transporter), where it displaces NE into the cytosol. In addition, amphetamine blocks MAO, allowing cytosolic NE concentration to rise unimpeded. This induces the plasmalemmal NAT to transport
NE in the opposite direction, that is, to liberate it into the extracellular space. Thus, amphetamine promotes a nonexocytotic release of NE. The effectiveness of such indirect sympathomimetics diminishes quickly or disappears (tachyphylaxis) with repeated administration.
Indirect sympathomimetics can penetrate the blood–brain barrier and evoke such CNS effects as a feeling of well-being, enhanced physical activity and mood (euphoria), and decreased sense of hunger or fatigue. Subsequently, the user may feel tired and depressed. These after-effects are partly responsible for the urge to readminister the drug (high abuse potential). To prevent their misuse, these substances are subject to governmental regulations (e.g., Food and Drugs Act, Canada; Controlled Drugs Act, USA) restricting their prescription and distribution.
When amphetamine-like substances are misused to enhance athletic performance (“doping”), there is a risk of dangerous physical overexertion. Because of the absence ofa sense of fatigue, a drugged athlete may be able to mobilize ultimate energy reserves. In extreme situations, cardiovascular failure may result (B).
Closely related chemically to amphetamine are the so-called appetite suppressants or anorexiants (p.329). These may also cause dependence and their therapeutic value and safety are questionable. Some of these (D-norpseudoephedrine, amfepramone) have been withdrawn.
Sibutramine inhibits neuronal reuptake of NE and serotonin (similarly to antidepressants, p.226). It diminishes appetite and is classified as an antiobesity agent (p.328).

|
Indirect Sympathomimetics |
93 |
||
A. Monoamine oxidase inhibitor |
|
|
|
|
|
Inhibitor: |
Moclobemide |
MAO-A |
|
|
|
Selegiline |
MAO-B |
|
Nor- |
MAO |
|
MAO |
|
epinephrine |
|
|
||
|
|
|
|
|
|
Norepinephrine |
|
|
|
|
transport system |
|
|
|
|
Effector organ |
|
|
|
B. Indirect sympathomimetics with central stimulant activity
B. and abuse potential
|
§ |
§ |
H2C CH NH2 |
Controlled |
|
Substances |
|
|
CH3 |
Act regulates |
|
use of |
|
|
Amphetamine |
|
|
cocaine and |
|
|
|
amphetamine |
|
Pain stimulus |
Local |
|
|
anesthetic |
|
|
effect |
|
H3C |
O |
|
N |
C O |
CH3 |
|
O |
C |
Cocaine |
|
O |
|
|
|
MAO |
MAO |
“Doping”
Runner-up

94 Drugs Acting on the Sympathetic Nervous System
α-Sympathomimetics, α-Sympatholytics
α-Sympathomimetics can be used systemically in certain types of hypotension (p.324) and locally for nasal or conjunctival decongestion (p.336) or as adjuncts in infiltration anesthesia (p.204) for the purpose of delaying the removal of local anesthetic. With local use, underperfusion of the vasoconstricted area results in a lack of oxygen (A). In the extreme case, local hypoxia can lead to tissue necrosis. The appendages (e.g., digits, toes, ears) are particularly vulnerable in this regard, thus precluding vasoconstrictor adjuncts in infiltration anesthesia at these sites.
Vasoconstriction induced by an α-sympa- thomimetic is followed by a phase of enhanced blood flow (reactive hyperemia, A). This reaction can be observed after applying α-sympathomimetics (naphazoline, tetrahydrozoline, xylometazoline) to the nasal mucosa. Initially, vasoconstriction reduces mucosal blood flow and, hence, capillary pressure. Fluid exuded into the interstitial space is drained through the veins, thus shrinking the nasal mucosa. Owing to the reduced supply of fluid, secretion of nasal mucus decreases. In coryza, nasal patency is restored. However, after vasoconstriction subsides, reactive hyperemia causes renewed exudation of plasma fluid into the interstitial space, the nose is “stuffy” again, and the patient feels a need to reapply decongestant. In this way, a vicious cycle threatens. Besides rebound congestion, persistent use of a decongestant entails the risk of atrophic damage caused by the prolonged hypoxia of the nasal mucosa.
