


156 Plasma Volume Expanders
Plasma Volume Expanders
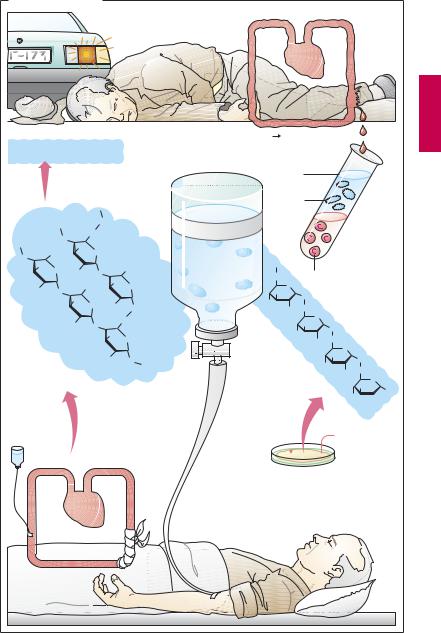
Major blood loss entails the danger of lifethreatening circulatory failure, i.e., hypovolemic shock. The immediate threat results not so much from the loss of erythrocytes, i.e., oxygen carriers, as from the reduction in volume of circulating blood.
To eliminate the threat of shock, replenishment of the circulation is essential. With moderate loss of blood, administration of a plasma volume expander may be suf cient. Blood plasma consists basically of water, electrolytes, and plasma proteins. However, aplasmasubstitute neednotcontain plasma proteins. These can be suitably replaced with macromolecules (“colloids”) that, like plasma proteins, (1) do not readily leave the circulation and are poorly filtrable in the renal glomerulus; and (2) bind water along with its solutes owing to their colloid osmotic properties. In this manner, they will maintain circulatory filling pressure for many hours. On the other hand, complete elimination of these colloids from the body is clearly desirable.
Compared with whole blood or plasma, plasma substitutes offer several advantages: they can be produced more easily and at lower cost, have a longer shelf-life, and are free ofpathogens such ashepatitis Band C or AIDS viruses.
Three colloids are currently employed as plasma volume expanders—the two polysaccharides dextran and hydroxyethyl starch, and the polypeptide gelatin.
Dextran is a polymer formed by bacteria and consisting of atypically linked (1†6 instead of 1†4 bond) glucose molecules. Commercially available plasma substitutes contain dextran of a mean molecular weight (MW) of 70 or 75 kDa (dextran 70 or 75) or 40 kDa (dextran 40 or low-molecular- weight dextran). The chain length of single molecules varies widely, however. Smaller dextran molecules can be filtered at the glomerulus and slowly excreted in urine; the larger ones are eventually taken up and de-
graded by cells of the mononuclear phagocyte system. Apart from restoring blood volume, dextran solutions are used for hemodilution in the management of blood flow disorders.
As for microcirculatory improvement, it is occasionally emphasized that low -molecu- lar-weight dextran, unlike dextran 70, may directly reduce the aggregability of erythrocytes by wayof altering their surface properties. With prolonged use, larger molecules will accumulate owing to the more rapid renal excretion of the smaller ones. Consequently, the molecular weight of dextran circulating in blood will tend toward a higher mean molecular weight with the passage of time.
The most important adverse effect results fromthe antigenicityofdextrans,whichmay lead to an anaphylactoid reaction. Dextran antibodies can be intercepted without an immune response by injection of small dextran molecules (MW 1000), thus obviating any incompatibility reaction to subsequent infusion of the dextran plasma substitute solution.
Hydroxyethyl starch (hetastarch) is produced from starch. By virtue of its hydroxyethyl groups, it is metabolized more slowly and retained significantly longer in blood than would be the case with infused starch. Hydroxyethyl starch resembles dextrans in terms of its pharmacological properties and therapeutic applications. A particular adverse effect ispruritus of prolonged duration with deposition of the drug in peripheral nerves.
Gelatin colloids consist of cross-linked peptide chains obtained from collagen. They are employed for blood replacement but not for hemodilution in circulatory disturbances.
