


120 Biogenic Amines
Serotonin
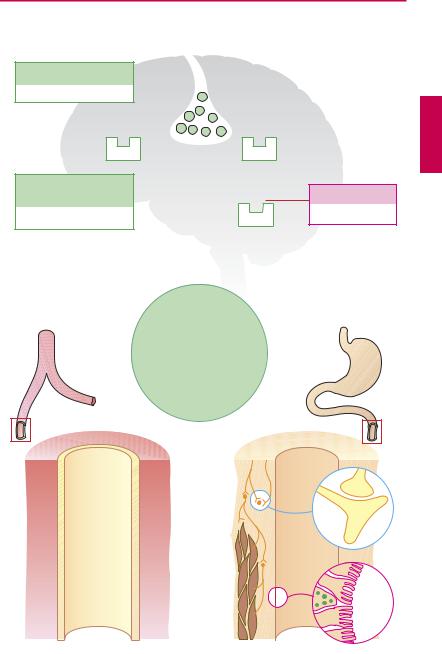
Occurrence. Serotonin (5-hydroxytrypta- mine, 5-HT) is synthesized from L-trypto- phan in enterochromaf n cells of the intestinal mucosa. 5-HT-synthesizing neurons occur also in the enteric nerve plexus and the CNS, where the amine fulfills a neuromediator function. Blood platelets are unable to synthesize 5-HT, but are capable of taking up, storing, and releasing it.
Serotonin receptors. Based on biochemical and pharmacological criteria, seven receptors classes can be distinguished. Of major pharmacotherapeutic importance are those designated: 5-HT1, 5-HT2, each with different subtypes, 5-HT4, and 5-HT7, all of which are G-protein-coupled, whereas the 5-HT3 subtype represents a ligand-gated nonselective cation channel (p.64).
Serotonin actions—cardiovascular system.
The responses to 5-HT are complex, because multiple, in part opposing, effects are exerted via the different receptor subtypes. Thus, 5-HT2A receptors on vascular smooth muscle cells mediate direct vasoconstriction. Vasodilation and lowering of blood pressure can occur by several indirect mechanisms: 5-HT1A receptors mediate sympathoinhibition († decreasein neurogenicvasoconstrictor tonus) both centrally and peripherally; 5-HT1-like receptors on vascular endothelium promote release of vasorelaxant mediators (NO; prostacyclin). 5-HT released from platelets plays a role in thrombogenesis, hemostasis, and the pathogenesis of preeclamptic hypertension.
Sumatriptan is an antimigraine drug that possesses agonist activity at 5-HT receptors of the 1D and 1B subtypes (p.334). It causes a constriction of cranial blood vessels, which may result from a direct vascular action or from inhibition of the release of neuropeptides that mediate “neurogenic inflammation.” A sensation of chest tightness may occur and be indicative of coronary vaso-
spasm. Other “triptans” are naratriptan, zolmitriptan, and rizatriptan.
Gastrointestinal tract. Serotonin released from myenteric neurons or enterochromaffin (EC) cells acts on 5-HT4 receptors to enhance bowel motility, enteral fluid secretion, and thus propulsive activity. To date, attempts at modifying the influence of serotonin on intestinal motility by agonistic or antagonistic drugs have not been very successful. Although the 5-HT4 agonist cisapride was shown to be effective in increasing propulsive activity of the intestinal tract, its adverse effects were very pronounced. Since it isdegraded via CYP3A4, it isliable to interact with numerous drugs. In particular, arrhythmias (in part severe) associated with QT prolongation were noted; the arrhythmogenic action is caused by blockade of K+ channels. The drug is no longer available.
Central nervous system. Serotoninergic neurons play a part in various brain functions, as evidenced by the effects of drugs likely to interfere with serotonin.
Fluoxetine is an antidepressant which, by blocking reuptake, retards inactivation of released serotonin. Its activity spectrum includes significant psychomotor stimulation and depression of appetite.