α-Sympatholytics (B). The interaction of norepinephrine with α-adrenoceptors can be inhibited by α-sympatholytics (α-adreno- ceptor antagonists, α-blockers). This inhibition can be put to therapeutic use in antihypertensive treatment (vasodilation † peripheral resistance ø, blood pressure ø, p.122). The first α-sympatholytics blocked the action of norepinephrine not only at postsynaptic α1-adrenoceptors but also at
presynaptic α2-receptors (nonselective α- blockers, e.g., phenoxybenzamine, phentolamine).
Presynaptic α2-adrenoceptors function like sensors that enable norepinephrine concentration outside the axolemma to be monitored, thus regulating its release via a local feedback mechanism. When presynaptic α2-receptors are stimulated, further release of norepinephrine is inhibited. Conversely, their blockade leads to uncontrolled release of norepinephrine with an overt enhancement of sympathetic effects at β1- adrenoceptor-mediated myocardial neuroeffector junctions, resulting in tachycardia and tachyarrhythmia.
Selective α1-Sympatholytics (α1-blockers, e.g., prazosin, or the longer-acting terazosin and doxazosin) do not disinhibit norepinephrine release.
α1-Blockers may be used in hypertension (p.315). Because they prevent reflex vasoconstriction, they are likely to cause postural hypotension with pooling of blood in lower limb capacitance veins during change from the supine to the erect position (orthostatic collapse, p.324).
In benign hyperplasia of the prostate, α1- blockers (terazosin, alfuzosin, tamsulosin) may serve to lower tonus of smooth musculature in the prostatic region and thereby improve micturition. Tamsulosin shows enhanced af nity for the α1A subtype; the risk of hypotension is therefore supposedly diminished.
α-Sympathomimetics, α-Sympatholytics |
95 |
A.Reactive hyperemia due to α -sympathomimetics, e.g., following decongestion of nasal mucosa
Before |
α -Agonist |
After |
Naphazolin
N
CH2
N
H
O2 supply = O2 demand |
O2 supply < O2 demand |
O2 supply < O2 demand |
B. Autoinhibition of norepinephrine release and α -sympatholytics
α 2 |
|
|
|
α |
2 |
|
|
α |
2 |
NE |
Nonselective |
|
|
|
α |
|
|
||
α |
-blocker |
|
|
|
|
1-blocker |
|
||
α 1 |
β 1 |
α 1 |
|
|
|
β 1 |
|
α 1 |
β 1 |
C. Indications for α 1-sympatholytics |
|
|
|
|
|
|
|
||
High blood pressure |
|
|
|
α 1-blocker |
|
Benign |
|||
|
|
|
e.g., terazosin |
|
prostatic hyperplasia |
||||
|
|
|
|
|
|
|
O |
|
|
|
|
|
|
|
|
N |
|
|
|
|
|
H3CO |
|
|
N |
N |
O |
|
|
|
|
H3CO |
|
|
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NH2 |
|
|
|
|
|
|
|
Inhibition of |
|
|
|
|||
|
|
|
α |
|
1-adreneric |
|
|
|
|
|
Resistance |
stimulation of |
|
Neck of bladder, |
|||||
|
smooth muscle |
|
|||||||
|
arteries |
|
|
prostate |
|||||
|
|
|
|
|
|
|
|||

96 Drugs Acting on the Sympathetic Nervous System
β-Sympatholytics (β-Blockers)
β-Sympatholytics are antagonists of norepinephrine and epinephrine at β-adrenocep- tors; they lack af nity for α-receptors.
Therapeutic effects. β-Blockers protect the heart from the oxygen-wasting effect of sympathetic inotropism by blocking cardiac β-receptors; thus, cardiac work can no longer be augmented above basal levels (the heart is “coasting”). This effect is utilized prophylactically in angina pectoris to prevent myocardialstressthat could trigger an ischemic attack (p.316). β-Blockers also serve to lower cardiac rate (sinus tachycardia, p.136) and protect the failing heart against excessive sympathetic drive (p.322). β-Blockers lower elevated blood pressure. The mechanism underlying their antihypertensive action is unclear. Applied topically to the eye, β- blockers are used in the management of glaucoma; they lower production of aqueous humor (p.346).
Undesired effects. β-Blockers are used very frequently and are mostly well tolerated if risk constellations are taken into account. The hazards of treatment with β-blockers become apparent particularly when continuous activation of β-receptors is needed in order to maintain the function of an organ.