Plasma Volume Expanders |
157 |
A. Plasma subtitutes
Circulation
Gelatin colloids
=cross-linked peptide chains MW 35 000
Peptides |
MW ~ 15 000 |
|
|
|
Gelatin |
MW ~100 000 |
|
|
|
Collagen MW ~300 000 |
|
|
||
|
|
|
O |
|
|
O |
CH2 |
|
|
|
|
|
|
|
|
OH |
|
|
|
O |
CH2OH |
O |
|
|
OH |
|
|
CH2OH |
|
|
O HO |
O |
||
|
|
|
OH |
|
RO |
O |
CH2OH |
O |
|
|
OH |
O RO |
|
|
|
|
O |
||
|
|
|
|
|
|
RO |
O |
|
CH2 |
|
|
|
||
|
|
OH |
|
|
|
|
|
O |
|
|
|
|
|
|
R = HO–CH2–CH2– |
|
|
|
|
Hydroxyethyl starch |
RO |
O |
||
|
||||
(hetastarch)
mean MW 670 000
Hydroxyethylation starch
Blood loss |
Danger of shock |
|
Plasma |
|
Plasma- |
|
proteins |
Plasma- |
|
substitute |
|
with colloids |
CH2 |
O
OH |
O |
|
HO |
||
CH2 |
||
OH |
||
|
OH
HO
Dextran
MW 70 000
MW 40 000
Sucrose 
Erythrocytes
O
|
O |
|
|
OH |
CH2 |
|
|
O |
|
|
|
|
|
|
|
|
OH |
O |
|
|
|
|
|
HO |
|
6 |
|
OH |
CH2 |
|
|
|
|
||
|
5 |
O |
|
|
|
||
|
4 OH |
1 |
|
3 O HO 

OH
 Fructose
Fructose
Bacterium
Leuconostoc mesenteroides

158 Drugs Used in Hyperlipoproteinemias
Lipid-lowering Agents
Triglycerides and cholesterol are essential constituents of the organism. Among other things, triglycerides represent a form of energy store and cholesterol is a basic building block of biological membranes. Both lipids are water insoluble and require appropriate “packaging” for transport in the aqueous media of lymph and blood. To this end, small amounts of lipid are coated with a layer of phospholipids, embedded in which are additional proteins—the apolipoproteins (A). According to the amount and the composition of stored lipids, as well as the type of apolipoprotein, one distinguishes four transport forms (see table).
other tissues with fatty acids. Left behind are LDL particles that either return into the liver or supply extrahepatic tissues with cholesterol.
LDL particles carry the apolipoprotein B- 100, by which they are bound to receptors that mediate uptake of LDL into the cells, including the hepatocytes (receptor-medi- ated endocytosis, p.26).
HDL particles are able to transfer cholesterol from tissue cells to LDL particles. In this way, cholesterol is transported from tissues to the liver.
Hyperlipoproteinemias can be caused genetically (primary hyperlipoproteinemia) or can occur in obesity and metabolic disorders (secondary hyperlipoproteinemia). Ele-
|
Origin |
Density (g/ml) |
Mean time in |
Diameter (nm) |
|
|
|
blood plasma (h) |
|
|
|
|
|
|
Chylomicron |
Gut epithelium |
> 1.006 |
0.2 |
500 or more |
|
|
|
|
|
VLDL particle |
Liver |
0.95–1.006 |
3 |
100–200 |
|
|
|
|
|
LDL particle |
(Blood) |
1.006–1.063 |
50 |
25 |
|
|
|
|
|
HDL particle |
Liver |
1.063–1.210 |
— |
5–10 |
|
|
|
|
|
Lipoprotein metabolism. Enterocytes release absorbed lipids in the form of trigly- ceride-rich chylomicrons. Bypassing the liver, these enter the circulation mainly via the lymph and are hydrolyzed by extrahepatic endothelial lipoprotein lipases to liberate fatty acids. The remnant particles move on into liver cells and supply these with cholesterol of dietary origin.
