


|
|
|
|
|
|
|
Glucocorticoid Therapy |
245 |
||||
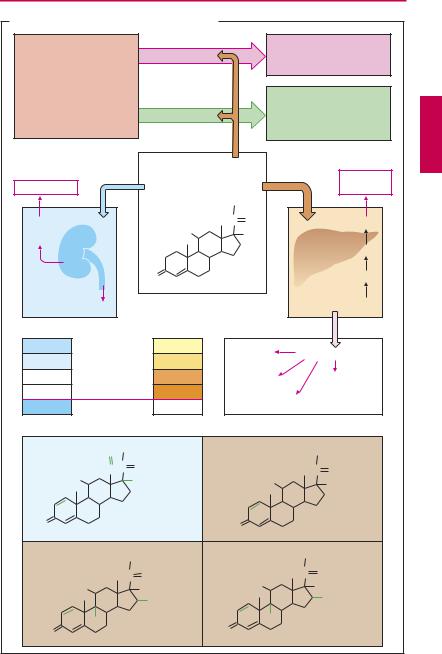
A. Glucocorticoids: principal and adverse effects |
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
e.g., allergy |
|
||
|
Inflammation |
|
Unwanted |
|
|
|
autoimmune disease, |
|
||||
|
|
|
|
|
|
|
|
|
transplant rejection |
|
||
|
redness, |
|
|
|
|
|
|
|
|
|
|
|
|
swelling heat, |
|
|
|
|
|
|
|
|
|
|
|
|
pain; |
|
|
|
|
|
|
|
Healing of |
|
||
|
scar |
|
|
Wanted |
|
|
|
tissue injury |
|
|||
|
|
|
|
|
|
|
due to bacteria, |
|
||||
|
|
|
|
|
|
|
|
|
viruses, fungi, trauma |
|
||
|
|
Mineralocorticoid |
|
|
|
|
|
Glucocorticoid |
|
|||
|
|
action |
|
|
Unphysiologically |
|
|
|
action |
|
|
|
|
|
|
|
|
high concentration |
|
|
|
|
Diabetes |
|
|
|
Hypertension |
|
|
|
|
|
|
|
|
mellitus |
|
|
|
|
|
|
|
Cortisol |
|
CH2OH |
|
|
|
|
|
|
Na+ |
|
|
|
HO |
|
C |
O |
|
|
Glucose |
|
|
H2O |
|
|
|
|
|
OH |
|
|
|
|
|
|
|
|
|
|
|
|
|
Gluconeogenesis |
|
|||
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
O |
|
|
|
|
|
Amino acids |
|
|
|
K+ |
|
|
|
|
|
|
Protein catabolism |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
Cortisol |
|
1 |
|
Muscle |
Tissue atrophy |
|
||||
|
0.8 |
Prednisolone |
|
4 |
|
weakness |
|
|||||
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
||||
Potency |
0 |
Triamcinolone |
|
7.5 |
|
Osteo- |
|
|
Skin |
|
||
0 |
Dexamethasone |
30 |
|
porosis |
|
|
atrophy |
|
||||
|
|
|
|
|
|
|
||||||
3000 |
Aldosterone |
|
0.3 |
|
Growth inhibition |
|
|
|
||||
|
|
O CH2OH |
|
|
|
|
|
CH2OH |
|
|||
|
|
HC C |
O |
|
|
|
|
|
|
C |
O |
|
|
|
HO |
H |
|
|
|
|
HO |
|
OH |
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
O |
|
Aldosterone |
|
O |
|
|
|
Prednisolone |
|
||
|
|
|
|
|
|
|
|
|||||
|
|
|
CH2OH |
|
|
|
CH2OH |
|
||||
|
|
|
C |
O |
|
|
|
C |
O |
|
||
|
|
|
|
|
HO |
|
|
|
|
|||
|
|
HO |
OH |
|
|
|
OH |
|
||||
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
CH3 |
|
|||
|
|
|
|
|
OH |
|
|
|
|
|
|
|
|
|
F |
|
|
|
|
|
F |
|
|
|
|
|
|
|
|
|
O |
|
|
|
|
|
|
|
|
O |
|
Triamcinolone |
|
|
|
Dexamethasone |
|
||||
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|||||

