


202 Local Anesthetics
Local Anesthetics
Local anesthetics reversibly inhibit impulse generation and propagation in nerves. In sensory nerves, such an effect is desired when painful procedures must be performed, e.g., surgical or dental operations.
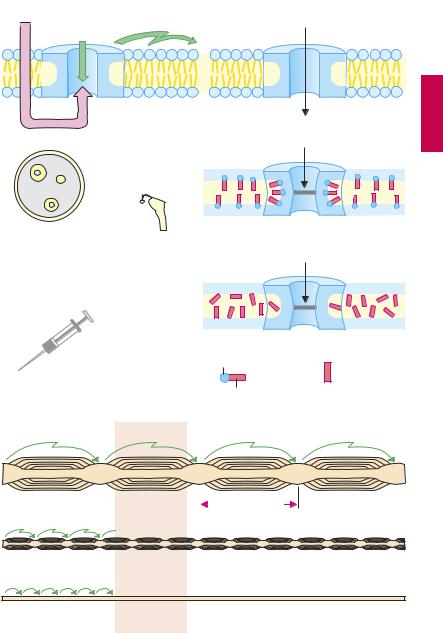
Mechanism of action. Axonal impulse conduction occurs in the form of an action potential. The change in potential involves a rapid influx of Na+ (A) through a membrane channel protein that, upon being opened (activated), permits rapid inward movement of Na+ down a chemical gradient ([Na+]outside ~ 150 mM, [Na+]inside ~ 7 mM). Local anesthetics are capable of inhibiting this rapid influx of Na+; initiation and propagation of excitation are therefore blocked (A).
Most local anesthetics exist in part in the cationic amphiphilic form (cf. p.206). This physicochemical property favors incorporation into membrane interphases between polar and apolar domains. These are found in phospholipid membranes and also in ion channel proteins. Some evidence suggests that Na+-channel blockade results from binding of local anesthetics to the channel protein. It appears certain that the site of action is reached from the cytosol, implying that the drug must first penetrate the cell membrane (p.204).
Local anesthetic activity is also shown by uncharged substances, suggesting a binding site in apolar regions of the channel protein or the surrounding lipid membrane.
Mechanism-specific adverse effects. Since local anesthetics block Na+ influx not only in sensory nerves but also in other excitable tissues (A and p.206), they are applied locally. Depression of excitatory processes in the heart, while undesired during local anesthesia, can be put to therapeutic use in cardiac arrhythmias (p.138).
Forms of local anesthesia. Local anesthetics are applied via different routes, including infiltration of the tissue (infiltration anesthesia) or injection next to the nerve branch carrying fibers from the region to be anesthetized (conduction anesthesia of the nerve, spinal anesthesia of segmental dorsal roots), or by application to the surface of the skin or mucosa (surface anesthesia). In each case, the local anesthetic drug is required to diffuse to the nerves concerned from a depot placed in the tissue or on the skin.
High sensitivity of sensory, low sensitivity of motor nerves. Impulse conduction in sensory nerves is inhibited at a concentration lower than that needed for motor fibers. This difference may be due to the higher impulse frequency and longer action potential duration in nociceptive as opposed to motor fibers. Alternatively, it may relate to the thickness of sensory and motor nerves, as well as the distance between nodes of Ranvier. In saltatory impulse conduction, only the nodal membrane is depolarized. Because depolarization can still occur after blockade of three or four nodal rings, the area exposed to a drug concentration suf cient to cause blockade must be larger for motor fibers (p.203B).
This relationship explains why sensory stimuli that are conducted via myelinated Aδ-fibers are affected later and to a lesser degree than are stimuli conducted via unmyelinated C-fibers. Since autonomic postganglionic fibers lack a myelin sheath, they are susceptible to blockade by local anesthetics. As a result, vasodilation ensues in the anesthetized region, because sympathetically driven vasomotor tone decreases. This local vasodilation is undesirable (see opposite).