The liver meets the larger part (60%) of its requirement for cholesterol by synthesis de novo from acetyl-coenzyme A. Synthesis rate is regulated at the step leading from hydroxymethylglutaryl-CoA (HMG-CoA) to mevalonic acid (p.161A), with HMG-CoA reductase as the rate-limiting enzyme.
The liver requires cholesterol for synthesizing VLDL particles and bile acids. Trigly- ceride-rich VLDL particles are released into the blood and, like the chylomicrons, supply
vated LDL-cholesterol serum concentrations are associated with an increased risk of atherosclerosis, especially when there is a concomitant decline in HDL concentration (increase in LDL : HDL quotient).
Treatment. Various drugs are available that have different mechanisms of action and effects on LDL (cholesterol) and VLDL (triglycerides) (A). Their use is indicated in the therapy of primary hyperlipoproteinemias. In secondary hyperlipoproteinemias, the immediate goal should be to lower lipoprotein levels by dietary restriction, treatment of the primary disease, or both.
Lipid-lowering Agents |
159 |
A. Lipoprotein metabolism |
|
|
|
|
|
||
Dietary fats |
|
|
|
Cell metabolism |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
Cholesterol |
|
Chylomicron |
|
|
|
LDL |
|
|
|
|
Fat tissue |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HDL |
|
|
|
|
Heart |
|
|
|
|
|
|
Skeletal muscle |
|
|
|
|
|
|
|
|
|
|
VLDL |
HDL |
LDL |
Chylomicron |
|
Lipoprotein |
|
|
Cholesterol |
|
|
remnant |
|
synthesis |
|
|
|
|
|
|
|
|
|
|
Triglycerides |
|
|
|
|
Cholesterol- |
|
|
|
|
|
|
|
ester |
|
|
|
|
|
|
|
Triglycerides |
|
|
|
|
|
Cholesterol |
cell |
|
|
|
Cholesterol |
|
|
|
|
|
|
|
|
||
Liver |
|
|
|
|
|
|
|
Fatty acids |
Apolipo- |
|
|
|
|
|
|
Lipoprotein |
protein |
OH |
|
OH |
|
|
|
|
OH |
|
|
||||
Lipase |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B. Cholesterol metabolism in liver cell and cholesterol-lowering drugs
Colestyramine |
|
Gut: binding |
Bile acids |
and |
|
excretion |
|
of bile |
|
acids (BA) |
|
Liver: |
|
BA synthesis |
|
Cholesterol |
|
consumption |
|
Ezetimib
Gut: Cholesterol absorption
Cholesterol store
Synthesis
Lipoproteins
Liver cell
LDL
HMG-CoA-Reductase inhibitors

160 Drugs Used in Hyperlipoproteinemias
Drugs. As nonabsorbable anion-exchange resins, colestyramine and colestipol can bind bile acids in the gut lumen, which are thus removed from cholesterol metabolism. The required dosage is rather high (15–30 g/day) and liable to produce gastrointestinal disturbances. Consequently, patient compliance is low. Moreover, the resins trap needed drugs and vitamins. A more promising approach to lowering absorption of cholesterol derives from a novel mechanism of action probably based on the specific inhibition of intestinal cholesterol transporters that are required for absorption of cholesterol. An inhibitor of this type is ezetimibe.
β-Sitosterin is a plant steroid that is not absorbed after oral administration; in suf - ciently high dosage it impedes enteral absorption of cholesterol. Treatment with sitosterin has become obsolete. The drug is no longer on the market.
The statins lovastatin and fluvastatin inhibit HMG-CoA reductase. They contain a molecular moiety that chemically resembles the physiological substrate of the enzyme (A). Lovastatin is a lactone that is rapidly absorbed by the enteral route, subjected to extensive first-pass extraction in the liver, and there hydrolyzed to active metabolites. Fluvastatin represents the active form and, as an acid, is actively transported by a specific anion carrier that moves bile acids from blood into liver and also mediates the selective uptake of the mycotoxin amanitin (A). Normally viewed as presystemic elimination, ef cient hepatic extraction serves to confine the action of statins to the liver. Despite the inhibition of HMG-CoA reductase, hepatic cholesterol content does not fall because hepatocytes compensate any drop in cholesterollevelsby increasing the synthesis of LDL receptor protein (along with the reductase). Since,in the presenceofstatins,the newly-formed reductase is inhibited as well, the hepatocyte must meet its cholesterol demand entirely by uptake of LDL from the blood (B). Accordingly, the concentration of circulating LDL falls. As LDL remains in blood
forashorter time,the likelihoodofLDLbeing oxidized to its proatherogenic degradation product decreases pari passu.
