


|
|
|
|
Insulin Formulations |
259 |
A. Human insulin |
|
|
|
|
|
B-chain |
|
|
|
Subcutaneous insulin injection |
|
|
Pro Lys Thr |
|
|||
|
|
28 |
29 |
30 |
|
|
|
|
C-terminus |
|
|
|
|
|
|
|
|
S |
S |
|
Asn 21 |
|
|
|
|
A-chain |
|
||
|
|
|
|
|
|
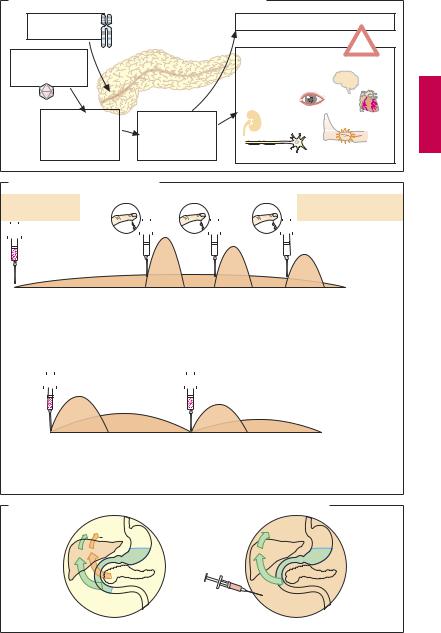
B. Control of release from injection site into bloodstream |
|
|
|
|
|||||||
Human insulin solution |
|
Blood- |
Variation in amino acid sequence |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
stream |
|
|
|
|
|
|
Thr 30 |
|
|
|
|
|
|
|
|
|
|
Thr 30 |
Lys 29 |
|
|
Hexamer |
|
|
|
|
|
|
|
Pro 29 |
Pro 28 |
Insulin |
|
|
|
|
|
|
|
Insulin lispro |
Lys 28 |
|
|
|
Dimers |
|
|
|
|
|
|
|||
|
solution |
|
|
|
|
|
solution |
|
|||
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
No aggregate |
|
||
|
|
Monomers |
|
|
|
|
formation |
|
|
||
|
|
|
|
|
|
|
|
|
|
||
|
Insulin concentration in blood |
|
|
|
Insulin concentration in blood |
|
|||||
0 |
6 |
12 |
18 |
h |
|
0 |
6 |
12 |
18 |
h |
|
Variation in formulation |
|
|
|
Variation in amino acid sequence |
|||||||
Insulin |
|
|
|
|
|
|
|
Precipitation |
Insulin |
Arg 32 |
|
suspension |
|
|
|
|
|
|
of crystals |
glargine |
Arg 31 |
||
|
|
|
|
|
|
|
|
solution |
|||
Crystal |
|
|
|
|
|
|
|
|
|
(pH 4) |
Thr 30 |
|
|
|
|
|
|
|
|
|
|
Lys 29 |
|
formation |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
Pro 28 |
Addition |
|
|
|
|
|
|
|
Tissue |
|
Gly 21 |
|
of zinc ions |
|
Insulin concentration in blood |
(pH 7) |
|
|
||||||
|
|
|
|
|
|
|
|||||
|
|
|
0 |
6 |
12 |
18 |
h |
|
|
|
|

Treatment of IDDM |
261 |
A. Diabetes mellitus type I: pathogenesis and complications |
|
|||
Genetic |
|
Diabetic coma |
|
|
disposition |
|
|
! |
|
Environmental |
|
Diabetic microand |
||
|
|
|||
factors, e.g., |
|
macroangiopathy |
|
|
viral infection |
|
Late organ damage |
Stroke |
|
|
|
Retinopathy |
|
|
Autoimmune |
Absolute insulin |
Nephropathy |
Myocardial |
|
infarction |
||||
destruction of |
deficiency |
|
||
|
|
|||
B-cells in islets |
Hyperglycemia |
|
Peripheral obliterating |
|
of Langerhans |
Neuropathy |
|||
|
|
|
arterial disease |
|
B. Methods of insulin replacement
Extended-action |
Blood glucose measurement |
Rapid-acting insulin: |
insulin |
|
flexible time and dose |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
22 |
|
|
24 |
|
4 |
|
8 |
|
12 |
|
|
|
|
|
|
|
16 |
20 |
22 |
|
||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Breakfast |
|
|
|
|
|
Lunch |
|
|
Dinner |
Food intake: |
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
flexible |
|
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
1. Intensified insulin therapy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Combination |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Insulin administration: |
||||||||||||||
|
insulin |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
fixed schedule |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
|
8 |
|
12 |
|
16 |
|
20 |
|
|
|
|
|
|
|
24 |
4 |
8 |
|
||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Breakfast |
|
|
Lunch |
|
|
|
|
|
|
|
|
|
Dinner |
|
|
|
|
|
|
|
|
|
|
Food intake: |
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
& snacks |
|
|
|
|
|
|
|
|
|
Supper |
|
|
|
|
|
|
|
|
|
|
fixed schedule |
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2.Conventional insulin therapy
C. Presystemic and systemic insulin action in healthy and diabetic subjects
Insulin
Glucose
 Glucose
Glucose
InsulinInsulin
Healthy subject |
Diabetic |