Sibutramine, an inhibitor of the neuronal reuptake of 5-HT and norepinephrine, is marketed as an antiobesity drug (pp.329).
Ondansetron, an antagonist at the 5-HT3 receptor, possesses striking effectiveness against cytotoxic drug-induced emesis, evident both at the start of and during cytostatic therapy. Tropisetron and granisetron produce analogous effects.
LSD and other psychedelics (psychotomimetics) such as mescaline and psilocybin can induce states of altered awareness, or induce hallucinations and anxiety, probably mediated by 5-HT2A receptors.
|
|
|
|
|
|
|
|
Serotonin |
|
121 |
A. Serotonin actions as influenced by drugs |
|
|
|
|
|
|
||||
Serotoninergic neuron |
|
|
|
|
|
|
|
|||
|
|
|
|
|
H |
|
|
|
|
CH3 |
LSD |
|
|
|
|
|
|
CH2 |
CH2 |
N |
|
|
|
|
|
|
N |
SO2 |
||||
Lysergic acid diethylamide |
|
|
|
CH2 |
|
CH3 |
||||
Psychedelic |
|
|
|
H3C |
|
|
N |
|
|
|
|
|
|
|
|
|
|
|
H |
|
|
Hallucination |
|
|
|
|
|
|
Sumatriptan |
|
||
|
|
|
|
|
|
|
|
|
||
|
|
5-HT2A |
|
|
|
5-HT1D |
Antimigraine |
|
||
|
|
|
|
|
|
|
|
|||
Fluoxetine |
|
|
|
|
|
|
|
Ondansetron |
|
|
5-HT-reuptake inhibitor |
|
|
|
|
|
|
||||
Antidepressant |
|
|
|
|
|
5-HT3 |
Antiemetic |
|
||
|
|
|
|
|
|
|
|
|||
|
|
|
H |
|
|
|
|
O |
CH2 |
CH3 |
|
|
|
|
|
|
|
|
|||
CH |
CH2 |
CH2 |
N |
|
|
|
Emesis |
N |
N |
|
|
|
|
|
|||||||
O |
|
|
CH3 |
|
|
|
|
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
F3C |
|
|
|
|
|
|
|
CH3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5-Hydroxy-tryptamine |
|
|
|
||||
|
|
|
HO |
CH2 |
CH2 |
NH2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
N |
|
|
|
|
|
|
|
|
|
|
H |
|
|
|
|
|
|
|
|
|
|
Serotonin |
|
|
|
|
|
|
Blood vessel |
|
|
|
|
|
|
Intestine |
|
|
|
|
Endothelium |
|
|
|
|
|
|
|
||
|
|
mediated Dilatation |
|
|
|
|
|
|
|
|
|
5-HT2B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5-HT4 |
|
|
|
Platelets |
Constriction |
|
|
|
|
|
|
||
|
|
|
|
|
|
Propulsive |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
motility |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
-HT |
|
|
|
|
|
Entero- |
|
|
|
|
5 |
|
|
|
|
|
chrom- |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
affin |
|
|
|
|
|
|
|
|
|
|
cell |
|

122 Vasodilators
Vasodilators—Overview
The distribution of blood within the circulation is a function of vascular caliber. Venous tone regulates the volume of blood returned to the heart and, hence, stroke volume and cardiac output. The luminal diameter of the arterial vasculature determines peripheral resistance. Cardiac output and peripheral resistance are prime determinants of arterial blood pressure (p.324).
In (A), the clinically most important vasodilators are presented. Some of these agents possess different ef cacy in affecting the venous and arterial limbs of the circulation.
Possible uses. Arteriolar vasodilators are given to lower blood pressure in hypertension (p.314), to reduce cardiac work in angina pectoris (p.318), and to reduce ventricular afterload (pressure load) in cardiac failure (p.322). Venous vasodilators are used to reduce venous filling pressure (preload) in anginapectoris(p.318) or congestive heartfailure (p.322). Practical uses are indicated for each drug group.
