



Inhibitors of Cell Wall Synthesis |
273 |
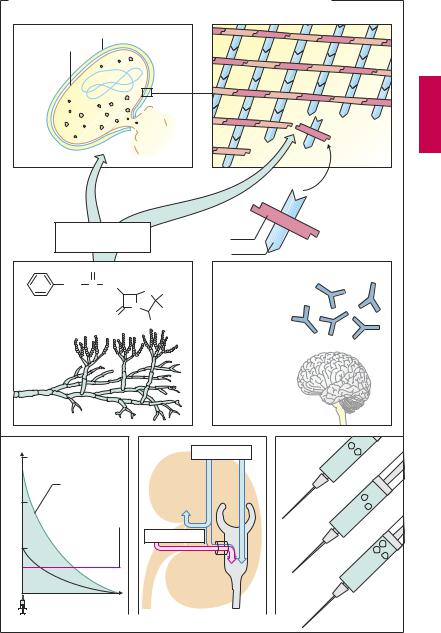
A. Disadvantages of penicillin G |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
6-Aminopenicillanic acid |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
O |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CH2 |
C |
NH |
S |
CH3 |
Salmonella typhi |
|
|
|
|
active |
||||
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
O |
N |
CH3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COOH |
|
|
|
|
|
|
|
|
Not |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
negative |
|||
Penicillin G |
|
|
|
|
|
|
E. coli |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
Gram |
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Acid sensitivity |
|
|
|
|
Penicillinase |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
sensitivity |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Treponema |
|
|
|
|
|
|
Gonococci |
|
|
|
|
|
|
|
|
|
pallidum |
|
|
|
|
|
|
||
|
|
|
|
H+Cl- |
|
Penicillinase |
actionspectrum |
|
|
|
positive |
|
|
|
|
|
|
|
|
|
|
|
|
Active |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
Gram |
- |
|
|
|
Pneumococci |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
Narrow- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Staphylococci |
|
|
|
|
|
|
|
Streptococci |
|
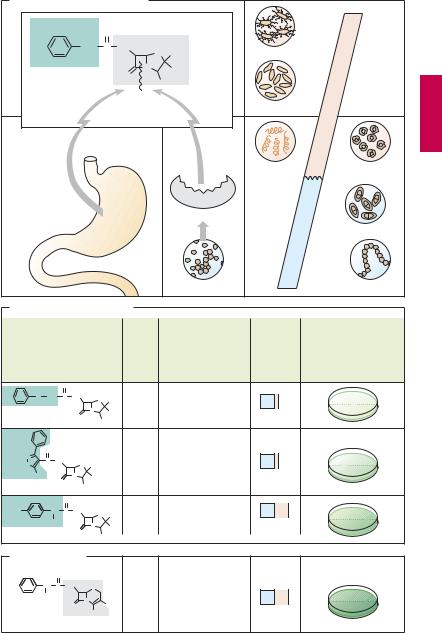
B. Derivatives of penicillin G |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Concentration needed |
|||
|
|
|
|
|
|
Acid |
Penicillinase |
Spectrum |
|
|
|
to inhibit penicillin G- |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
sensitive bacteria |
|||
|
O |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
O |
CH2 C |
NH |
S |
CH3 |
Resis- |
Sensitive |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Penicillin V |
O |
N |
CH3 |
tant |
|
|
Narrow |
|
|
|
|
|
|
|
||
|
|
COOH |
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
N |
O |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
C NH |
|
|
|
|
Resis- |
Resistant |
|
|
|
|
|
|
|
|
|
|
O |
S |
CH3 |
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
tant |
|
|
|
|
|
|
|
|
|
|
|||
CH3 |
|
N |
CH3 |
|
|
|
|
Narrow |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Oxacillin O |
COOH |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
O |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HO |
CH C |
NH |
S |
CH3 |
Resis- |
Sensitive |
|
|
|
|
|
|
|
|
|
|
|
NH2 |
|
tant |
|
|
|
|
|
|
|
|
|
|
|||
|
|
N |
CH3 |
|
|
Broad |
|
|
|
|
|
|
|
|||
Amoxicillin |
O |
|
|
|
|
|
|
|
|
|
|
|||||
COOH |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
C. Cephalosporin |
|
|
|
|
|
O |
|
|
|
|
|
CH C |
NH |
S |
|
Resistant, |
|
|
|
|
|
||
NH2 |
|
|
Resis- |
|
|
N |
|
but sensitive to |
|
||
Cefalexin |
O |
CH3 |
tant |
cephalosporinase |
Broad |
|
COOH |
||||
|
|
|
|||