Local Anesthetics |
203 |
A. Effects of local anesthetics
Local anesthetic |
Propagated |
|
Na+ |
|
|
Na+-entry |
impulse |
Activated |
|
|
|
|
Na+-channel |
|
|||
|
inside |
|
|
inside |
|
Peripheral nerve |
CNS |
Blocked |
Na+ |
|
|
|
|
||||
|
|
|
|
||
|
|
Na+-channel |
|
||
Perineurium |
|
|
|
||
Conduction |
Restlessness, |
|
Na+ |
|
|
block |
convulsions, |
|
|
||
|
respiratory |
Blocked |
|
|
|
|
paralysis |
Na+-channel |
|
||
|
Heart |
|
|
|
|
|
|
polar |
Cationic |
Uncharged |
|
|
Impulse |
+ |
amphiphilic |
local |
|
Local |
conduction |
local |
anesthetic |
||
|
|||||
application |
cardiac arrest |
apolar |
anesthetic |
|
|
B. Inhibition of impulse conduction in different types of nerve fibers
Local anesthetic
Aα motor |
|
|
|
0.8–1.4 mm |
|
||||
|
|
Aδ sensory 

 0.3–0.7 mm
0.3–0.7 mm
Csensory and postganglionic

204 Local Anesthetics
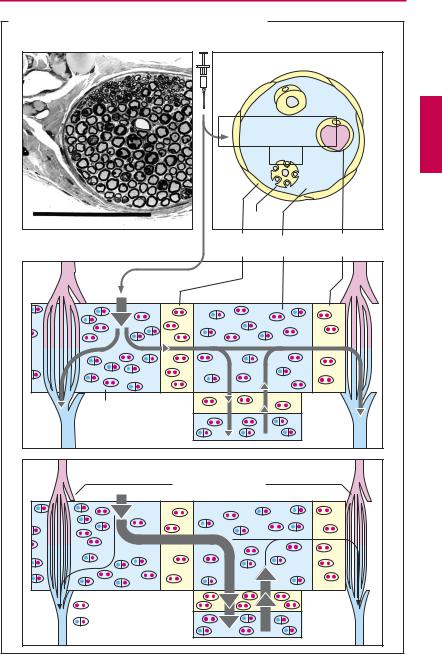
Diffusion and effect. During diffusion from the injection site (i.e., the interstitial space of connective tissue) to the axon of a sensory nerve, the local anesthetic must traverse the perineurium. The multilayered perineurium is formed by connective tissue cells linked by zonulae occludentes (p.22) and therefore constitutes a closed lipophilic barrier.
Local anesthetics in clinical use are usually tertiary amines; at the pH of interstitial fluid these exist partly as the neutral lipophilic base (symbolized by particles marked with two red dots) and partly as the protonated form, i.e., amphiphilic cation (symbolized by particles marked with one blue and one red dot). The uncharged form can penetrate the perineurium and enters the endoneural space, where a fraction of the drug molecules regains a positive charge in keeping with the local pH. The same process repeats itself when the drug penetrates through the axonal membrane (axolemma) into the axoplasm from which it exerts its action on the sodium channel; and again when it diffuses out of the endoneural space through the unfenestrated endothelium of capillaries into the blood.
The concentration of local anesthetic at the site of action is, therefore, determined by the speed of penetration into the endoneurium and axoplasm and the speed of diffusion into the capillary blood. To enable a suf ciently fast build-up of drug concentration at the site of action, there must be a correspondingly large concentration gradient between drug depot in the connective tissue and the endoneural space. Injection of solutions of low concentration will fail to produce an effect; however, too high concentrations must also be avoided because of the danger of intoxication resulting from too rapid systemic absorption into the blood.
To ensure a reasonably long-lasting local effect with minimal systemic action, a vasoconstrictor (epinephrine, less frequently norepinephrine or vasopressin derivatives) is often co-administered in an attempt to confine the drug to its site of action. Asblood
flow is diminished, diffusion from the endoneural space into the capillary blood decreases. Addition of a vasoconstrictor, moreover, helps to create a relative ischemia in the surgical field. Potential disadvantages of catecholamine-type vasoconstrictors include the reactive hyperemia following washout of the constrictor agent (p.94) and cardiostimulation when epinephrine enters the systemic circulation. In lieu of epinephrine, the vasopressin analogue felypressin can be used as adjunctive vasoconstrictor (less pronounced reactive hyperemia, no arrhythmogenic action, but danger of coronaryconstriction). Vasoconstrictorsmustnot be applied in local anesthesia involving the appendages (e.g., fingers, toes).
