


Drugs for the Treatment of AIDS |
291 |
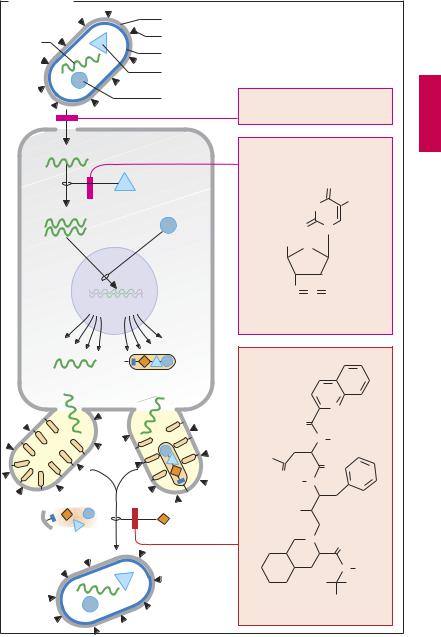
A. AIDS drugs |
|
|
|
|
|
|
Envelope |
|
|
|
|
RNA |
Fusion glycoprotein |
|
|
|
|
|
|
|
|
|
|
|
Matrix protein |
|
|
|
|
|
Reverse |
|
|
|
|
|
transcriptase |
|
|
|
|
|
Integrase |
Fusion inhibitor Enfuvirtide, |
|||
|
|
||||
|
|
a peptide, s.c. administration |
|||
Viral RNA |
|
Inhibitors of |
|
|
|
|
reverse |
|
|
|
|
|
|
|
|
|
|
|
|
transcriptase |
|
|
|
|
|
|
|
|
O |
|
|
|
|
H N |
CH 3 |
DNA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
O |
N |
|
|
|
HOCH2 |
O |
|
|
|
|
|
N |
+ |
N – |
|
|
|
N |
||
|
|
e.g., zidovudine |
|
||
|
|
Inhibitors of |
|
|
|
Viral RNA |
Polyproteins |
HIV protease |
|
|
|
|
|
|
|
||
|
|
|
|
|
N |
|
|
|
O |
|
|
|
|
|
|
N |
H |
|
|
H2N |
|
|
O |
|
|
O |
|
|
|
|
|
H |
N |
|
|
|
|
|
|
||
|
Protease |
HO |
|
|
|
|
|
|
|
|
|
Polyprotein |
|
|
|
N |
O |
cleavage |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
N H |
|
|
|
|
H3C |
CH3 |
|
Mature virus |
e.g., saquinavir |
CH3 |
||
|
|
||||


|
Drugs against Endoand Ectoparasites |
293 |
A. Endoparasites and ectoparasites: therapeutic agents |
|
|
Tapeworms |
Louse |
|
e.g., beef |
|
|
tapeworm |
|
|
Spasm, |
|
|
|
|
|
|
Cl |
|
|
injury of |
|
|
|
|
|
|
|
|
|
integument |
|
|
|
|
|
|
|
|
|
O |
C |
|
|
|
|
Chlor- |
|
Cl |
|
|
N |
|
|
|
|
HC |
C |
Cl |
|
|
|
|
|
|
phenothane |
||||
|
N |
|
|
|
|
(DDT) |
|
Cl |
|
|
|
O |
|
|
death |
|
|
|
|
|
|
|
Praziquantel |
Cl |
|
|
|||
|
|
|
|
|
|
||||
|
|
|
|
|
|
convulsions, |
|
|
|
Round- |
|
|
|
|
|
|
|
|
|
worms, |
|
|
|
|
|
|
|
|
|
e.g., |
|
|
|
|
|
system:nervousto |
|
|
|
ascaris |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pinworm |
|
|
Flea |
|
|
|
|
O |
|
|
|
|
|
Damage |
Cl |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
Cl |
|
|
Cl |
|
C |
|
|
|
|
|
|
|
||
|
|
NH |
|
|
|
|
|
|
|
|
|
N |
NH |
COOC |
3 |
Cl |
|
|
Cl |
|
|
|
|
Cl |
|
|
|||
|
|
|
|
H |
|
|
|
|
|
|
|
|
|
|
|
Hexachlorocyclo- |
|||
Mebendazole |
|
|
|
|
hexane (Lindane) |
||||
Trichinella |
|
larvae |
Scabies mite |