


144 Antithrombotics
Prophylaxis and Therapy of Thromboses
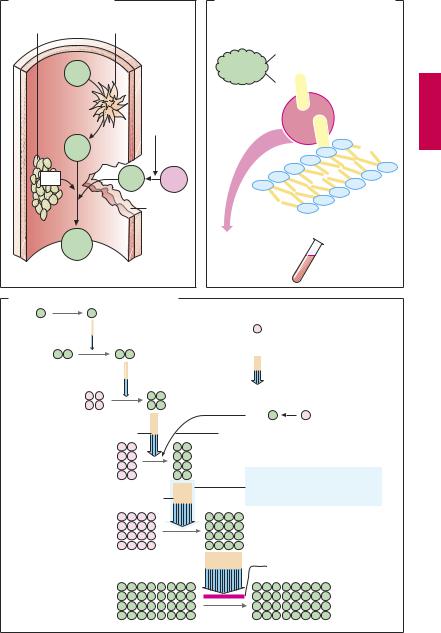
Upon vascular injury, the coagulation system is activated: thrombocytes and fibrin molecules coalesce into a “plug” that seals the defect and halts bleeding (hemostasis). Unnecessary formation of an intravascular clot—a thrombosis—can be life-threatening. If the clot forms on an atheromatous plaque in a coronary artery, myocardial infarction is imminent; a thrombus in a deep leg vein can be dislodged and carried into a lung artery and can cause pulmonary embolism.
Drugs that decrease the coagulability of blood, such as coumarins and heparin (A) are employed for the prophylaxis of thromboses. In addition, attempts are directed, by means of acetylsalicylic acid, at inhibiting the aggregation of blood platelets, which are prominently involved in intra-ar- terial thrombogenesis (p.152). For the therapy of thrombosis, drugs are used that dissolve the fibrin meshwork—fibrinolytics (p.150).
An overview of the coagulation cascade and sites of action for coumarins and heparin is shown in (A). There are two ways to initiate the cascade (B): (1) conversion of factor XII into its active form (XIIa, intrinsic system) at intravascular sites denuded of endothelium; (2) conversion of factor VII into VIIa (extrinsic system) under the influence of a tissue-derived lipoprotein (tissue thromboplastin). Both mechanisms converge via factor X into a common final pathway.
The clotting factors are protein molecules. “Activation” mostly means proteolysis (cleavage of protein fragments) and, with the exception of fibrin, conversion into proteinhydrolyzing enzymes (proteases). Some activated factors require the presence of phospholipids (PL) and Ca2+ for their proteolytic activity. Conceivably, Ca2+ ions cause the adhesion of factor to a phospholipid surface, as depicted in (B). Phospholipids are contained in platelet factor 3 (PF3), which is released from aggregated platelets, and in tissue
thromboplastin (A). The sequential activation of several enzymes allows the aforementioned reactions to “snowball” (symbolized in C by increasing number of particles), culminating in massive production of fibrin.
Ca2+-chelators (B) prevent the enzymatic activity of Ca2+-dependent factors; they contain COO– groups that bind Ca2+ ions (C): citrate and EDTA (ethylenediaminetetraacetic acid) form soluble complexes with Ca2+; oxalate precipitates Ca2+ as insoluble calcium oxalate. Chelation of Ca2+ cannot be used in vivo for therapeutic purposes because Ca2+ concentrations would have to be lowered to a level incompatible with life (hypocalcemic tetany). These compounds (sodium salts) are, therefore, used only for rendering blood incoagulable outside the body. This effect can be reversed at any time by addition of Ca2+ ions.
In vivo, the progression of the coagulation cascade can be inhibited as follows (C):
1.Coumarin derivatives decrease the blood concentrations of inactive factors II, VII, IX and X, by inhibiting their synthesis in the liver.
2.The complex consisting of heparin and antithrombin III neutralizes the protease activity of activated factors; unlike unfractionated heparin, low-molecular-weight heparin fragments or the “minimal molecular subunit of heparin,” fondaparinux, inhibit only activated factor Xa when complexed with antithrombin III.
