


Drugs for Maintaining Calcium Homeostasis |
267 |
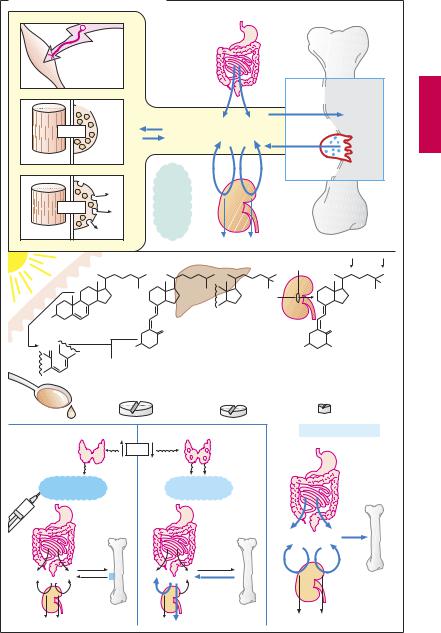
A. Calcium homeostasis of the body |
|
|
|
|
|
|||||
|
Electrical |
|
|
|
|
|
|
|
|
|
|
excitability |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Bone trabeculae |
|
|
|
1 x 10-7M |
|
|
|
|
|
|
Hydroxyapatite crystals |
|
|
~ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Ca2+ |
|
cell function |
|
1 x 10-3M |
Ca2+ + PO43- |
Ca10(PO4)6(OH)2 |
||||
|
|
|
|
|||||||
Muscle cell |
Gland cell |
|
|
|
|
|
|
|
||
|
|
|
on |
~1 |
Ca |
|
|
|
Osteoclast |
|
|
|
~10-5M |
Effect |
|
|
|
||||
|
|
|
x |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|||
|
|
|
10- |
|
|
|
|
|||
|
|
|
|
|
3 |
|
|
|
|
|
|
|
|
|
|
Albumin |
M |
|
|
|
|
Ca2+ |
|
|
|
Globulin |
|
|
|
|
||
Contraction |
Secretion |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|||
|
|
Skin |
|
|
|
|
|
Parathyroid hormone, Ca2+ , PO3- |
||
|
|
|
|
|
|
|
|
|
|
4 |
|
|
|
25 |
|
|
|
25 |
OH |
|
OH |
|
|
|
|
|
|
|
|
|
||
1 |
|
|
|
|
|
|
|
|
|
|
HO |
|
7 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7-Dehydrocholesterol |
|
|
CH2 |
|
|
|
CH2 |
|||
H2C |
|
|
HO |
1 |
|
|
|
|
HO |
OH |
|
|
|
|
|
|
|
||||
|
|
Cholecalciferol |
|
|
25-Hydroxychole- |
|
1,25-Dihydroxychole- |
|||
|
|
(vitamin D3) |
|
|
calciferol |
|
calciferol (calcitriol) |
|||
|
|
50 – 5000 g/day |
(calcifediol) |
|
0.5 – 2 g/day |
|||||
|
|
|
|
|
|
|
50 – 2000 g/day |
|
|
|
Cod liver oil |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Vit. D-Hormone |
Parafollicular |
|
|
Ca2+ |
|
|
|
|
Parathyroid |
|
|
cells of |
|
|
|
|
|
|
glands |
|
|
|
thyroid |
|
|
|
|
|
|
|
|
|
|
Calcitonin |
|
|
|
Parathyroid |
|
|
||||
|
|
|
hormone |
|
|
|
||||
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
Ca2+ + PO3- |
|
|
|
|
|
|
|
|
|
|
|
4 |

Drugs for Treating Bacterial Infections |
269 |
A. Principles of antibacterial therapy |
|
|
|
|
|
|
Anti- |
|
|
|
|
bacterial |
|
|
Bacterial |
|
drugs |
|
|
|
|
|
|
|
invasion: |
|
|
|
|
infection |
|
|
|
|
|
|
Selective |
|
|
|
|
antibacterial |
|
|
|
|
toxicity |
|
|
|
Immune |
|
|
|
1. |
defenses |
|
Body cells |
Bacteria |
|
Penicillins |
Bacitracin |
Polymyxins |
|
|
Cephalosporins |
Vancomycin |
Tyrothricin |
|
Cell wall |
DNA |
RNA |
|
Cell |
|
Tetrahydro- |
|
|
membrane |
|
|
|
|
|
|
folate |
|
Protein |
|
|
synthesis |
|
|
|
Bacterium |
Sulfonamides |
Rifampicin |
Tetracyclines |
|
Trimethoprim |
Aminoglycosides |
|
||
|
|
|||
|
|
|
Chloramphenicol |
|
|
“Gyrase-inhibitors” |
Erythromycin |
|
|
|
Clindamycin |
|
||
|
Nitroimidazoles |
|
||
2. |
|
|
||
|
|
|
|
|
|
1 day |
|
Resistance |
|
|
|
|
|
|
Antibiotic |
|
|
|
|
|
|
Insensitive strain |
|
|
|
Bactericidal |
|
|
|
3. |
Bacteriostatic |
Sensitive strain with |
Selection |
|
resistant mutant |
|
|||