Other statins include simvastatin (also a lactone prodrug), pravastatin, atorvastatin, and cerivastatin (active formwithopenring). The statins are the most important therapeutics for lowering cholesterol levels. Their notable cardiovascular protective effect, however, appears to involve additional actions.
The combination of a statin with an inhibitor of cholesterol absorption (e.g., ezetimibe) can lower LDL levels even further.
A rare but dangerous adverse effect of statins is damage to skeletal muscle (rhabdomyolysis). This risk is increased by combined use of fibric acid agents (see below). Cerivastatin has proved particularly toxic. Besides muscle damage associated with myoglobinuria and renal failure, severe hepatotoxicity has also been noted, prompting withdrawal of the drug.
Nicotinic acid and its derivatives (pyridylcarbinol, xanthinol nicotinate, and acipimox) activate endothelial lipoprotein lipase and thereby mainly lower triglyceride levels. At the start of therapy, a prostaglandin-medi- ated vasodilation occurs (flushing, hypotension) that can be prevented by low doses of acetylsalicylic acid.
Clofibrate and derivatives (bezafibrate, fenofibrate, and gemfibrozil) lower concentrations of VLDL (triglycerides) along with LDL (cholesterol). They may cause damage to liver and skeletal muscle (myalgia, myopathy, rhabdomyolysis with myoglobinemia and renal failure). The mechanism of action of fibrates is not completely understood. They bind to a peroxisome proliferator-activated receptor (PPARα) and thereby influence genes regulating lipid metabolism.

Lipid-lowering Agents |
161 |
A. Accumulation and effect of HMG-CoA reductase inhibitors in liver |
|
||||||
|
|
Low systemic availability |
|
||||
|
|
3-Hydroxy-3-methyl- |
Mevalonate |
|
|||
|
|
glutaryl-CoA |
|
HO |
COO– |
|
|
|
|
HO |
|
|
|
||
|
|
COO– |
|
|
CH3 |
|
|
|
|
CH3 |
|
|
|
OH |
|
|
|
|
O |
|
|
|
|
|
|
SCoA HMG-CoA- |
Cholesterol |
|
|||
|
|
|
Reductase |
|
|||
|
|
Bio- |
HO |
COO– |
|
|
|
|
|
|
OH |
|
|
|
|
|
|
activation |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R Active form |
|
||
|
|
Extraction |
|
|
|
Active |
|
|
|
of lipophilic |
|
|
|
uptake of |
|
|
|
lactone |
|
|
|
anion |
|
|
|
|
|
|
|
HO |
|
|
HO |
O |
|
|
|
COO– |
|
|
|
|
|
OH |
|
||
|
|
O |
|
|
|
|
|
|
O |
|
|
|
|
|
|
|
|
|
|
|
F |
|
|
|
|
|
Oral |
|
|
CH3 |
|
H3C |
O |
|
|
|
|
||
CH3 |
administration |
N |
CH3 |
||||
|
H3C |
|
|
|
|||
|
H3C |
Lovastatin |
|
Fluvastatin |
|
||
|
|
|
|
||||
B.Regulation by cellular cholesterol concentration of HMG-CoA reductase and LDL-receptors
Inhibition of
HMG-CoA reductase
LDL- |
|
|
Receptor |
|
|
HMG-CoA |
Gene |
Gene |
reductase |
expression |
expression |
|
Cholesterol |
|
LDL |
|
Increased receptor- |
|
mediated uptake of LDL |
|
in blood |
|
|