3.Hirudin and its derivatives (bivalirudin, lepirudin) block the active center of thrombin.
Prophylaxis and Therapy of Thromboses |
145 |
A. Activation of clotting |
|
|
B. Inhibition of clotting by removal of Ca2+ |
|
Platelets |
Endothelial defect |
Clotting factor |
|
|
|
|
|
|
|
|
|
|
COO– |
|
XII |
|
|
COO– |
|
|
|
|
|
|
|
|
Tissue |
+ |
+ |
|
|
kinase |
Ca |
|
|
|
thrombo- |
|
|
XIIa |
|
|
|
– |
|
|
– |
– |
|
|
|
|
|
|
|
|
|
– |
|
PF3 |
VIIa |
VII |
– |
|
|
|
|
– |
|
|
|
Vessel |
|
Phospholipids, |
|
|
rupture |
|
|
|
|
|
e.g., PF3 |
|
|
|
|
|
|
Fibrin |
|
|
Ca2+ chelation |
|
|
|
|
Citrate |
only in vitro |
|
|
|
EDTA |
|
|
|
|
|
|
|
|
|
Oxalate |
|
C. Inhibition of clotting cascade in vivo |
|
|
||
XII |
XIIa |
|
|
|
|
|
Synthesis susceptible to |
|
|
|
inhibition by coumarins |
XI |
XIa |
|
Reaction susceptible to |
|
|
|
|
|
|
|
inhibition by heparin– |
|
|
|
antithrombin complex |
|
IX |
IXa |
|
|
|
VIIa |
VII |
|
VIII + Ca2+ + Pl |
Ca2+ + Pl (phospholipids) |
|
|
X |
Xa |
|
|
|
Susceptible to inhibition also |
|
|
|
by low-molecular-weight |
|
|
V + Ca2+ + Pl |
heparin and fondaparinux |
|
|
Prothrombin II |
IIa Thrombin |
|
|
|
|
Hirudin |
|
Fibrinogen I |
|
Ia Fibrin |

146 Antithrombotics
VitaminKAntagonistsand VitaminK
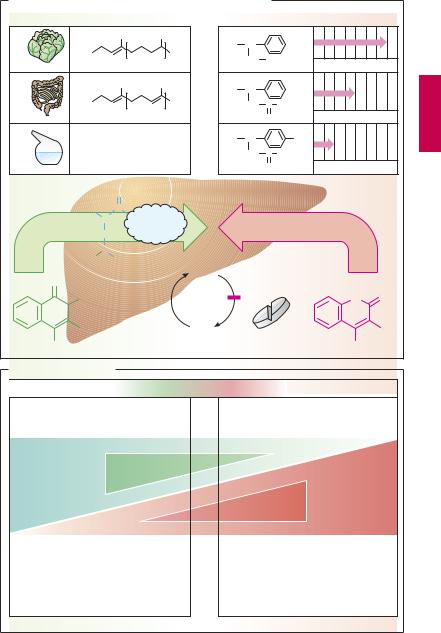
Vitamin K promotes the hepatic γ-carboxy- lation of glutamate residues on the precursors of factors II, VII, IX, and X. Carboxyl groups are required for Ca2+-mediated binding to phospholipid surfaces (p.144). There are several vitamin K derivatives of different origins: K1 (phytomenadione) from chlorophyllous plants; K2 from gut bacteria; and K3 (menadione) synthesized chemically. All are hydrophobic and require bile acids for absorption.
Oral anticoagulants. Structurally related to vitamin K, 4-hydroxycoumarins act as ”false” vitamin K and prevent regeneration of reduced (active) vitamin K from vitamin K epoxide, hence the synthesis of vitamin K- dependent clotting factors
Coumarins are well absorbed after oral administration. Their duration of action varies considerably. Synthesis of clotting factors depends on the intrahepatocytic concentration ratio between coumarins and vitamin K. The dose required for an adequate anticoagulant effect must be determined individually for each patient (monitoring of the International Normalized Ratio, INR).
Indications. Hydroxycoumarins are used for the prophylaxis of thromboembolism as, for instance, in atrial fibrillation or after heart valve replacement.