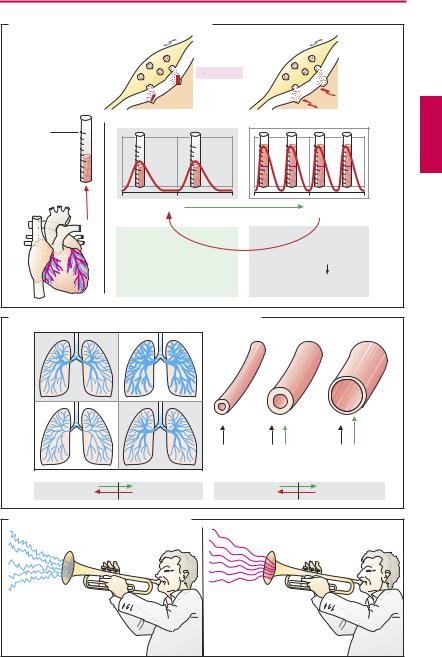
Congestive heart failure. For a long time, β- blockers were considered generally contraindicated in heart failure. Increased release of norepinephrine givesrise to an increase in heart rate and systolic muscle tension, enabling cardiac output to be maintained despite progressive cardiac disease. When sympathetic drive is eliminated during β- receptor-blockade, stroke volume and cardiac rate decline, a latent myocardial insuf - ciency is unmasked, and overt insuf ciency is exacerbated. Sympathoactivation not only helps for some time to maintain pump function in chronic congestive failure but itself also contributes to the progression of insufficiency: triggering of arrhythmias, in-
creased O2-consumption, enhanced cardiac hypertrophy (A).
On the other hand, convincing clinical evidence demonstrates that, under appropriate conditions (prior testing of tolerability, low dosage), β-blockers are able to improve prognosis in congestive heart failure. Protection against heart rate increases and arrhythmias may be important underlying factors.
Bradycardia, AV block. Elimination of sympathetic drive can lead to a marked fall in cardiacrateaswellastodisordersofimpulse conduction from the atria to the ventricles.
Bronchial asthma. Increased sympathetic activity prevents bronchospasm in patients disposed to paroxysmal constriction of the bronchial tree (bronchial asthma, bronchitis in smokers). In this condition, β2-receptor blockade may precipitate acute respiratory distress (B).
Hypoglycemia in diabetes mellitus. When treatment with insulin or oral hypoglycemics in the diabetic patient lowers blood glucose below a critical level, epinephrine is released, which then stimulates hepatic glucose release via activation of β2-recep- tors. β-Blockers suppress this counterregulation, besides masking other epinephrinemediated warning signs of imminent hypoglycemia, such as tachycardia and anxiety. The danger of hypoglycemic shock is therefore aggravated.
Altered vascular responses: When β2-re- ceptors are blocked, the vasodilating effect of epinephrine is abolished, leaving the α- receptor-mediated vasoconstriction unaffected: “cold hands and feet.”
β-Blockers exert an “anxiolytic” action that may be due to the suppression of somatic responses (palpitations; trembling) to epinephrine release that is induced by emotional stress; in turn, these responses would exacerbate “anxiety” or “stage-fright.” Because alertness is not impaired by β-block- ers, these agents are occasionally taken by orators and musicians before a major performance (C).
β-Sympatholytics (β-Blockers) |
97 |
|
A. β -Sympatholytics: effect on cardiac function |
|
|
β -Blocker |
β -Receptor |
|
blocks |
|
|
receptor |
|
|
100 ml |
|
|
Stroke |
|
|
volume |
|
|
1 sec |
|
|
β 1-Stimulation |
|
|
β 1-Blockade |
|
|
Heart is |
Exercise |
|
“coasting“ |
capacity |
|
B. β -Sympatholytics: effect on bronchial and vascular tone
Healthy |
|
|
|
|
|
|
|
|
|
|
Asthmatic |
|
|
|
α |
α |
β |
2 |
|
α |
β 2 |
β |
2-Blockade |
β 2-Stimulation |
β |
2-Blockade |
|
|
|
β |
2-Stimulation |
|
C. “Anxiolytic” effect of β -sympatholytics |
|
|
|
|
|
|
|
|
||
|
|
|
β -Blockade |
|
|
|
|
|
|
|