|
|
|
|
|
Glucocorticoid Therapy |
|
247 |
||
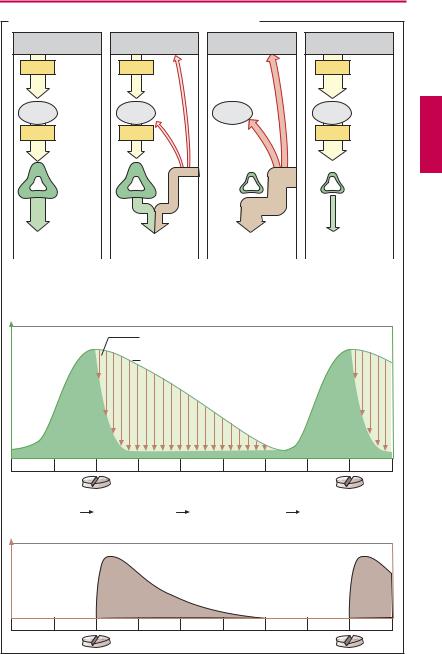
A. Cortisol release and its modification by glucocorticoids |
|
|
|
|
|||||
Hypothalamus |
|
|
|
|
|
|
|
|
|
CRH |
|
|
|
|
|
|
|
|
|
|
Hypo- |
|
|
|
|
|
|
|
|
|
physis |
|
|
|
|
|
|
|
|
ACTH |
|
|
|
|
Adreno- |
|
|
|
|
|
|
|
|
|
cortical |
|
|
|
|
|
|
|
|
|
atrophy |
|
|
|
|
|
Adrenal |
|
|
|
|
|
|
|
|
|
cortex |
|
|
|
|
|
|
|
|
Cortisol |
|
|
|
Exogenous |
|
|
|
|
|
|
|
|
admini- |
|
|
|
|
|
|
30 mg/day |
|
|
stration |
|
|
|
|
|
|
Cortisol |
|
|
Decrease in |
|
Cessation of |
|
Cortisol deficiency |
||
production under |
|
cortisol production |
cortisol production |
after abrupt |
|
||||
normal |
|
|
with cortisol dose |
with cortisol dose |
cessation of |
|
|
||
conditions |
|
|
< daily production |
> daily production |
administration |
|
|||
Cortisol |
|
|
Glucocorticoid-induced |
|
|
|
|
||
concentration |
|
inhibition of cortisol production |
|
|
|
|
|||
|
|
|
normal circadian time-course |
|
|
|
|
||
0 |
4 |
8 |
12 |
16 |
20 |
24 |
4 |
8 |
h |
Morning dose |
Inhibition of |
|
Elimination of |
|
Start of early |
|
|||
|
|
endogenous |
|
exogenous |
|
morning |
|
|
|
|
|
cortisol |
|
glucocorticoid |
|
cortisol |
|
|
|
|
|
production |
|
during daytime |
|
production |
|
|
|
Glucocorticoid |
|
|
|
|
|
|
|
|
|
concentration |
|
|
|
|
|
|
|
|
|
0 |
4 |
8 |
12 |
16 |
20 |
24 |
4 |
8 |
h |

Androgens, Anabolic Steroids, Antiandrogens |
249 |
A. Testosterone |
|
|
|
|
|
|
|
|
|
|
Hypothalamus |
|
|
Substitution |
|
|
O |
|
|
|
|
|
|
|
|
|
|
O |
C |
|
|
|
|
GnRH |
|
|
|
|
|
Testosterone |
|
p.o. |
|
|
|
|
|
|
|
|
undecanoate |
|
|
|
|
|
|
|
transdermal |
|
|
|
|
|
|
Hypophysis |
|
|
|
|
|
|
|
|
|
|
|
LH |
|
|
i.m. |
|
|
Intestinal lymph |
|||
|
|
|
|
Testosterone ester |
|
|
|
|
|
|
Testosterone |
|
|
|
|
|
e.g., skeletal muscle fiber |
||||
|
|
|
|
|
|
|
|
|
||
|
OH |
|
|
|
|
Androgen receptor |
||||
|
|
|
|
|
|
|
||||
O |
|
|
|
|
|
|
Gene expression |
|||
|
|
|
|
|
|
|
|
|
|
|
e.g., Prostatic |
|
|
|
|
|
O |
|
|
|
|
gland cell |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
Conjugation with |
|||
|
|
|
|
|
|
|
|
|
||
5α -Reductase |
|
|
|
|
|
|
|
sulfate, glucuronate |
||
|
|
|
|
HO |
|
H |
|
|
|
|
|
|
|
|
|
H |
|
|
|
|
|
|
O |
|
|
|
Androsterone |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
Dihydro- |
H H |
|
|
|
|
|
|
|
|
|
testosterone |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
17-Keto- |
|
|
|
|
|
|
|
|
|
|
steroid |
I n h i b i t o r y P r i n c i p l e s |
|
Receptor antagonists |
||||||||
|
|
|
|
|
|
|||||
|
GnRH superagonists |
|
|
|
|
|
CH3 |
|
||
|
|
|
|
|
|
C |
O |
|
||
|
|
|
|
|
|
|
|
|
||
5α -Reductase inhibitor |
|
|
H2C |
|
|
O C |
CH3 |
|||
|
|
|
|
O |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
O |
|
CH3 |
|
|
|
Cyproterone |
|||
|
C |
NH |
C |
CH3 |
|
O |
|
|||
|
|
Cl |
acetate |
|||||||
|
|
|
CH3 |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
F3C |
Flutamide |
CH3 |
||
|
|
|
|
|
|
|
|
|
||
O |
N |
Finasteride |
O2N |
NH |
C |
C |
H |
|||
|
H |
|
|
|
O |
CH3 |
||||
|
|
|
|
|
|
|
|
|||