The most important adverse effect is bleeding. With coumarins, this can be counteracted by giving vitamin K1. However, coagulability of blood returns to normal only after hours or days, when the liver has resumed synthesis and restored suf cient blood levels of carboxylated clotting factors. In urgent cases, deficient factors must be replenished directly (e.g., by transfusion of whole bloodor ofprothrombin concentrate).
Other notable adverse effects include: at the start of therapy, hemorrhagic skin necroses and alopecia; with exposure in utero, disturbances of fetal cartilage and bone for-
mation and CNS injury (due to bleeding); enhanced risk of retroplacental bleeding.
Possibilities for Interference (B)
Adjusting the dosage of a hydroxycoumarin calls for a delicate balance between the opposing risks of bleeding (effect too strong) and of thrombosis (effect too weak). After the dosage has been titrated successfully, loss of control may occur if certain interfering factorsare ignored. If the patientchanges dietary habits and consumes more vegetables, vitamin K may predominate over the vitamin K antagonist. If vitamin K-producing gut flora is damaged in the course of antibiotic therapy, the antagonist may prevail. Drugs that increase hepatic biotransformation via enzyme induction (p.38) may accelerate elimination of a hydroxycoumarin and thus lower its blood level. Inhibitors of hepatic biotransformation (e.g., the H2 blocker cimetidine) augment the action of hydroxycoumarins. Apart from pharmacokinetic alterations, pharmacodynamic interactions must be taken into account. Thus, acetylsalicylic acid is contraindicated because (a) it retards hemostasis by inhibiting platelet aggregation and (b) itmaycause damage tothe gastric mucosawith erosion of blood vessels.
Vitamin K Antagonists and Vitamin K |
147 |
A. Vitamin K-antagonists of the coumarin type and vitamin K |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
Duration of action/days |
||
|
|
|
CH3 |
|
CH3 |
R = |
CH |
|
|
|
|
|
|
R = |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
CH3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CH2 |
CH3 |
|
|
|
||
Vit. K1 |
Phytomenadione |
3 |
|
Phenprocoumon |
||||||||
|
|
|
|
|
||||||||
|
|
|
CH3 |
|
CH3 |
R = |
CH |
|
|
|
|
|
|
R = |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
CH3 |
|
CH2 |
C |
CH3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Vit. K2 |
|
|
|
|
1 – 12 |
|
|
O |
|
Warfarin |
|
|
|
|
|
|
|
|
|
|
|
||||
|
R = H |
|
|
|
|
R = |
CH |
|
|
NO2 |
|
|
|
|
|
|
|
|
CH2 C CH3 |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||
Vit. K3 |
Menadione |
|
|
|
|
O |
|
Acenocoumarol |
||||
|
|
|
O |
Carboxylation of glutamine residues |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
H2N |
CH |
C |
|
|
|
|
|
|
|
|
|
|
|
II, VII, IX, X |
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||
|
|
CH2 |
|
|
|
|
|
|
|
|
|
|
|
HOOC |
CH |
|
|
|
|
|
|
|
|
|
|
|
|
COOH |
|
Vit. K- |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
O |
|
|
|
|
|
Epoxid |
|
|
|
|
|
|
|
CH3 |
|
|
|
|
|
|
|
|
|
O |
O |
|
R |
|
|
|
|
Vit. K |
4-Hydroxy- |
|
|
R |
||
OH |
|
|
|
|
|
|
|
OH |
|
|||
Vit. K derivates |
|
|
coumarin derivatives |
|
||||||||
B. Possible interactions
Risk of thrombosis |
Optimal adjustment |
Risk of bleeding |
|
|
|
Increased intake of vitamin K-rich food
Increase
Vitamin K effect
Decrease
Inhibition of enteral coumarin absorption by adsorbents, e.g., antacids, medicinal charcoal
Acceleration of hepatic coumarin metabolism: enzyme induction, e.g., by carbamazepine, rifampicin
Damage to vitamin K-producing intestinal bacteria by antibiotics
Decrease
Hydroxycoumarin effect
Increase
Inhibition of hepatic coumarin metabolism, e.g., by cimetidine, metronidazole