|
Local Anesthetics |
205 |
||
A. Disposition of local anesthetics in peripheral nerve tissue |
|
|
|
|
0.1 mm |
Axon |
|
|
|
|
|
|
|
|
Cross section through peripheral |
Perineurium |
Endoneural |
Capillary |
|
nerve (light microscope) |
|
|||
|
space |
wall |
|
|
Inter- |
Axolemma |
|
|
|
stitium |
Axoplasm |
|
|
|
|
|
|
|
|
|
Vasoconstriction |
|
|
|
|
e.g., with epinephrine |
|
|
|
lipophilic |
Axolemma |
|
|
|
amphiphilic |
Axoplasm |
|
|
|

206 Local Anesthetics
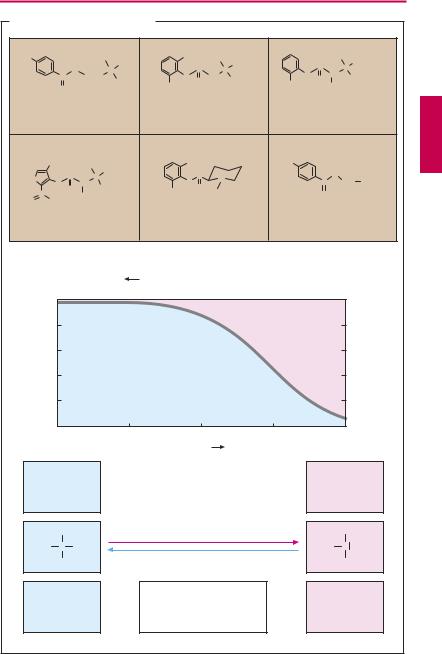
Characteristics of chemical structure. Local anesthetics possess a uniform structure. Generally they are secondary or tertiary amines. The nitrogen is linked through an intermediary chain to a lipophilic moiety— most often an aromatic ring system.
The amine function means that local anesthetics exist either as the neutral amine or as the positively charged ammonium cation, depending upon their dissociation constant (pKa value) and the actual pH value. The pKa of typical local anesthetics lies between 7.5 and 9. In its protonated form, the molecule possesses both a polar hydrophilic moiety (protonated nitrogen) and an apolar lipophilic moiety (ring system)—it is amphiphilic.
Depending on the pKa, from 50% to 5% of the drug may be present at physiological pH in the uncharged lipophilic form. This fraction is important because it represents the lipid membrane-permeable form of the local anesthetic (p.26), which must take on its cationic amphiphilic form in order to exert its action (p.202).
Clinically used local anesthetics are either esters or amides. Even drugs containing a methylene bridge, such as chlorpromazine (p.233) or imipramine (p.229) would exert a local anesthetic effect with appropriate application. Ester-type local anesthetics are subject to inactivation by tissue esterases. This is advantageous because of the diminished danger of systemic intoxication. On the other hand, the high rate of bioinactivation and, therefore, shortened duration of action is a disadvantage.
Procaine cannot be used as surface anesthetic because it is inactivated faster than it can penetrate the dermis or mucosa. In mepivacaine, the nitrogen atom usually located at the end of the side chain forms part of a cyclohexane ring.
Lidocaine is broken down primarily in the liver by oxidative N-dealkylation. This step can occur only to a restricted extent in prilocaine and carticaine because both carry a substituent on the C-atom adjacent to the nitrogen group. Carticaine possesses a car-
boxymethyl group on its thiophene ring. At this position, ester cleavage can occur, resulting in the formation of a polar COO– group, loss of the amphiphilic character, and conversion to an inactive metabolite.
Benzocaine is a member of the group of local anesthetics lacking a nitrogen atom that can be protonated at physiological pH. It is used exclusively as a surface anesthetic.
Other agents employed for surface anesthesia include the uncharged polidocanol and the catamphiphilic tetracaine and lidocaine (e.g. as a 5% gel).
Adverse effects of local anesthetics (LAs).