Counterregulation in acute hypotension due to vasodilators (B). Increased sympathetic drive raises heart rate (reflex tachycardia) and cardiac output and thus helps to elevate blood pressure. The patients experience palpitations. Activation of the renin– angiotensin–aldosterone (RAA) system serves to increase blood volume, hence cardiac output. Fluid retention leads to an increase in body weight and, possibly, edemas.
These counterregulatory processes are susceptible to pharmacological inhibition (β-blockers, ACE inhibitors, diuretics).
Mechanisms of action. The tonus of vascular smooth muscle can be decreased by various means.
Protection against vasoconstricting mediators. ACE inhibitors and angiotensin receptor antagonists protect against angiotensin II (p.128); α-adrenoceptor antagonists inter-
fere with (nor)epinephrine (p.94); bosentan (see below) is an antagonist at receptors for endothelin, a powerful vasoconstrictor released by the endothelium.
Substitution of vasorelaxant mediators. Analogues of prostacyclin (from vascular endothelium), such as iloprost, or of prostaglandin E1, such as alprostadil, stimulate the corresponding receptors; organic nitrates (p.124) substitute for endothelial NO.
Direct action on vascular smooth muscle cells. Ca2+-channel blockers (p.126) and K+ channel openers (diazoxide, minoxidil) act at the level of channel proteins to inhibit membrane depolarization and excitation of vascular smooth muscle cells. Phosphodiesterase (PDE) inhibitors retard the degradation of intracellular cGMP,which lowerscontractile tonus. Several PDE isozymes with different localization and function are known.
The following sections deal with special aspects:
Erectile dysfunction. Sildenafil, vardenafil, and tardalafil are inhibitors of PDE-5 and are used to promote erection. During sexual arousal NO is released from nerve endings in the corpus cavernosum of the penis, which stimulatesthe formation ofcGMP invascular smoothmuscle. PDE-5,whichisimportantin this tissue, breaks down cGMP, thus counteracting erection. BlockersofPDE-5“conserve” cGMP.
Pulmonary hypertension. This condition involves a narrowing of the pulmonary vascular bed resulting mostly from unknown causes. The disease often is progressive, associated with right ventricular overload, and all but resistant to treatment with conventional vasodilators. The endothelin antagonist, bosentan, offers a new therapeutic approach. Administration of NO by inhalation is under clinical trial.
|
|
Vasodilators—Overview |
123 |
A. Vasodilators |
|
|
|
|
|
Cerebral blood |
|
|
|
flow not subject |
|
|
|
to specific interventions |
|
Venous bed |
Vasodilation |
Arterial bed |
|
Nitrates |
|
|
|
|
|
Ca-antagonists |
|
ACE inhibitors, angiotensin antagonists |
|
|
|
|
|
Dihydralazine |
|
|
|
Bosentan |
|
α 1-Antagonists |
|
|
|
Nitroprusside sodium |
|
|
|
B. Counter-regulatory responses in hypotension due to vasodilators |
|
|||
|
|
Sympathetic nerves |
|
Vasoconstriction |
|
|
β |
-Blocker |
Blood |
|
|
|
|
|
Vasodilation |
Vasomotor |
|
|
pressure |
|
Heart rate |
|
|
|
|
center |
Cardiac |
|
|
Blood |
|
|
||
|
|
|
||
|
|
output |
|
|
pressure |
|
|
|
|
|
Blood volume |
|
|
|
|
|
|
|
|
|
|
Angiotensinogen |
Aldosterone |
|
Angiotensin- |
Renin |
|
|
|
converting |
|
|
|
|
enzyme |
|
Angiotensin I |
|
|
(ACE) |
|
|
|
|
ACE-inhibitors |
|
Angiotensin II |
|
Vasoconstriction |
|
|
|
||
Angiotensin II antagonists |
Renin-angiotensin-aldosterone system |
|||
|
|
|||