The cellular point of attack of LAs is a “fast“ Na+ channel, opening of which initiates the action potential. LAs block this channel. Fast sodium channels also operate in other excitable tissues including nerve cells of the brain and muscle or specialized conducting tissues of the heart. The action of LAs is thus not confined to nerve tissue; it is not organ-spe- cific. Accordingly, serious adverse effects occur when LAs enter the circulation too rapidly or in too high concentrations. In the heart, impulse conduction is disrupted, as evidenced by atrioventricular block or, at worst, ventricular arrest. In the CNS, different regions are perturbed with a resultant loss of consciousness and development of seizures. Since no specific LA antidote is available, symptomatic countermeasures need to be taken immediately. If signs of cardiac inhibition predominate, epinephrine must be given intravenously. If CNS toxicity is present, anticonvulsant drugs have to be administered (e.g., diazepam i.v.).
|
|
|
|
|
|
|
|
|
|
|
Local Anesthetics |
207 |
|||
A. Local anesthetics and pH value |
|
|
|
|
|
|
|
||||||||
H2N |
|
|
H5C2 + |
C H |
5 |
CH3 |
H5C2 + C2H5 |
|
C |
|
H + C3H7 |
|
|||
|
|
|
O |
N |
2 |
C |
N |
|
N |
|
N |
|
|||
|
|
C |
(CH ) |
2 |
|
H |
|
N |
CH2 |
H |
O |
CH |
|
||
|
|
|
2 |
|
|
H O |
|
H |
|
H |
|
||||
|
|
O |
|
|
|
|
|
CH3 |
|
|
CH3 |
|
CH3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
Procaine |
|
|
|
|
Lidocaine |
|
|
Prilocaine |
|
||||
|
CH3 |
H |
C |
H |
|
|
CH3 |
|
|
H2N |
|
|
|
|
|
|
|
C |
+ |
7 |
|
C |
H |
|
|
|
O |
|
|||
S |
|
N |
3 |
|
|
|
|
|
|
||||||
|
N |
CH |
H |
|
|
|
N |
N+ |
|
|
C |
|
CH2 CH3 |
|
|
|
C |
H O |
CH3 |
|
|
|
CH3 H O H C |
|
|
O |
|
|
|
||
O |
|
|
|
|
|
|
3 |
|
|
|
|
|
|||
OCH3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Carticaine |
|
|
|
|
Mepivacaine |
|
Benzocaine |
|
|||||
|
|
|
|
|
|
|
|
[H+] Proton concentration |
|
|
|
|
|
||
|
100 |
|
|
|
|
|
|
|
|
|
|
|
|
0 |
|
|
80 |
|
|
|
|
|
|
|
|
|
|
|
|
20 |
|
|
60 |
|
|
|
|
|
|
|
|
|
|
|
|
40 |
|
|
40 |
|
|
|
|
|
|
|
|
|
|
|
|
60 |
|
|
20 |
|
|
|
|
|
|
|
|
|
|
|
|
80 |
|
|
0 |
6 |
|
|
|
7 |
|
8 |
|
|
9 |
|
|
100 |
|
|
|
|
|
|
|
|
|
|
|
10 |
|
||||
|
|
|
|
|
|
|
|
pH value |
|
|
|
|
|
|
|
|
Active form |
|
|
|
|
|
|
|
|
Membrane- |
|
||||
|
cationic- |
|
|
|
|
|
|
|
|
|
permeable |
|
|||
|
amphiphilic |
|
|
|
|
|
|
|
|
lipophilic form |
|
||||
|
|
R' |
|
|
|
|
|
|
|
|
|
|
|
R' |
|
|
R |
+ |
H |
|
|
|
|
|
|
|
|
|
R |
N |
|
|
N |
|
|
|
|
|
|
|
|
|
|
||||
|
|
R'' |
|
|
|
|
|
|
|
|
|
|
|
R'' |
|
|
|
|
|
|
|
|
|
Ability to penetrate |
|
|
|
|
|
||
|
Poor |
|
|
|
|
|
lipophilic |
|
|
|
|
|
Good |
|
|
|
|
|
|
|
|
barriers and |
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
cell membranes |
|
|
|
|
|
|
|